
Infectious syphilis and congenital syphilis in Canada, 2023

 Download this article as a PDF (463 KB)
Download this article as a PDF (463 KB)Published by: The Public Health Agency of Canada
Issue: Volume 51-2/3, February/March 2025: Health Economics in Public Health
Date published: February 2025
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 51-2/3, February/March 2025: Health Economics in Public Health
Infographic
Text description: Infographic
Infectious syphilis and congenital syphilis in Canada, 2023Note *
Social and structural determinants of health and health inequities play a role in the differences in rates of syphilis across different populationsNote ‡‡.
Syphilis screening and timely treatment are essential to prevent transmission and complications. Find the Public Health Agency of Canada (PHAC)’s recently updated syphilis screening recommendations in the Syphilis Guide: Screening and diagnostic testing, as part of PHAC’s Sexually transmitted and blood-borne infections (STBBI): Guides for Health Professionals.
Infectious syphilis
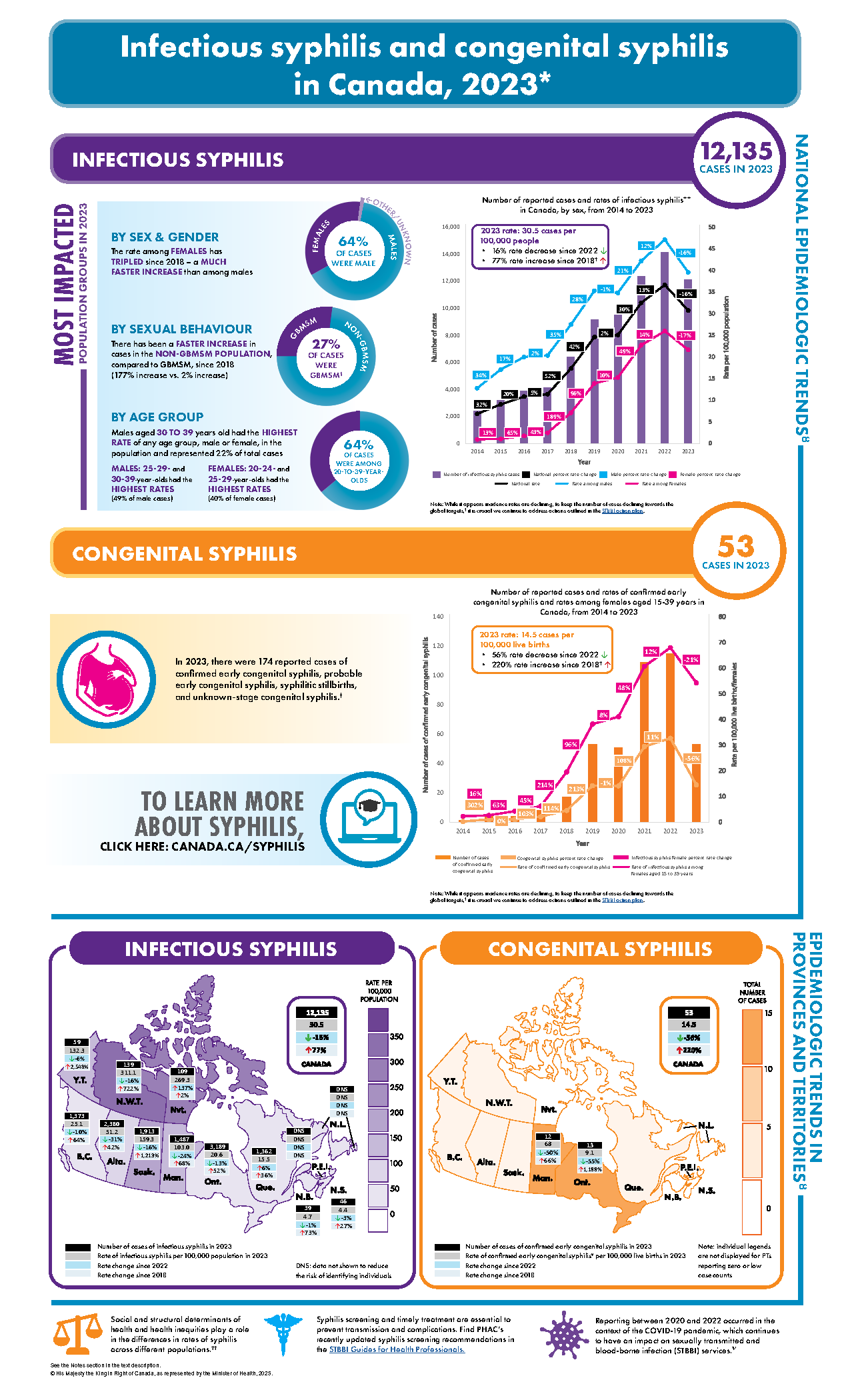
In 2023, there were 12,135 cases of infectious syphilisNote ** reported nationally, for a rate of 30.5 cases per 100,000 population. The 2023 national rate of infectious syphilis was:
- 16% lower than the 2022 rate
- 77% higher than the 2018Note ┼ rate
It is the first year since 2014 that the national number of cases and rate of infectious syphilis have decreased. However, data for 2023 alone cannot be viewed as a trend and must be interpreted with caution. Future data collection is needed to determine if a downward trend in infectious syphilis rates is being establishedNote ѱ.
The national reported rate of infectious syphilis increased by 32% from 2014 to 2015 and by 20% from 2015 to 2016. The rate remained relatively stable from 2016 to 2017, with a 5% increase. Substantial increases in the national reported rate of infectious syphilis were seen in subsequent yearsNote ४:
- From 2017 to 2018, an increase of 52%
- From 2018 to 2019, an increase of 42%
- From 2019 to 2020, a relatively stable rate, with an increase of 2%Note ѱ
- From 2020 to 2021, an increase of 30%Note ѱ
- From 2021 to 2022, an increase of 13%Note ѱ
Trends by sex
Nationally, 64% of cases reported in 2023 occurred among males, with a male-to-female ratio of 1.8. In comparison, in 2018, 79% of cases occurred among males, with a male-to-female ratio of 3.8 (see Appendix A, Table 5, for trends by gender).
- In 2023, the national reported rate of infectious syphilis increased by 204% in females and by 43% in males, compared to 2018
| Year | Number of cases among males | Number of cases among females | Total number of cases | Total rate per 100,000 population | Rate per 100,000 males | Rate per 100,000 females | Total percentage rate change | Percentage rate change among males | Percentage rate change among females |
|---|---|---|---|---|---|---|---|---|---|
| 2014 | 2,232 | 164 | 2,399 | 6.8 | 12.7 | 0.9 | NC | NC | NC |
| 2015 | 3,008 | 187 | 3,200 | 9.0 | 17.0 | 1.0 | 32.3% | 33.7% | 13.1% |
| 2016 | 3,551 | 311 | 3,877 | 10.8 | 19.9 | 1.7 | 19.9% | 16.9% | 64.6% |
| 2017 | 3,664 | 449 | 4,130 | 11.3 | 20.3 | 2.4 | 5.3% | 1.9% | 42.8% |
| 2018 | 5,022 | 1,315 | 6,371 | 17.3 | 27.4 | 7.1 | 52.1% | 35.1% | 189.1% |
| 2019 | 6,544 | 2,607 | 9,176 | 24.5 | 35.2 | 13.8 | 42.0% | 28.3% | 95.6% |
| 2020 | 6,564 | 2,902 | 9,498 | 25.0 | 34.7 | 15.2 | 2.0% | −1.3% | 9.7% |
| 2021 | 7,989 | 4,343 | 12,378 | 32.5 | 42.1 | 22.7 | 29.9% | 21.2% | 49.2% |
| 2022 | 9,045 | 5,031 | 14,135 | 36.5 | 47.0 | 25.9 | 12.6% | 11.6% | 14.3% |
| 2023 | 7,784 | 4,284 | 12,135 | 30.5 | 39.3 | 21.5 | −16.4% | −16.3% | −17.0% |
Abbreviation: NC, non-computable (rate change not computable due to a denominator of 0) Notes: Total number of national cases and rates include reported cases among all sexes. The percentage rate change refers to the proportional increase or decrease in rate relative to the previous year |
|||||||||
Trends by sex and age group
In 2023, national reported rates of infectious syphilis were highest in the 20- to 39-year age group (see Appendix A, Table 6 and Table 7). The rates were highest:
- In the 25–29- and 30–39-year age group for males
- In the 20–24- and 25–29-year age group for females
In 2023, males aged 30–39 years had the highest national rate of infectious syphilis of any age group, male or female, at 90.4 cases per 100,000 males aged 30–39 years. Followed closely were males aged 25–29 years, with a rate of 81.7 cases per 100,000 males aged 25–29 years.
- Rates in 2023 increased relative to 2018 across all age groups, with the highest rate increases occurring among 30–39- (46%) and 40–59-year-olds (67%)
- Rates in 2023 decreased relative to 2022 among most age groups, with the highest rate decreases occurring among 15–19- (24%) and 20–24-year-olds (21%)
- The rate in 2023 among those under 15 years increased by 32% relative to 2022
Among females, those aged 20–24 years had the highest national rate of infectious syphilis, at 67.4 cases per 100,000 females aged 20–24 years, followed by those aged 25–29 years, with a rate of 66.2 cases per 100,000 females aged 25–29 years.
- Rates in 2023 increased relative to 2018 among all age groups, with the highest rate increases occurring among 30–39- (243%) and 40–59-year-olds (444%)
- Rates in 2023 decreased relative to 2022 among most age groups, with the highest rate decreases occurring among 25–29- (22%) and 30–39-year-olds (23%)
- The rate in 2023 among those over 60 years increased by 24% relative to 2022
Trends by sexual behaviour
Cases of infectious syphilis reported among cisgender gay, bisexual and other men who have sex with men (GBMSM)§ represented 27% of all reported cases in 2023 (see Appendix A, Table 8).
- GBMSM represented 42% of total reported male cases in 2023, a 1% increase from 2022 and a 37% decrease from 2018
- The number of reported cases among GBMSM has remained relatively stable throughout time, even as the proportion of cases among GBMSM relative to cases in the total population (combined infectious syphilis cases among males, females, etc.) has decreased
Trends by province and territory
- Between 2014 and 2022, there was an upward trend in the reported number of cases and rates of infectious syphilis across all provinces and territories. However, 2023 has been characterized by non-uniform changes in case counts and rates across jurisdictions. Provincial and territorial data in 2023 are as follows:
- Rates in 2023 decreased relative to 2022 in most provinces and territories, with the highest rate decreases occurring in Alberta and Manitoba (31% and 24%, respectively)
- Rates in 2023 increased relative to 2022 in Newfoundland and Labrador, Nunavut and Québec (data not shown [DNS] to reduce the risk of identifying individuals, 137% and 6%, respectively)
- In 2023, the highest number of reported cases of infectious syphilis occurred in Ontario (n=3,189), followed by Alberta (n=2,380), Saskatchewan (n=1,913) and Manitoba (n=1,487)
- Provinces and territories that reported rates of infectious syphilis higher than the national rate of 30.5 cases per 100,000 population included:
- Northwest Territories (311.1 cases per 100,000 population)
- Nunavut (269.3 cases per 100,000 population)
- Saskatchewan (159.3 cases per 100,000 population)
- Yukon (132.3 cases per 100,000 population)
- Manitoba (103.0 cases per 100,000 population)
- Alberta (51.2 cases per 100,000 population)
- Provinces and territories that reported rates of infectious syphilis lower than the national rate of 30.5 cases per 100,000 population included:
- British Columbia (25.1 cases per 100,000 population)
- Ontario (20.6 cases per 100,000 population)
- Québec (15.5 cases per 100,000 population)
- Newfoundland and Labrador (DNS)
- New Brunswick (4.7 cases per 100,000 population)
- Nova Scotia (4.4 cases per 100,000 population)
- Prince Edward Island (DNS)
| Province or territory | Number of cases | Rate per 100,000 population, 2023 | Change in rate since 2022 | Change in rate since 2018 |
|---|---|---|---|---|
| British Columbia | 1,373 | 25.1 | ↓−9.6% | ↑63.7% |
| Alberta | 2,380 | 51.2 | ↓−31.0% | ↑41.8% |
| Saskatchewan | 1,913 | 159.3 | ↓−15.7% | ↑1,212.9% |
| Manitoba | 1,487 | 103.0 | ↓−24.3% | ↑68.3% |
| Ontario | 3,189 | 20.6 | ↓−13.0% | ↑52.1% |
| Québec | 1,362 | 15.5 | ↑5.9% | ↑36.2% |
| New Brunswick | 39 | 4.7 | ↓−0.5% | ↑72.7% |
| Nova Scotia | 46 | 4.4 | ↓−3.1% | ↑27.4% |
| Prince Edward Island | DNS | DNS | DNS | DNS |
| Newfoundland and Labrador | DNS | DNS | DNS | DNS |
| Yukon | 59 | 132.3 | ↓5.8% | ↑2,548.4% |
| Northwest Territories | 139 | 311.1 | ↓−16.0% | ↑722.3% |
| Nunavut | 109 | 269.3 | ↑137.0% | ↑2.3% |
| Canada | 12,135 | 30.5 | ↓−16.4% | ↑76.9% |
Abbreviation: DNS, data not shown to reduce the risk of identifying individuals |
||||
Trends by sex and by province and territory
In 2023, the proportion of males with infectious syphilis, relative to females, varied across provinces and territories (see Appendix A, Table 9).
- Provinces and territories that reported a male-to-female rate ratio lower than the national ratio of 1.8 or, in other words, had a higher proportion of females impacted than the national average, included:
- Saskatchewan (rate ratio: 0.8)
- Manitoba (rate ratio: 0.9)
- Yukon (rate ratio: 1.0)
- Nunavut (rate ratio: 1.0)
- Northwest Territories (rate ratio: 1.2)
- Alberta (rate ratio: 1.2)
- Prince Edward Island (rate ratio: 1.6)
Congenital syphilis
In 2023, there were 53 cases of confirmed early congenital syphilisNote ╪ reported nationally, for a rate of 14.5 cases per 100,000 live births. The 2023 national rate of confirmed early congenital syphilis was:
- 56% lower than the 2022 rate
- 220% higher than the 2018Note ┼ rate
From 2018 to 2022, national reported rates of confirmed early congenital syphilis increased annually. However, in 2023, the rate decreased, in parallel with the decrease in the reported rate of infectious syphilis among females aged 15–39 years.
As with infectious syphilis, it is the first year since 2014 that the national number of cases and rate of congenital syphilis have substantially decreased. However, data for 2023 alone cannot be viewed as a trend and must be interpreted with caution. Future data collection is needed to determine if a downward trend in congenital syphilis rates is being establishedNote ѱ.
In 2023, following annual increases from 2018 to 2022, the rate of infectious syphilis among females aged 15–39 years decreased.
- The 2023 national reported rate of infectious syphilis among females aged 15–39 years was:
- 21% lower than the 2022 rate
- 176% higher than the 2018 rate
| Year | Total national cases of confirmed early congenital syphilis | Total national cases of probable early congenital syphilis | Total national cases of syphilitic stillbirth | Total national cases of unknown congenital syphilis stage | Rate of confirmed early congenital syphilis per 100,000 live births | Rate of infectious syphilis in women aged 15–39 years per 100,000 females aged 15–39 years |
|---|---|---|---|---|---|---|
| 2014 | 1 | N/A | N/A | N/A | 0.3 | 2.3 |
| 2015 | 4 | N/A | N/A | N/A | 1.0 | 2.6 |
| 2016 | 4 | N/A | N/A | N/A | 1.0 | 4.3 |
| 2017 | 8 | N/A | N/A | N/A | 2.1 | 6.2 |
| 2018 | 17 | 8 | N/A | N/A | 4.5 | 19.5 |
| 2019 | 53 | 10 | N/A | N/A | 14.2 | 38.2 |
| 2020 | 51 | 37 | 22 | 7 | 14.1 | 41.0 |
| 2021 | 109 | 55 | 18 | 7 | 29.4 | 60.6 |
| 2022 | 115 | 114 | 18 | 18 | 32.7 | 67.8 |
| 2023 | 53 | 86 | 16 | 19 | 14.5 | 53.8 |
Abbreviation: N/A, data not available Notes: Not all provinces and territories have a case definition for probable and stillbirth congenital syphilis casesNote ╪ |
||||||
In 2023, there were 174 cases of congenital syphilis, including confirmed early congenital syphilis, probable early congenital syphilis, syphilitic stillbirth and unknown-stage congenital syphilisNote ╪.
Trends by province and territory
Between 2014 and 2022, there was an upward trend in the reported number of cases and rates of congenital syphilis across all provinces and territories. However, in 2023, the reported number of cases of confirmed early congenital syphilis decreased or remained stable across jurisdictions. Provincial and territorial data in 2023 are as follows:
- Rates in 2023 decreased relative to 2022 in British Columbia (24%), Alberta (78%), Saskatchewan (65%), Manitoba (50%) and Ontario (55%). However, an increase in reported case counts was observed in Québec (107%) and Yukon (rate change not computable)
- There were no cases of confirmed early congenital syphilis reported in New Brunswick, Nova Scotia, Prince Edward Island, Newfoundland and Labrador and Nunavut
- Case counts remained stable in the Northwest Territories
- Within the context of decreasing national case counts, the highest number of confirmed early congenital syphilis cases reported, overall, in 2023 occurred in Ontario (n=13; rate=9.1 cases per 100,000 live births, 55% decrease) and Manitoba (n=12; rate=68.0 cases per 100,000 live births, 50% decrease)
- Provinces and territories that reported rates of congenital syphilis higher than the national rate of 14.5 cases per 100,000 live births included:
- Northwest Territories (DNS)
- Yukon (DNS)
- Manitoba (68.0 cases per 100,000 live births)
- Saskatchewan (DNS)
- Alberta (DNS)
- Provinces and territories that reported rates of congenital syphilis lower than the national rate of 14.5 cases per 100,000 live births included:
- Ontario (9.1 cases per 100,000 live births)
- British Columbia (DNS)
- Québec (DNS)
- New Brunswick (0.0 cases per 100,000 live births)
- Nova Scotia (0.0 cases per 100,000 live births)
- Prince Edward Island (0.0 cases per 100,000 live births)
- Newfoundland and Labrador (0.0 cases per 100,000 live births)
- Nunavut (0.0 cases per 100,000 live births)
| Province or territory | Number of cases | Rate per 100,000 live births, 2023 | Change in rate since 2022 | Change in rate since 2018 |
|---|---|---|---|---|
| British Columbia | DNS | DNS | ↓DNS | NC |
| Alberta | DNS | DNS | ↓DNS | ↑DNS |
| Saskatchewan | DNS | DNS | ↓DNS | NC |
| Manitoba | 12 | 68.0 | ↓−50.4% | ↑66.0% |
| Ontario | 13 | 9.1 | ↓−54.5% | ↑1,188.2% |
| Québec | DNS | DNS | ↑DNS | ↑DNS |
| New Brunswick | 0 | 0.0 | NC | NC |
| Nova Scotia | 0 | 0.0 | NC | NC |
| Prince Edward Island | 0 | 0.0 | NC | NC |
| Newfoundland and Labrador | 0 | 0.0 | NC | ↓−100% |
| Yukon | DNS | DNS | NC | NC |
| Northwest Territories | DNS | DNS | ↓DNS | NC |
| Nunavut | 0 | 0.0 | NC | NC |
| Canada | 53 | 14.5 | ↓−55.6% | ↑220.2% |
Abbreviations: DNS, data not shown to reduce the risk of identifying individuals; NC, non-computable (rate change not computable due to a denominator of 0) |
||||
To learn more about syphilis, visit: www.canada.ca/syphilis.
Appendix A: List of supplementary tables
The supplementary tables described below are available upon request via sti-hep-its@phac-aspc.gc.ca.
- Table 5: Number and proportion of reported cases of infectious syphilis by gender, Canada, 2018–2023Note ४
- Table 6: Rates per 100,000 population of reported cases of infectious syphilis by age group, Canada, 2014–2023Note ४
- Table 7: Rates per 100,000 population of reported cases of infectious syphilis by sex and age group, Canada, 2014–2023Note ४
- Table 8: Number of reported cases of infectious syphilis by sexual behavior, Canada, 2018–2023Note §Note ४
- Table 9: Reported cases and rates per 100,000 population of infectious syphilis by sex and by province and territory, 2023Note ¥
Notes
- Note *
-
Data were directly obtained from provinces and territories through both routine and enhanced surveillance systems for syphilis. Data for 2023 data were received from 12 out of 13 provinces and territories; data for Alberta were projected based on partial-year data. Data for 2023 are preliminary.
- Note **
-
Infectious syphilis includes the primary, secondary, early latent and infectious neurosyphilis (less than one year after infection) stages of infection, during which syphilis is most transmissible. Reference: Public Health Agency of Canada. National case definition: Syphilis. PHAC; 2008. https://www.canada.ca/en/public-health/services/diseases/syphilis/health-professionals/national-case-definition.html. Note that latent syphilis of unknown duration, some of which may be reported by jurisdictions as infectious, is not currently captured in national reporting.
- Note ┼
-
Rates are compared against a 2018 benchmark to align, for comparability purposes, with the Government of Canada’s commitment in 20181 to the World Health Organization (WHO)’s 2030 global STBBI targets2. The targets include a 90% reduction of syphilis incidence and 50 or fewer cases of congenital syphilis per 100,000 live births. 1) Public Health Agency of Canada. Reducing the health impact of sexually transmitted and blood-borne infections in Canada by 2030: A pan-Canadian STBBI framework for action. PHAC; 2018. https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/reports-publications/sexually-transmitted-blood-borne-infections-action-framework.html 2) World Health Organization. Global health sector strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections for the period 2022–2030. WHO; 2022. https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/strategies/global-health-sector-strategies
- Note Ѱ
-
Reporting between 2020 and 2022 occurred in the context of the COVID-19 pandemic, which included a period of decreased demand for and access to sexually transmitted and blood-borne infection (STBBI) services. Reference: Public Health Agency of Canada. National report: findings from the survey on the impact of COVID-19 on the delivery of STBBI prevention, testing and treatment, including harm reduction services, in Canada. PHAC; 2022. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/survey-impact-covid-19-delivery-stbbi-prevention-testing-treatment.html. This decrease in demand for and access to services related to STBBIs, including prevention, testing, treatment and other supportive services, likely contributed to fewer reported cases of infectious and congenital syphilis between 2020 and 2022. As parts of the country experienced various levels of disruptions due to COVID-19 from 2020 to 2022, comparisons of reported infectious and congenital syphilis case counts and rates between provinces and territories may also be inaccurate. The impacts of the COVID-19 pandemic on STBBI services are still ongoing and continue to be experienced to varying extents in different jurisdictions.
- Note ४
-
Due to periodic updates of jurisdictional surveillance data and Statistics Canada population estimates, case counts and rates may change over time. In cases of discrepancy between data reported by PHAC and data reported by individual provinces and territories, provincial and territorial data should be considered more accurate as they are the most current. The Statistics Canada demographic estimates used as denominators to calculate rates of infectious syphilis now incorporate the concept of gender, rather than sex, as was previously the case. This change was introduced in the 2021 Census of Population. Prior to 2021, the demographic estimates were based on the concept of sex at birth. This change may result in variations in the rates computed for past years, although the impact is not expected to be significant, because the two concepts produce very similar distributions. Reference: Statistics Canada. Table 17-10-0005-01 Population estimates on July 1, by age and gender. https://doi.org/10.25318/1710000501-eng. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501
- Note §
-
GBMSM: cisgender gay, bisexual and other men who have sex with men. Note that only eight provinces and territories (British Columbia, Alberta, Saskatchewan, Ontario, New Brunswick, Nova Scotia, Yukon and the Northwest Territories) have consistently submitted data on cases among GBMSM since 2018, therefore only these provinces and territories are included in calculations of GBMSM proportions. Data on other priority populations are not currently available for analysis.
- Note ¥
-
Caution should be used when interpreting changes in rates of congenital syphilis and when comparing rates of infectious or congenital syphilis across provinces and territories. When population denominators are small, even small fluctuations in case counts can result in large rate changes. To contextualize rates and rate changes, it is also important to consider case counts. Considering results in their full context is critical in understanding the syphilis landscape in Canada to address syphilis as a public health threat appropriately, according to the STBBI action plan.
- Note ‡‡
-
Aho J, Lybeck C, Tetteh A, Issa C, Kouyoumdjian F, Wong J, Anderson A, Popovic N. Rising syphilis rates in Canada, 2011–2020. Can Comm Dis Rep 2022;48(2/3):52–60. https://doi.org/10.14745/ccdr.v48i23a01
- Note ╪
-
In the reporting years 2014–2023, the national case definition for congenital syphilis comprised only one case classification, namely confirmed early congenital syphilis. This was defined as a laboratory confirmation of infection by Treponema pallidum occurring within the first two years of birth. Reference: Case definitions for communicable diseases under national surveillance. Can Comm Dis Rep 2009;35S2. Available at https://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/09pdf/35s2-eng.pdf. Provinces and territories submitted data using their own congenital syphilis case definitions. All provinces and territories had a case classification for confirmed early congenital syphilis. British Columbia, Québec and Yukon had case classifications for confirmed early congenital syphilis that included stillbirths. British Columbia also had a case classification for probable early congenital syphilis that included stillbirths. Alberta, Saskatchewan and Manitoba had case classifications for both probable early congenital syphilis and syphilitic stillbirth. The Northwest Territories had a case classification for syphilitic stillbirth, but not for probable early congenital syphilis. The Public Health Agency of Canada, in collaboration with provinces and territories, revised the national case definition for congenital syphilis in January 2024.
© His Majesty the King in Right of Canada, as represented by the Minister of Health, 2025.
