
At-a-glance – Injuries and poisonings associated with methamphetamine use: sentinel surveillance, the electronic Canadian Hospitals Injury Reporting and Prevention Program (eCHIRPP), 2011–2019
Health Promotion and Chronic Disease Prevention in Canada
Steven R. McFaull, MSc; André Champagne, MPH; Wendy Thompson, MSc; Felix Bang, MPH
https://doi.org/10.24095/hpcdp.40.4.04
Author references
Public Health Agency of Canada, Ottawa, Ontario, Canada
Correspondence: Steven R. McFaull, Injury Section, Centre for Surveillance and Applied Research, Public Health Agency of Canada, 785 Carling Avenue, Ottawa, ON K1A 0K9; Tel: 613-404-1881; Email: steven.mcfaull@canada.ca
Abstract
Information from emergency department (ED) visits for methamphetamine-related injuries and poisonings between 1 April 2011 and 9 August 2019 were captured from 19 sentinel sites across Canada for all ages.
Overall, 1093 cases (97.6/100 000 eCHIRPP cases) were identified (59.4% male), with female patients experiencing more poisonings (71% vs 57.4% for males). Unintentional injuries and poisoning accounted for 14.8% of ED presentations. Self-harm (while or as a result of consuming methamphetamine) accounted for 11.4% of cases. The circumstances surrounding injuries and poisonings associated with methamphetamine are varied and include self-harm, fall-related brain injuries, mental illness, criminal activity and other circumstances. These domains should be taken into account when developing mitigation strategies.
Keywords: methamphetamine, poisoning, injury, surveillance, eCHIRPP
Highlights
- 1093 methamphetamine-related injury and poisoning cases presented to participating emergency departments (EDs).
- 71.4% of patients aged 10–14 years were female; of those aged 15–19 years, 63.7% were female.
- 70.4% of the patients aged 20 years plus were male.
- Of the 689 cases that also involved other substances (63%), 40.9% involved two or more other substances. Alcohol (24.4%), cannabis (10.7%), cocaine (7.7%), heroin (5.4%), opiates (3.6%) and other substances (7.3%) were involved when only one substance other than methamphetamine was used.
- Compared to males, females had more poisonings, while males more frequently had multiple injuries.
- Self-harm accounted for 11.4% of cases.
Introduction
Methamphetamine is a highly addictive stimulant that acts on the central nervous system. Also known as “meth,” “blue,” “ice,” “crystal,” “crank,” “peanut” and others, methamphetamine takes the form of an odourless, bitter-tasting white crystalline powder that dissolves in water or alcohol. Methamphetamine was developed in the 1930s from its parent drug, amphetamine. It was used originally in nasal decongestants and bronchial inhalers.Footnote 1Footnote 2Footnote 3
Like amphetamine, methamphetamine use decreases appetite and increases alertness and energy, euphoria, physical activity, talkativeness, disinhibition and confidence. Chronic use may lead to psychotic symptoms such as hallucinations, paranoia and anxiety.Footnote 4
Methamphetamine differs from amphetamine in that, at similar doses, larger amounts of the drug get into the brain, making it a more potent psychostimulant.Footnote 5 It also has longer-lasting and more harmful effects on the central nervous system.Footnote 6 Methamphetamine can be easily manufactured from readily available precursor substances.Footnote 4 These characteristics make it a drug with high potential for abuse.
There are many physical, physiological and psychological harms associated with methamphetamine use and manufacture.Footnote 4Footnote 7Footnote 8Footnote 9Footnote 10Footnote 11 There are also sex differences in the harms associated with methamphetamine use.Footnote 1
The purpose of this study is to describe the circumstances of emergency department (ED) visits for injuries and poisonings associated with methamphetamine use or manufacture.
Methods
Data source
The Electronic Canadian Hospitals Injury Reporting and Prevention Program (eCHIRPP) is an injury and poisoning sentinel surveillance system operating in 11 pediatric and 8 general hospitals across Canada. eCHIRPP is managed by the Centre for Surveillance and Applied Research at the Public Health Agency of Canada. The eCHIRPP captures detailed information via text fields, which allows more detailed coding of circumstances and mechanisms.Footnote 13 In contrast, administrative data coding using International Classification of Diseases, 10th Revision (ICD-10-CA)Footnote 14 lacks the specificity to identify methamphetamine-related cases and does not provide details surrounding the circumstances of the incident.
Extraction of cases
We searched the eCHIRPP database for cases (all ages) of methamphetamine-related injuries and poisonings in the system as of 9 August 2019. Cases were included if the injured/poisoned person was a consumer and/or a manufacturer of methamphetamine or if the patient was injured by a person under the influence of and/or manufacturing methamphetamine (including infants born to addicted mothers and child bystanders). Since people could be injured (as opposed to poisoned), we used a broad, bilingual (English and French) text search to identify records using the eCHIRPP narrative and substance ID fields. A detailed list of 83 terms in both official languages (available upon request) was used in the initial search. Ultimately, the majority of cases (82.1%) were identified with four keywords/strings: “meth,” “crystal meth,” “speed” and “ice.” The data were cleaned by mining the narrative fields using Practical Extraction and Report Language (PERL) regular expressionsFootnote 15 in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and all irrelevant expressions (e.g. “speed bumps,” “speeding”) were excluded.
The clean dataset was manually reviewed and coded with further circumstantial details (police involvement, use of other substances, self-harm, “on a bender,” presented with an unintentional injury, etc.).
Statistical analyses were conducted using SAS version 9.4, Epi Info 7.2.0.1 (CDC, Atlanta, GA, USA) and Microsoft Excel (2013).
Results
Overview
Overall, 1093 patients (97.6/100,000 eCHIRPP cases) were identified for the period between 1 April 2011 and 9 August 2019; of these, 59.4% (n = 649) were male. Among those aged 10–14 and 15–19 years, females accounted for 71.4% and 63.7%, respectively. Of those aged 20 years and older, males predominated at 70.4% (see Figure 1 for the normalized age and sex distribution).
Figure 1. NormalizedFootnote a age and sex distribution of emergency department visits associated with methamphetamine use, eCHIRPP, 2011–2019 (N = 1093)
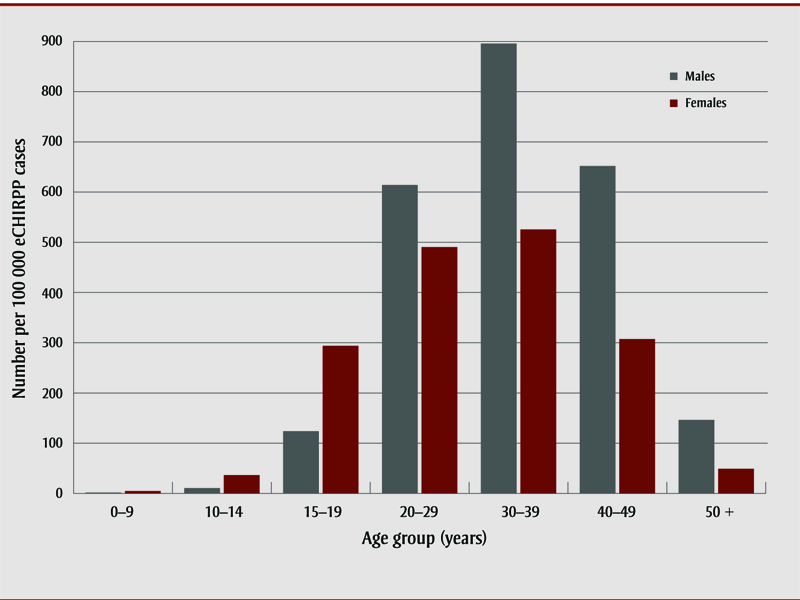
Figure 1 - Text Equivalent
| Age group (years) | Males | Females |
|---|---|---|
| 0–9 | 1.7 | 4.8 |
| 10–14 | 10.5 | 36.4 |
| 15–19 | 123.8 | 293.8 |
| 20–29 | 614.1 | 490.4 |
| 30–39 | 895.7 | 525.5 |
| 40–49 | 651.9 | 307.4 |
| 50 + | 146.4 | 49.0 |
Abbreviation: eCHIRPP, electronic Canadian Hospitals Injury Reporting and Prevention Program.
- Footnote a
-
Expressed as a proportion of all eCHIRPP cases in the given age group (× 100 000).
Location
The location where the injury occurred was specified in 420 cases (38.4%). Of those, 30.2% occurred in the patient’s own home and 16.9% in another private home. About one-quarter (26.4%) of the incidents happened outside, on a road or in an alley or public park. The injury occurred in a group home in 7.1% of cases. The remaining incidents (approximately 20%) occurred in hospitals, bars, hotels and numerous other locations, with each type of location contributing only a few per cent overall.
Circumstances
At 14.8%, unintentional injuries (aside from the toxic effects of the substances) were the most frequent circumstances surrounding the ED presentation (see Table 1). Of these unintentional injuries, 30.2% were falls. Self-harm, including attempted suicide, accounted for 11.4% of cases. People aged 15–29 years accounted for the highest percentage of self-harm (data not shown). Of the self-harm cases aged 10–19 years, 75% were female; among those aged 20–49 years, 66.7% were male. Of the 1093 identified patients, 10.8% involved police or criminal activity and 9.4% involved violence (family and other).
| CircumstancesFootnote a leading to ED visit | Number | |
|---|---|---|
| Frequency (n) | Per cent (%) | |
| Unintentional injury | 162 | 14.8 |
| Fall | 49 | 4.5 |
| Motor vehicle collision | 32 | 2.9 |
| Bicyclist, pedestrian | 22 | 2.0 |
| Other unintentional injuryFootnote b | 59 | 5.4 |
| Self-harm, suicide | 125 | 11.4 |
| Police involvement/criminal activityFootnote c | 118 | 10.8 |
| KnownFootnote d addict/abuser | 108 | 9.9 |
| On a binge/benderFootnote e | 106 | 9.7 |
| Violence | 103 | 9.4 |
| Other violenceFootnote f | 77 | 7.0 |
| Family violence | 26 | 2.4 |
| Found having a seizure/unresponsive | 82 | 7.5 |
| Found wandering, homeless | 62 | 5.7 |
| Depression, anxiety, mentally ill | 59 | 5.4 |
| Partying (including at a rave) | 37 | 3.4 |
| Asking for help | 9 | 0.8 |
| Other person injected or “slipped” pillFootnote g | 8 | 0.7 |
| Undergoing meth withdrawalFootnote h | 7 | 0.6 |
| Bad batch/“different from usual” | 6 | 0.5 |
| Took meth, NFS | 93 | 8.5 |
| OtherFootnote i | 8 | 0.7 |
| Total | 1093 | 100.0 |
Abbreviations: eCHIRPP, electronic Canadian Hospitals Injury Reporting and Prevention Program; ED, emergency department; NFS, not further specified.
|
||
Use of other substances
Of the 1093 identified patients, 404 (37%) involved methamphetamine use alone. Of the remaining 689 cases, 40.9% involved polysubstance use (i.e. the simultaneous use of two or more substances in addition to methamphetamine). When only one other substance was involved, the following distribution was observed: alcohol (24.4%), cannabis (10.7%), cocaine (7.7%), heroin (5.4%), opiates (3.6%) and other substances (e.g. LSD, ecstasy, psychoactive medications) (7.3%).
Injuries and poisonings – sex differences
The 1093 patients had a total of 1389 injuries and poisonings, as 27.1% had multiple injuries. The sex differences in the injury and poisoning patterns were as follows: male patients had multiple injuries more frequently (32.8% vs. 18.7% for females; p < .001); female patients had more poisonings (71% vs. 57.4% for males; p < .001). Also, male patients had a higher proportion of fractures (21.5% vs 11.1%; p < .005) and females had a higher proportion of bruises and abrasions (16.3% vs. 7.9%; p < .005). After evaluation in EDs, females more frequently had a diagnosis of “no injury detected” (11.8% vs. 4.4% for males; p < .005). Males had a higher proportion of traumatic brain injuries (9.8% vs. 5.2% for females), but due to the low counts, this was statistically not significant (p = .06). Thirteen patients had frostbite due to prolonged exposure to cold (“found outside unresponsive”). Males accounted for 11 of these 13 cases, but due to low counts the difference was not statistically significant (p = .21).
Treatment in the emergency department
Overall, 17.7% of male cases and 10.8% of female cases (p < .001) who presented to the ED were admitted. A further 2.9% of cases were admitted for reasons other than injury (e.g. addiction treatment).
Discussion
The physical and psychological harms to users as well as to families and society can be considerable, making methamphetamine use a serious public health concern.Footnote 7Footnote 16
The opioid crisis in Canada has shown that various factors contribute to substance abuse increasing rapidly in populations.Footnote 17 Thus continued surveillance is necessary to detect changes and implement mitigation strategies.
The eCHIRPP narratives allow contextual information and further circumstantial details can be gleaned, for example, involvement of police/criminal activity, family violence, psychological state, self-harm, homelessness and other situations. This information can be used in health promotion and injury mitigation efforts. The eCHIRPP database has been previously used in the same way to describe suspected opioid-related poisonings.Footnote 18
We observed sex differences with respect to poisonings, injuries and self-harm. Such sex differences (which have been previously reportedFootnote 12) should be kept in mind when developing prevention initiatives.
Strengths and limitations
The eCHIRPP does not capture all the incidents in Canada, but only those presenting to the participating EDs. Because most of the eCHIRPP hospitals are pediatric (and usually located in major cities), certain populations are underrepresented, for example, rural inhabitants (including some Indigenous peoples), older teens and adults.
While eCHIRPP captures people who are dead-on-arrival, those who died at the scene or later in hospital are not included. Patients who bypass the ED registration desk for immediate treatment may also not be captured as is the case for those who do not complete an Injury/Poisoning Reporting form.
In the case of polysubstance use, it is not possible to determine the effects of the individual substances on the outcome. In addition, sex differences in use behaviors and drug responses may result in a bias of those presenting to the ED.Footnote 12Footnote 19
Conclusion
The circumstances, sex and age differences to do with injuries and poisonings associated with methamphetamine use and manufacture should be taken into account when developing mitigation strategies.
Acknowledgements
The authors would like to thank James Cheesman for extracting the data and Jaskiran Kaur and Aimée Campeau for reviewing the manuscript.
Conflicts of interest
The authors declare no conflicts of interest.
Authors’ contributions and statement
SRM: conceptualization, analysis, methodology, writing – original draft; AC: writing – review and editing; WT: writing – review and editing; FB: writing – review and editing.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.
References
- Footnote 1
-
Diversion Control Division. National Forensic Laboratory Information System (NFLIS): 2015 Annual Report. Springfield (VA): U.S. Department of Justice Drug Enforcement Agency; 2016.
- Footnote 2
-
Chomchai C, Chomchai S. Global patterns of methamphetamine use. Curr Opin Psychiatry. 2015;28(4):269-74. doi:10.1097/YCO.0000000000000168.
- Footnote 3
-
Levmetamfetamine [Internet]. Drugbank; 2015 Nov 30 [cited 2019 Oct 3]. Available from: https://www.drugbank.ca/drugs/DB09571
- Footnote 4
-
Sheridan J, Bennett S, Coggan C, Wheeler A, McMillan K. Injury associated with methamphetamine use: a review of the literature. Harm Reduct J. 2006;3:14. doi:10.1186/1477-7517-3-14.
- Footnote 5
-
Panenka WJ, Procyshyn RM, Lecomte T, et al. Methamphetamine use: a comprehensive review of molecular, preclinical and clinical findings. Drug Alcohol Depend. 2013;129(3):167-79. doi:10.1016/j.drugalcdep.2012.11.016.
- Footnote 6
-
Moszczynska A. Neurobiology and clinical manifestations of methamphetamine neurotoxicity. Psychiatr Times. 2016;33(9):16-8.
- Footnote 7
-
Darke S, Kaye S, McKetin R, Duflou J. Major physical and psychological harms of methamphetamine use. Drug Alcohol Rev. 2008;27:253-62. doi:10.1080/09595230801923702.
- Footnote 8
-
Charukamnoetkanok P, Wagoner MD. Facial and ocular injuries associated with methamphetamine production accidents. Am J Opthalmol. 2004;138(5):875-6. doi:10.1016/j.ajo.2004.05.056.
- Footnote 9
-
Lee JH, Farley CL, Brodrick CD, Blomquist PH. Anhydrous ammonia eye injuries associated with illicit methamphetamine production. Ann Emerg Med. 2003;41(1):157. doi:10.1067/mem.2003.33.
- Footnote 10
-
Davidson SB, Blostein PA, Walsh J, Maltz SB, Elian AE, Vandenberg SL. Resurgence of methamphetamine related burns and injuries: a follow-up study. Burns. 2013;39:119-25. doi:10.1016/j.burns.2012.03.003.
- Footnote 11
-
Swanson SM, Sise CB, Sise MJ, Sack DI, Holbrook TL, Paci GM. The scourge of methamphetamine: impact on a level I trauma center. J Trauma. 2007;63(3):531-7. doi:10.1097/TA.0b013e318074d3ac.
- Footnote 12
-
Brecht ML, O’Brien A, von Mayrhauser C, Anglin MD. Methamphetamine use behaviors and gender differences. Addict Behav. 2004;29:89-106. doi:10.1016/S0306-4603(03)00082-0.
- Footnote 13
-
Crain J, McFaull S, Thompson W, et al. Status report. The Canadian Hospitals Injury Reporting and Prevention Program: a dynamic and innovative injury surveillance system. Health Promot Chronic Dis Prev Can. 2016;36(6):112-7. doi:10.24095/hpcdp.36.6.02.
- Footnote 14
-
Canadian Institute for Health Information. International statistical classification of diseases and related health problems, 10th revision, Canada. Volume Two — Alphabetical Index [Internet]. Ottawa (ON): CIHI; 2015 [cited 2017 Dec 11]. Available from: https://www.cihi.ca/sites/default/files/icd_volume_two_2015_en_0.pdf
- Footnote 15
-
Zhang Y. PERL regular expression in SAS macro programming. SAS Global Forum. 2011;159–2011:1-7.
- Footnote 16
-
McKetin R, Degenhardt L, Shanahan M, Baker AL, Lee NK, Lubman DI. Health service utilisation attributable to methamphetamine use in Australia: patterns, predictors and national impact. Drug Alcohol Rev. 2018;37:196-204. doi:10.1111/dar.12518.
- Footnote 17
-
Belzak L, Halverson J. The opioid crisis in Canada: a national perspective. Health Promot Chronic Dis Prev Can. 2018; 38(6):224-33. doi:10.24095/hpcdp.38.6.02.
- Footnote 18
-
Do MT, Chang VC, Tibebu S, Thompson W, Ugnat AM. Sentinel surveillance of suspected opioid-related poisonings and injuries: trends and context derived from the electronic Canadian Hospitals Injury Reporting and Prevention Program, March 2011 to June 2017. Health Promot Chronic Dis Prev Can. 2018;38(9):317-27. doi:10.24095/hpcdp.38.9.03.
- Footnote 19
-
Mayo LM, Paul E, DeArcangelis J, Van Hedger K, de Wit H. Gender differences in the behavioral and subjective effects of methamphetamine in healthy humans. Psychopharmacology. 2019;236:2413-23.