
Evidence synthesis – Structural determinants of stigma across health and social conditions: a rapid review and conceptual framework to guide future research and intervention
Health Promotion and Chronic Disease Prevention in Canada
Clara Bolster-Foucault, MScPHAuthor reference footnote 1Author reference footnote 2; Brigitte Ho Mi Fane, MPHAuthor reference footnote 1; Alexandra Blair, PhDAuthor reference footnote 1Author reference footnote 3
https://doi.org/10.24095/hpcdp.41.3.03
This article has been peer reviewed.
Correspondence: Alexandra Blair, Dalla Lana School of Public Health, University of Toronto, 155 College Street, Toronto, ON M5T 1P8; Email: alexandra.blair@utoronto.ca
Abstract
Introduction: Stigma has been identified as a key determinant of health and health inequities because of its effects on access to health-enabling resources and stress exposure. Though existing reports offer in-depth summaries of the mechanisms through which stigma influences health, a review of evidence on the upstream drivers of stigma across health and social conditions has been missing. The objective of this review is to summarize known structural determinants of stigma experienced across health and social conditions in developed country settings.
Methods: We conducted a rapid review of the literature. English- and French-language peer-reviewed and grey literature works published after 2008 were identified using MEDLINE, Embase, PsycINFO, Google and Google Scholar. Titles and abstracts were independently screened by two reviewers. Information from relevant publications was extracted, and a thematic analysis of identified determinants was conducted to identify broad domains of structural determinants. A narrative synthesis of study characteristics and identified determinants was conducted.
Results: Of 657 publications identified, 53 were included. Ten domains of structural determinants of stigma were identified: legal frameworks, welfare policies, economic policies, social and built environments, media and marketing, pedagogical factors, health care policies and practices, biomedical technology, diagnostic frameworks and public health interventions. Each domain is defined and summarized, and a conceptual framework for how the identified domains relate to the stigma process is proposed.
Conclusion: At least 10 domains of structural factors influence the occurrence of stigma across health and social conditions. These domains can be used to structure policy discussions centred on ways to reduce stigma at the population level.
Keywords: stigma, discrimination, structural determinants, social conditions, health conditions
Highlights
- A review of known structural determinants of stigma operating across health and social conditions has been missing from existing literature.
- This study reviewed and synthesized existing literature and identified 10 domains of structural determinants of stigma.
- The 10 domains identified were: legal frameworks, welfare policies, economic policies, social and built environments, media and marketing, pedagogical factors, health care policies and practices, biomedical technology, diagnostic frameworks and public health interventions.
- The proposed conceptual framework of the 10 domains of structural determinants of stigma can be used to structure future policy discussions on ways to address stigma at the population level.
Introduction
Stigma has been defined as a process enabled by social, economic and political power inequities, through which negative labels, beliefs and perceived differences between groups can culminate in discrimination and status loss.Footnote 1 As Link and Phelan wrote, “…stigma exists when elements of labelling, stereotyping, separation, status loss and discrimination occur together in a power situation that allows them.”Footnote 1,p.377 A key social determinant of health, stigma is a cause for concern in many substantive areas of public health practice.Footnote 2 Stigma-related discrimination and status loss influence health by restricting affected populations’ access to health-enabling resources such as housing, employment, social ties and health care, and by increasing exposure to stress.Footnote 2
In Canada, the Public Health Agency of Canada’s Chief Public Health Officer (CPHO)’s 2019 report Addressing Stigma: Towards a More Inclusive Health SystemFootnote 3 has proposed a conceptual summary of the myriad pathways through which stigma can affect health and health inequities. This and previous frameworksFootnote 4Footnote 5 are helpful for understanding the theoretical underpinnings of the effects of stigma on health and for identifying potential areas for health and social policy intervention.
However, with their in-depth focus on the downstream effects of stigma on health, existing reports typically lack a thorough exploration of the upstream factors that drive stigma,Footnote 6 particularly those operating at a structural level. Existing literature on structural determinants of stigma tends to focus on stigma pertaining to specific stigmatized experiences, identities, behaviours or health conditions.Footnote 7Footnote 8 A general summary of determinants of stigma across affected populations is currently missing from the literature. This review seeks to fill these gaps in the extant literature by contributing a summary of known structural determinants of stigma across stigmatized populations.
Described as “contextual factors” in the World Health Organization’s Social Determinants of Health Model,Footnote 9 and structural “practices” in the CPHO’s 2019 report’s Stigma Pathways Model,Footnote 3 structural determinants can be defined as factors that operate outside the locus of control of individuals,Footnote 10 such as elements of physical, social, policy or legal environments.Footnote 11 For example, structural determinants can include various forms of legislation (or lack thereof) to protect individuals’ rights,Footnote 12 or wealth redistribution policies.Footnote 9Footnote 13 Structural factors are distinct from but tightly influence more proximal, individual-level determinants of health, such as individuals’ access to income, housing, food or safe working conditions.Footnote 9
The scope of this review is restricted to examining the structural determinants of stigma for several reasons. First, according to public health research and theory, structural factors are considered to be those that create and perpetuate social and economic stratification within societies.Footnote 9 They are often identified as “root causes” of negative health and social outcomes and health inequities, and therefore merit particular attention from the perspective of population health and health equity promotion.Footnote 9
Second, in the context of public health practice, structural factors tend to exert influence across multiple social contexts and populations.Footnote 14 Structural factors are therefore particularly relevant to consider when aiming to understand the determinants of stigma occurring across a multitude of health and social conditions—particularly when many forms of stigma intersect.Footnote 3
Third, though it is difficult to achieve and often requires intersectoral collaboration,Footnote 9 structural determinants can theoretically be modified through changes in health and social policy.Footnote 15 When successful, structural-level interventions are often more impactful and far-reaching than more proximal (i.e. individual-level) interventions at reducing population-level health inequities.Footnote 9
This review therefore was intended to provide a knowledge summary that, in the Canadian context, can complement the knowledge synthesis of the Canadian CPHO’s report on stigma’s effects on healthFootnote 3 and, more broadly, can be used to structure policy discussions on ways to orient public health interventions to reduce stigma in Canada and abroad. The specific objective of this rapid review was to identify and summarize known structural determinants of stigma in Canada and in similar settings, such as those in other member countries of the Organisation for Economic Co-operation and Development (OECD).
Methods
We used a rapid review design.Footnote 16 Used most frequently within governmental policy contexts when time-related resources are limited,Footnote 17 a rapid review consists of an evidence review strategy that follows the structure of a systematic review process with abridged components to allow research questions to be addressed in a shorter time frame than is typically needed for a systematic review.Footnote 16 A defining feature of the rapid review design is its restricted evidence search component,Footnote 17 which involves a non-exhaustive search of available evidence pertaining to the research question. First, a search strategy to identify presynthesized evidence summaries (reviews, summary reports, conceptual frameworks) is applied. If identified synthesis documents are insufficient, because identified publications are not sufficiently recent or methodologically rigorous, a search for less synthesized evidence, including individual studies, is then conducted based on study relevance. Individual studies are collected until additional works fail to offer new information needed to address the research question or until other time or resource constraints prohibit future searches.Footnote 16
For this review, a first search strategy was designed to prioritize the identification of presynthesized evidence such as conceptual summaries and literature reviews (Table 1, rows A and B).Footnote 18 A secondary search strategy was then applied to identify relevant individual studies, using general title and abstract search terms pertaining to the theme of “structural determinants of stigma” (Table 1, row C).Footnote 18 This secondary search was non-exhaustive. It was done to fill potential data gaps and identify domains missing from identified syntheses, and was ceased after the search strategy no longer yielded studies that reported new types of structural determinants or forms of stigma.
| Components of search | Search string in titles or abstracts |
French terms |
|---|---|---|
| A. Conceptual frameworks of determinants of stigma and mechanisms explaining stigma’s effect on health | (stigma OR stigmatization OR stigmatisation OR “stigmatized status”) AND (determinants OR cause OR “social factors” OR theory OR process OR pathway OR mechanism) AND (“conceptual framework” OR framework) |
Stigmatisation, stigmatisé déterminant, cause, « facteur social » théorie, processus, mécanisme, « cadre conceptuel » |
| B. Systematic reviews of determinants of stigma | (Stigma OR stigmatization OR stigmatisation OR discrimination OR “stigmatized status”) AND (determinants OR cause OR “social factors” OR theory OR process OR pathway OR mechanism) AND (“systematic review” OR review) |
« Revue systématique », revue, « recension des écrits » stigmatisation, stigmatisé déterminant, cause, « facteur social » |
| C. Individual studies of structural, upstream, system-level, population-level social determinants of stigma | (Stigma OR stigmatization OR stigmatisation OR “stigmatized status”) AND (determinants OR cause OR factor) AND (structural OR upstream OR “population-level” OR “system-level” OR structure OR structural OR infrastructural OR legal OR legislation OR policy OR “social environment” OR “built environment”) |
Structurel, structure, amont, populationnel, système, systémique, infrastructure, légal, législation, « environnement social », « environnement bâti » |
Note: The first search strategy was designed to prioritize the identification of presynthesized evidence such as conceptual summaries and literature reviews (rows A and B). A secondary search strategy was then applied to identify relevant individual studies, using general title and abstract search terms pertaining to the theme of “structural determinants of stigma” (row C). This secondary search was non-exhaustive. It was done to fill potential data gaps and identify domains missing from identified syntheses, and was ceased after the search strategy no longer yielded studies that reported new types of structural determinants or forms of stigma. |
||
Eligibility criteria
Works included were those documenting conceptual frameworks, reviews and individual quantitative, qualitative or mixed-methods studies of structural determinants of stigma. We restricted our review to works in English or French (due to the authors’ languages of expertise), published since January 2008, in peer-reviewed or grey-literature sources and set in Canada or other OECD nations. We excluded works without a research design (e.g. commentaries, letters to editors, fact sheets), as well as those that were not available through the Health Canada Health Library network.
Search strategy
MEDLINE, Embase, PsycINFO, Google and Google Scholar databases were searched to ensure appropriate coverage of international health research and social science literature.Footnote 19 Table 1 presents a summary of the search string components. Search strings were also applied in French in Google and Google Scholar, of which the first three pages of results were reviewed. A snowball search approachFootnote 20 was also used to identify reviews or conceptual summaries that were mentioned in reviewed studies but were not captured through our search strategy.
Study identification, data extraction and quality appraisal
Two reviewers independently screened titles and abstracts of all identified works, and, based on eligibility criteria, selected works for full-text review through consensus. Four reviewers conducted full-text screening and extracted data on publications’ authors, year of publication, title, country setting, study population and identified structural-level determinants of stigma (Table 2). All data elements were recorded in the data extraction table to enable synthesis of study features and thematic analysis of structural determinants. Two reviewers evaluated the quality of included works using an adaptation of Dixon-Woods et al.’s framework for critical appraisal of works with varied design.Footnote 21 Seven questions requiring yes-or-no answers were applied to evaluate the quality of each publication (Table 3).
| Author, year | Setting | Design | Population | Identified structural determinants of stigma | Structural determinant domains | Critical appraisal score |
|---|---|---|---|---|---|---|
| Clair et al. 2016Footnote 46 | United States | Mixed methods sequential design | People living with HIV, African Americans, and people labelled as obese | Framework proposed: cultural resources and actors contributing to de-stigmatization
|
Legal frameworks Pedagogy |
Moderate |
| Coreil et al. 2010Footnote 48 | United States and Haiti | Mixed methods sequential design | Haitian immigrants (N = 95), TB patients (N = 126), health care providers (N = 126) |
|
Legal frameworks Social & built environment Media & marketing Health care practices Biomedical technology |
Strong |
| Henderson et al. 2017Footnote 68 | United States (Alabama) | Mixed methods sequential design | College students aged 18–25 years, N = 38 to 212 based on study phase |
|
Legal frameworks Pedagogy |
Strong |
| MacLean 2018Footnote 47 | Canada | Mixed methods sequential design | Individuals with STBBI experience (N = 20 individual interviews, N = 3 focus groups), provider survey (N = 410) | Framework proposed: conceptual framework of STBBI stigma (structural stigma: stigma confronted at policy/legal, institutional, community levels) | Legal frameworks | Weak |
| Arrey et al. 2017Footnote 55 | Belgium | Qualitative | Adult HIV+ women who migrated from sub-Saharan Africa to Belgium (N = 44) |
|
Welfare policy Media & marketing Pedagogy Health care policy |
Strong |
| France et al. 2015Footnote 41 | Ireland | Qualitative | Persons living with HIV (N = 17) | Framework proposed: conceptual framework of HIV self-stigma (social factors, self-factors, contextual factors)
|
Social & built environment Health care practices |
Strong |
| Hansen et al. 2014Footnote 73 | United States (New York City) | Qualitative | Individuals who received psychiatric diagnoses and qualified for disability benefits (N = 4) |
|
Welfare policy | Strong |
| Paterson et al. 2013Footnote 65 | Canada (Nova Scotia) | Qualitative | Professionals in ERs (N = 25) or NGOs (N = 25) serving those who use illicit substances or living with hepatitis C | Framework proposed: analytic framework of structural stigmatization (institutional policies, cultural, protocols)
|
Health care practices | Strong |
| Woodgate et al. 2017Footnote 40 | Canada (Winnipeg) | Qualitative | Indigenous people living with HIV since age 15–29 years (N = 21); service providers, elders (N = 14) | Framework proposed: social ecology of stigma and discrimination for Indigenous people living with HIV in Manitoba, Canada
|
Welfare policy Pedagogy Health care practices |
Strong |
| Jorm et al. 2008Footnote 79 | Australia | Quantitative (cross-sectional) | Adult (> 18 years), general population surveyed on mental health–related stigma (N = 3998) |
|
Biomedical technology Diagnostic frameworks |
Moderate |
| Min et al. 2017Footnote 39 | South Korea | Quantitative (cross-sectional) | Persons living with mental illness who were users of community mental health centres (N = 532) |
|
Social & built environment | Strong |
| Pachankis et al. 2017Footnote 69 | Europe | Quantitative (cross-sectional) | Immigrants to Europe who identify as MSM surveyed on HIV risk (N = 23 371) |
|
Legal frameworks | Strong |
| Stringer et al. 2016Footnote 78 | United States (Southern states) | Quantitative (cross-sectional) | Health care workers surveyed on HIV-related stigma (N = 651) |
|
Health care policy Biomedical technology |
Strong |
| Stuber et al. 2008Footnote 64 | United States (New York City) | Quantitative (cross-sectional) | Current and former smokers in New York City (N = 816) |
|
Welfare policy Economic policy Social & built environment |
Strong |
| Angermeyer et al. 2014Footnote 75 | Germany | Quantitative (longitudinal) | Adults (> 18 years) (Cycle 1, N = 5025; Cycle 2, N = 1232) surveyed on mental health stigma |
|
Economic policy Social & built environment |
Strong |
| Hatzenbuehler et al. 2015Footnote 70 | United States | Quantitative (longitudinal) | Youth (9–14 years) from the Growing Up Today Study cohort surveyed on illicit substance use (N = 12 723) |
|
Legal frameworks Social & built environment |
Moderate |
| Arboleda-Florez et al. 2012Footnote 29 | No restriction | Review (narrative) | Persons living with mental health issues | Structural approaches are identified to curb attributions of blame, dangerousness, unpredictability and thereby reduce stigma:
|
Legal frameworks Pedagogy |
Moderate |
| Aste 2016Footnote 53 | United States | Review (narrative) | Adults with chronic pain |
|
Pedagogy | Strong |
| Bell et al. 2016Footnote 63 | No restriction | Review (narrative) | Mothers of children born with fetal alcohol syndrome disorder (FASD) | Framework proposed: stigma “loads” experienced by those affected by FASD
|
Diagnostic frameworks Public health interventions |
Moderate |
| Benoit et al. 2018Footnote 60 | No restriction | Review (narrative) | Sex workers |
|
Legal frameworks Economic policy Media & marketing Health care practices Public health interventions |
Moderate |
| Bonsack et al. 2013Footnote 31 | No restriction | Review (narrative) | Individuals living with mental illness |
|
Legal frameworks Pedagogy Health care practices |
Weak |
| Brewis 2014Footnote 62 | No restriction | Review (narrative) | Individuals labelled as obese |
|
Economic policies Social & built environment |
Moderate |
| Carroll 2017Footnote 61 | United Kingdom | Review (narrative) | Single mothers |
|
Legal frameworks Welfare policy Social environment Media & marketing |
Strong |
| Chaudoir et al. 2013Footnote 66 | No restriction | Review (narrative) | Individuals with visible or concealable stigmatized attributes | Framework proposed: the stigma mechanisms in health disparitiesframework
|
Legal frameworks Welfare policy Social & built environment |
Moderate |
| Collins et al. 2013Footnote 32 | United States | Review (narrative) | Individuals living with mental illness | Framework proposed: conceptual model for reducing stigma associated with mental illness (individual, social, and policy/practice change)
|
Media & marketing Pedagogy |
Weak |
| Livingston, JD (Commission de la santé mentale du Canada), 2013Footnote 37 | Canada | Review (narrative) | Individuals living with mental health issues |
|
Welfare policy Economic policy Social & built environment Media & marketing Pedagogy Health care practices |
Moderate |
| National Academies of Sciences, Engineering, Medicine (Committee on the Science of Changing Behavioral Health Social Norms) 2016Footnote 34 | No restriction | Review (narrative) | Individuals with mental and substance use disorders |
|
Legal frameworks Social & built environment Media & marketing Pedagogy Health care practices |
Moderate |
| De Ruddere & Craig 2016Footnote 52 | No restriction | Review (narrative) | Individuals living with chronic nonmalignant pain |
|
Pedagogy | Moderate |
| Désy et al. 2013Footnote 76 | Canada | Review (narrative) | Stigma in the context of public health actions |
|
Social & built environment Media |
Weak |
| Earnshaw et al. 2015Footnote 42 | United States | Review (narrative) | Individuals living with HIV | Framework proposed: Stigma and HIV Disparities Model
|
Social & built environment Public health interventions |
Moderate |
| Fernandes et al. 2011Footnote 51 | No restriction | Review (narrative) | Individuals living with epilepsy |
|
Legal frameworks Pedagogy |
Moderate |
| Golub 2018Footnote 26 | No restriction | Review (narrative) | Individuals who may be eligible for HIV pre-exposure prophylaxis (PrEP) |
|
Health care practices Biomedical technology |
Moderate |
| Groulx 2011Footnote 59 | Canada | Review (narrative) | Individuals experiencing economic and social exclusion |
|
Welfare policy Economic policy |
Strong |
| Hatzenbuehler 2016Footnote 8 | No restriction | Review (narrative) | Persons living with mental health issues and sexual minorities |
|
Legal frameworks | Moderate |
| Hatzenbuehler 2014Footnote 57 | No restriction | Review (narrative) | Lesbian, gay, bisexual (LGB) populations |
|
Legal frameworks Social & built environment |
Moderate |
| Holder et al. 2019Footnote 30 | United States | Review (narrative) | Individuals living with mental health issues |
|
Pedagogy | Moderate |
| Kerr et al. 2016Footnote 45 | United States | Review (narrative) | Disparities in HIV risk across racialized communities in the context of drug policy | Framework proposed: the Drug War HIV/AIDS Inequities Model
|
Legal frameworks Welfare policies |
Moderate |
| Knapp et al. 2014Footnote 54 | No restriction | Review (narrative) | Individuals living with cancer |
|
Legal frameworks Media & marketing Biomedical technology |
Strong |
| Link & Hatzenbuehler 2016Footnote 72 | United States | Review (narrative) | General population |
|
Legal frameworks Social & built environment Pedagogy |
Moderate |
| Ministère de la Santé et des Services sociaux du Québec, 2016Footnote 38 | Canada | Review (narrative) | Individuals with a history of mental illness accessing health care services |
|
Pedagogy | Weak |
| Mirabito et al. 2016Footnote 67 | No restriction | Review (narrative) | Stigma occurring in the marketplace | Framework proposed: The Stigma Turbine of individual, societal and marketplace-based determinants of stigma.
|
Legal frameworks Social & built environment Media & marketing Public health interventions |
Moderate |
| Morey 2018Footnote 56 | United States | Review (narrative) | Immigrants and racialized communities in the United States |
|
Legal frameworks Welfare policy Media & marketing |
Moderate |
| Mukolo et al. 2010Footnote 28 | No restriction | Review (narrative) | Children experiencing mental illness | Framework proposed: framework of the relationships among child mental disorder stigma dimensions, contexts and targets
|
Media & marketing Health care practices |
Moderate |
| Nairn et al. 2011Footnote 27 | No restriction | Review (narrative) | Individuals living with mental health issues |
|
Media & marketing | Moderate |
| Pescosolido et al. 2008Footnote 33 | No restriction | Review (narrative) | Individuals living with mental illness | Framework proposed: framework integrating normative influence on stigma
|
Welfare policy Media Biomedical technology |
Moderate |
| Phelan et al. 2014Footnote 77 | No restriction | Review (narrative) | General population |
|
Social & built environment Media & marketing Public health interventions |
Strong |
| Schabert et al. 2013Footnote 50 | No restriction | Review (narrative) | Individuals living with diabetes | Framework proposed: a framework for understanding diabetes-related stigma (structural mitigating strategies: social marketing, education, counselling, health promotion)
|
Media & marketing Pedagogy Public health interventions |
Strong |
| White Hughto et al. 2015Footnote 58 | United States | Review (narrative) | Individuals identifying as transgender | Framework proposed: modified social-ecological model of transgender stigma and stigma interventions (structural interventions: policies against discrimination, promoting access to care, or curricula on the health of trans people)
|
Legal frameworks Welfare policy Pedagogy Diagnostic frameworks |
Moderate |
| Williams 2018Footnote 35 | United Kingdom | Review (narrative) | Individuals living with mental health issues |
|
Legal frameworks Economic policy Media & marketing Diagnostic frameworks |
Moderate |
| Clement et al. 2013Footnote 36 | No restriction | Review (systematic) | Individuals living with mental health issues |
|
Media & marketing | Strong |
| Craig et al. 2017Footnote 49 | Low TB–incidence countries | Review (systematic) | People living with TB in low-incidence countries (Western Europe, USA, Canada, Australia, New Zealand) |
|
Media & marketing Health care policy Public health interventions |
Strong |
| Darlington et al. 2017Footnote 43 | United States | Review (systematic) | Women living with HIV |
|
Legal frameworks Pedagogy Health care policy |
Strong |
| Katz et al. 2013Footnote 44 | United States | Review (systematic) | Individuals living with HIV |
|
Health care practices and policy | Strong |
Abbreviations: AIDS, acquired immunodeficiency syndrome; DSM, Diagnostic and Statistical Manual of Mental Disorders; ERs, emergency rooms; FASD, fetal alcohol spectrum disorder; HIV, human immunodeficiency virus; LGB, lesbian, gay, bisexual; MSM, men who have sex with men; NGOs, nongovernmental organizations; PEP, post-exposure prophylaxis; PrEP, pre-exposure prophylaxis; SAT, scholastic assessment tests; STBBI, sexually transmitted and blood-borne infection; TB, tuberculosis. |
||||||
| Author, year | Design | Are the aims and objectives of the research clearly stated? | Is the research design clearly specified? | Is the research design appropriate for the aims and objectives of the research? | Do the researchers provide a clear account of the process by which their findings were produced? | Do the researchers display enough data to support their interpretations and conclusions? | Is the method of analysis appropriate? | Is the method of analysis adequately explicated? | Total score (/7) |
|---|---|---|---|---|---|---|---|---|---|
| Clair et al. 2016Footnote 46 | Mixed methods sequential design | Yes, to examine how cultural constructions of stigmatized groups shift over time | No, the authors do not specify the study design | Yes, a narrative review is appropriate for an overview of current understanding | No, the review describes key concepts without sufficient details to reproduce the content | Yes, each concept is sufficiently referenced | Yes, the authors used a “systematic process analysis approach,” which is appropriate for the objectives | No, the authors do not explain how they applied their “systematic process analysis approach” | 4 |
| Coreil et al. 2010Footnote 48 | Mixed methods sequential design | Yes, to investigate the influence of structural forces on TB-related stigma among Haitians living in the US and Haiti | Yes, the authors specify that they used a mixed-methods design, and clearly describe the two phases | Yes, the design is aligned with the questions asked by the researchers | Yes, the methods are clear and reproducible | Yes, results of each phase are clearly provided | Yes, the methods of analysis are appropriate for each phase and objective | Yes, the analyses pertaining to both phases of the study are well explained | 7 |
| Henderson et al. 2017Footnote 68 | Mixed methods sequential design | Yes, to examine how differences in understanding of the etiology of addiction influence stigma attribution | Yes, the authors use a mixed-method study using a sequential design approach (with three phases, each building on the last), with each phase clearly described | Yes, the study builds on the results of each phase using a sequential approach | Yes, each of the data collection methods is well described | Yes, results of each phase are clearly described, and justification of qualitative coding was provided | Yes, analysis of the available data is appropriate | Yes, the authors provide sufficient detail on coding of qualitative themes and quantitative analyses | 7 |
| MacLean 2018Footnote 47 | Mixed methods sequential design | No, to identify determinants of STBBI-related stigma and propose a conceptual framework | No, the authors describe various components of the project without specifying a design | Yes, the activities conducted were appropriate for the objectives | No, data on each of the phases is lacking (e.g. selection approach, analysis, etc.) | No, very little data is presented for each of the sections | No, due to the lack of detail provided, it is impossible to judge whether the method of analysis is appropriate | No, very few details on the method of analysis are presented | 1 |
| Arrey et al. 2017Footnote 55 | Qualitative | Yes, to investigate stigma and discrimination among migrant sub-Saharan African women in health care settings in Belgium | Yes, the authors use a mixed-qualitative approach for data collection and analysis | Yes, the mixed-methods approach is appropriate for the objective | Yes, the sampling strategy and data collection methods are clearly described | Yes, the authors summarize the key themes identified, and provide direct quotes to support their observations | Yes, the method of analysis is appropriate for the available data and research question | Yes, the authors used an inductive thematic analysis approach | 7 |
| France et al. 2015Footnote 41 | Qualitative | Yes, to identify core beliefs underlying self-stigma in PLHIV in Ireland | Yes, the authors describe their data collection strategy and sample | Yes, qualitative research design is appropriate, especially to identify beliefs | Yes, they describe their method of data collection and coding | Yes, the authors summarize the key themes identified, and provide direct quotes to support their observations | Yes, the method of analysis is appropriate for the available data and research question | Yes, the coding strategy is well explained, as are approaches used to assess saturation | 7 |
| Hansen et al. 2014Footnote 73 | Qualitative | Yes, to describe the experience of structural stigma imposed by medicalization of public support for the poor | Yes, the authors use an ethnographic interview-based design | Yes, the qualitative approach is appropriate for the objective | Yes, data collection and analyses were clearly described | No, the authors provide only one case study to illustrate each identified theme | Yes, the method of analysis is appropriate for the available data and research question | Yes, the authors used iterative thematic coding techniques | 6 |
| Paterson et al. 2013Footnote 65 | Qualitative | Yes, to identify structural determinants of stigma of patients in emergency departments who use illicit drugs and are HCV+ | Yes, the authors use an inductive qualitative design approach | Yes, the qualitative approach is appropriate | Yes, they describe their method of data collection and coding | Yes, the authors summarize the key themes identified, and provide direct quotes to support their observations | Yes, the interpretive description design analytical approach is appropriate | Yes, the analytical approach is clearly described | 7 |
| Woodgate et al. 2017Footnote 40 | Qualitative | Yes, to understand the experiences and needs of Indigenous PLHIV who were diagnosed young | Yes, the authors clearly describe their sampling, data collection and analysis approach | Yes, the qualitative approach is appropriate for the objective and population | Yes, the authors clearly describe their sampling, data collection and analysis approach | Yes, the authors summarize the themes identified, and provide quotes to support them | Yes, the method of analysis is appropriate for the available data and research question | Yes, the authors explain their deductive thematic analysis approach | 7 |
| Jorm et al. 2008Footnote 79 | Quantitative (cross-sectional) | Yes, to assess whether social distance and belief in dangerousness are increased in those who believe in genetic causes of psychiatric illness; and whether social distance is reduced by belief in psychosocial causes | Yes, the authors clearly specify the design, including details on data collection and analysis | No, the design appears to be appropriate for the first objective, but not for the second objective, as it implies the effect of an intervention and the study was not designed to answer this question | Yes, the authors describe data available, the analyses conducted | No, it is unclear whether results are adjusted for known covariates, and the results of the linear models are difficult to interpret | Yes, analyses appear to be appropriate given available data and operationalization of study measures | Yes, the authors describe data available, the analyses conducted | 5 |
| Min et al. 2017Footnote 39 | Quantitative (cross-sectional) | Yes, to examine community factors as correlates of perceived and experienced stigma in a community sample of persons with mental illness | Yes, the authors clearly specify the design, including details on data collection and analysis | Yes, the cross-sectional design is appropriate for the objective | Yes, the authors describe data available, the analyses conducted | Yes, descriptive and analytic results are presented | Yes, the modelling strategy is appropriate given the nested nature of the data within health centres | Yes, the authors describe data available, the analyses conducted | 7 |
| Pachankis et al. 2017Footnote 69 | Quantitative (cross-sectional) | Yes, to investigate 6 structural determinants of stigma predicting lack of HIV-prevention in MSM migrants | Yes, cross-sectional study involving large-scale international survey | Yes, prospective data collection appropriate for the research question | Yes, operational definitions of all variables clearly provided, and resources provided for justification and validation | Yes, sufficiently large sample, sufficient variation in exposure to allow for analysis, and linkage to external measures | Yes, two-level cross-classified model reflecting hierarchical nature of the research question | Yes, statistical analysis plan and modelling strategy explained sufficiently to allow for reproduction | 7 |
| Stringer et al. 2016Footnote 78 | Quantitative (cross-sectional) | Yes, to examine the relationship between HIV stigma and individual/clinic–level characteristics and policies among health care workers in the Southern US | Yes, the authors clearly specify the design, including details on data collection and analysis | Yes, the cross-sectional design is appropriate for the objective | Yes, the authors describe data available, the analyses conducted | Yes, descriptive and analytic results are presented | No, the modelling strategy did not take into consideration the nested nature of the data within health centres | Yes, the authors describe data available, the analyses conducted | 6 |
| Stuber et al. 2008Footnote 64 | Quantitative (cross-sectional) | Yes, to examine 5 domains of stigma contributing to stigma among smokers | Yes, cross-sectional study involving survey data | Yes, prospective data collection appropriate for the research question | Yes, participant selection and methodology clearly explained, question items listed verbatim | Yes, sample size sufficiently large, authors show data for each of their 5 proposed domains of stigma | Yes, the authors used a regression model, weighted to correct for sampling bias | Yes, the analytical methodology is explained sufficiently to allow for reproduction | 7 |
| Angermeyer et al. 2014Footnote 75 | Quantitative (longitudinal) | Yes, to investigate whether the individual and structural stigma develop similarly | Yes, the authors clearly specify the design, data collection and analysis | Yes, the repeat cross-sectional design is appropriate for the objective | Yes, the authors describe data available, the analyses conducted | Yes, descriptive and analytic results are presented | Yes, the modelling strategies and estimation of probabilities is appropriate | Yes, the authors describe data available, the analyses conducted | 7 |
| Hatzenbuehler et al. 2015Footnote 70 | Quantitative (longitudinal) | No, the authors do not explicitly state an objective, but studied sexual orientation–related disparities in past-year illicit drug use and the influence of structural stigma | Yes, the authors use an observational, cohort-based design based on survey data | No, the objective of the study is unclear, and it is not possible to assess appropriateness | Yes, the authors describe available data and analyses conducted | No, only two results tables are presented, and several results are missing | Yes, analyses appear to be appropriate given available data | Yes, the authors describe data available, the analyses conducted | 4 |
| Arboleda-Florez et al. 2012Footnote 29 | Review (narrative) | Yes, to describe stigma associated with mental illness, stigmatization by health providers, and approaches for stigma reduction | Yes, the authors describe this as a narrative review of psychological and social literature | Yes, a narrative review is appropriate for the descriptive aims | No, the authors do not provide any details explaining how they arrived at their narrative synthesis | No, the authors cite few studies, and the lack of research in this field is a major limitation | Yes, a narrative summary of results is appropriate for the aims | No, there are no details on how analysis was conducted or what elements guided the synthesis | 4 |
| Aste 2016Footnote 53 | Review (narrative) | Yes, to describe the literature on the sources of stigma for individuals with chronic pain | Yes, the author describes the review as an “exploratory literature review” | Yes, the scoping review approach is appropriate for the objectives | Yes, the search strategy is well described, including clear selection criteria | Yes, sufficient evidence has been identified to support each concept | Yes, each included study is described in detail | No, there are no details on how analysis was conducted or what elements guided the synthesis | 6 |
| Bell et al. 2016Footnote 63 | Review (narrative) | Yes, to propose a descriptive model of FASD stigma, identify knowledge gaps, and discuss ethical implications of stigma | No, the authors do not specify their research design | Yes, a narrative synthesis is appropriate for the study aims | No, the authors do not describe how they selected or appraised supporting works for this framework | Yes, the authors provide a thorough theoretical foundation for included concepts | Yes, the authors have synthesized relevant literature to support their framework | Yes, the authors detail the process by which they identified domains in their framework | 5 |
| Benoit et al. 2018Footnote 60 | Review (narrative) | Yes, to review the state of research pertaining to the stigmatization of sex workers | No, the authors state that they are “reviewing evidence” but do not specify design | Yes, a narrative synthesis is appropriate for the descriptive aims | No, the authors do not describe how they selected or appraised supporting works for inclusion | Yes, the authors provide an in-depth synthesis of the state of research, and thoroughly cite all concepts | Yes, a synthesis of available evidence pertaining to the topic of interest is sufficient for the descriptive aims | No, there is no explanation of the analytical process or how synthesized information guided the summary | 4 |
| Bonsack et al. 2013Footnote 31 | Review (narrative) | Yes, to describe the concept of stigma and examine various interventions to reduce stigma | No, the authors do not specify their research design | Yes, a narrative summary is sufficient for the descriptive aims | No, there are no details of how relevant information was identified | No, very few works are cited as supporting evidence | Yes, a brief summary of the theory of mental health is sufficient for the aims | No, there are no details on how analysis was conducted or what elements guided the synthesis | 3 |
| Brewis 2014Footnote 62 | Review (narrative) | Yes, to identify mechanisms by which stigma may contribute to the perpetuation of obesity | No, the author simply describes their work as a review/synthesis | Yes, a narrative review is appropriate for the descriptive aims | No, the author does not detail the process by which supporting works were identified and included | Yes, the author provides support for each proposed mechanism | Yes, a narrative summary of results is appropriate for the descriptive aims | No, there are no details on how analysis was conducted or what elements guided the synthesis | 4 |
| Carroll 2017Footnote 61 | Review (narrative) | Yes, to investigate experiences of stigma among single mothers in diverse socioeconomic circumstances | Yes, the author conducts a narrative review of stigma theory as it applies to lone motherhood | Yes, a narrative summary of concepts followed by qualitative study supporting the author’s conclusions is appropriate for the study aims | Yes, the author describes the literature review process, and details how identified works contributed to the design and content | Yes, the author has thoroughly cited the theoretical groundwork, and provided a robust qualitative study to support the conclusions | Yes, a narrative synthesis of relevant research and semi-structured interview is appropriate for the study aims | Yes, the author clearly describes the methods used to synthesize sources to guide the narrative review and the analytical process used to extract key themes | 7 |
| Chaudoir et al. 2013Footnote 66 | Review (narrative) | Yes, to propose a framework that describes how stigma leads to psychological and physical health disparities | No, the authors do not specify their research design | Yes, a theoretical summary is appropriate for the proposal of a novel framework | No, the authors do not describe how they selected or appraised supporting works for this framework | Yes, the authors provide sufficient citations to support the proposed the causal pathways in their framework | Yes, a summary of supporting evidence for the framework is appropriate for the study aims | No, the authors do not detail how supporting works were synthesized in order to generate the framework | 4 |
| Collins et al. 2013Footnote 32 | Review (narrative) | Yes, to review evaluations of mental illness stigma reduction efforts in order to inform policy in California | No, the authors do not specify their research design | No, as the review is aimed at guiding policy, a more systematic review would have been more appropriate | No, the authors specify databases and keywords used, but not in sufficient detail to know how works were selected | Yes, each concept is referenced, offering an overview of included sources | Yes, a synthesis of key types of interventions is appropriate for the aim of the review | No, there are no details on how analysis was conducted or what elements guided the synthesis | 3 |
| Livingston, JD. (Commission de la santé mentale du Canada), 2013Footnote 37 | Review (narrative) | No, the authors do not state a specific aim, they introduce structural stigma in the context of modern institutional and social systems and examine tools to address stigma | No, the authors describe this work simply as a “report” | Yes, a narrative review of the concepts and tools to address stigma is sufficient | No, the authors do not provide an explanation of how they identified works for inclusion | Yes, the authors provide a well-cited summary of the state of knowledge in the field and of the Canadian context in support of their conclusions | Yes, a narrative description of the state of knowledge is appropriate for the descriptive aims of this study | No, the authors do not provide details regarding how the supporting evidence was synthesized or contributed to recommendations | 3 |
| National Academies of Sciences, Engineering, and Medicine (Committee on the Science of Changing Behavioral Health Social Norms), 2016Footnote 34 | Review (narrative) | Yes, to review the current understanding of stigma, its determinants, and targets for intervention | No, the authors do not specify their research design | Yes, the narrative review approach is appropriate for the aims | No, the review describes key concepts without sufficient details to reproduce the content | Yes, each concept is referenced, offering an overview of included sources | Yes, synthesis of key theoretical concepts is appropriate for the aim of the review | No, there are no details on how analysis was conducted or what elements guided the synthesis | 4 |
| De Ruddere & Craig 2016Footnote 52 | Review (narrative) | Yes, to describe current understanding of stigma pertaining to chronic pain | Yes, the authors use the term “topical review” to describe the design | Yes, the narrative review approach is appropriate for the descriptive aim | No, the narrative review describes concepts without sufficient detail to reproduce results | Yes, each concept is referenced, offering an overview of included sources | Yes, synthesis of key theoretical concepts is appropriate for the study aim | No, there are no details on how analysis was conducted or what guided the synthesis | 5 |
| Désy et al. 2013Footnote 76 | Review (narrative) | Yes, to describe stigma, explore the ethical dimensions of stigma and propose a reflection tool to assist public health stakeholders | No, the authors do not specify their research design | Yes, a narrative review of evidence is appropriate for the aims and target audience of this report | No, the authors describe their search (databases, search terms), without sufficient detail to reproduce the content | No, the authors cite a very limited number of studies | Yes, a summary of the field of stigma and ethics research is appropriate for the objectives of this report | No, there are no details on how analysis was conducted or what elements guided the synthesis | 3 |
| Earnshaw et al. 2015Footnote 42 | Review (narrative) | Yes, to propose a framework that describes how societal stigma can lead to physical and psychological health disparities | No, the authors do not specify their research design | Yes, a theoretical summary and review of supporting evidence is appropriate for the proposal of a novel framework | No, the authors do not describe how they selected or appraised supporting works for this framework | Yes, the authors conduct a thorough assessment of the supporting evidence, and each component of the framework is well referenced | Yes, a summary of supporting evidence for the framework is appropriate for the study aims | No, there is no explanation of how included works were synthesized in order to generate the framework | 4 |
| Fernandes et al. 2011Footnote 51 | Review (Narrative) | Yes, to describe epilepsy stigma, and consider the influence of legislation on power imbalances | No, the authors do not specify their research design | Yes, a narrative review is appropriate for the descriptive aims | No, the authors provide no explanation of how information for this review was obtained/selected | Yes, theories are supported with sufficient citations and consider the availability and quality of evidence | Yes, a synthesis of existing research is appropriate for the generation of a conceptual novel framework | No, there is no explanation of how included works were synthesized | 4 |
| Golub 2018Footnote 26 | Review (narrative) | Yes, to review the role of PrEP-related stigma in access and adherence to PrEP, and examine its antecedents and consequences | No, the design is not clearly specified | Yes, a narrative review is appropriate for the descriptive aims | No, the authors do not specify how they selected works to include in their review | Yes, the authors have cited a wide range of literature, lending support to their conclusions | Yes, synthesis of key theoretical concepts is appropriate for the objectives | No, no detail is provided regarding how the included works were synthesized | 4 |
| Groulx 2011Footnote 59 | Review (narrative) | Yes, to summarize the factors driving social exclusion, and describe their manifestations in Canadian society | Yes, the authors state that they will use a narrative review design | Yes, the narrative review approach is appropriate | Yes, the search strategy is well described, including a description of inclusion criteria | Yes, each concept is referenced, offering an overview of included sources | Yes, synthesis of key theoretical concepts is appropriate for the aim of the review | No, there are no details on how analysis was conducted or what elements guided the synthesis | 6 |
| Hatzenbuehler 2016Footnote 8 | Review (narrative) | Yes, to review structural stigma related to mental illness and sexual orientation | No, the author simply describes the work as a review | Yes, a narrative review is appropriate for the descriptive aims | No, the author does not describe how works were selected for inclusion | Yes, concepts are well supported by theoretical evidence and empirical research | Yes, a narrative summary of theoretical and empirical research is appropriate for the descriptive aim | No, there are no details on how analysis was conducted or what elements guided the synthesis | 4 |
| Hatzenbuehler 2014Footnote 57 | Review (narrative) | Yes, to describe structural stigma as a risk indicator for psychiatric and physical-health morbidities among LGBT populations | No, the author describes the work as a review | Yes, a narrative review is appropriate for the descriptive aims | No, the author does not describe how works were selected for inclusion | Yes, the assertions are supported by citing a varied body of research, and comments on the methodological rigour of studies | Yes, a narrative summary of results is appropriate for the study aims | No, there is no explanation of the analytical process that contributed to the synthesis of included works | 4 |
| Holder et al. 2019Footnote 30 | Review (narrative) | Yes, to describe how mental health stigma discourages treatment-seeking | No, the authors describe it only as a “theoretical paper based on literature” | Yes, a narrative review is appropriate given the descriptive aim | No, the authors do not describe how works were selected for inclusion | Yes, the authors cite a wealth of resources from academic and grey literature | Yes, a theoretical review of literature is appropriate for the aim and design | No, there is no explanation of the analytical process contributing to the overall synthesis | 4 |
| Kerr et al. 2016Footnote 45 | Review (narrative) | Yes, to propose a novel conceptual framework and examine mechanisms leading to disparities in HIV risk for racialized communities | No, the authors do not specify their research design | Yes, a narrative review of evidence and proposed framework is appropriate for the proposal of a novel framework | No, the authors do not describe how they selected or appraised supporting works for this framework | Yes, the authors are proposing a complex model, and cite a large and diverse body of research to support their claims | Yes, a summary of supporting evidence for the framework is appropriate for the study aims | No, there is no explanation of how included works were synthesized in order to generate the framework | 4 |
| Knapp et al. 2014Footnote 54 | Review (narrative) | Yes, to describe the identity-threat model of stigma and adapt it to cancer stigma | Yes, the authors describe this as a review and application of stigma theory | Yes, the narrative review design is appropriate for the descriptive aims | Yes, the authors are adapting an established theory, however they do not describe the identification of supporting works | Yes, all concepts in the article are thoroughly cited, and the authors' analysis is based on a well-known theory of stigma | Yes, the authors have synthesized and summarized the salient points in the literature to support their conclusions | No, the authors do not describe how their synthesis was guided by included works | 6 |
| Link & Hatzenbuehler 2016Footnote 72 | Review (narrative) | Yes, to explore the impact of stigma on health via processes of social disadvantage | No, the authors do not specify their research design | Yes, a narrative review is appropriate for the descriptive aims | No, the authors describe concepts in the literature without detailing how they identified relevant works | Yes, all concepts are thoroughly cited, and the first author is an authority in this field of research | Yes, the authors have provided a theoretical conceptualization based on existing research | No, there are no details on how analysis was conducted or what elements guided the synthesis | 4 |
| Ministère de la Santé et des Services sociaux Québec, 2016Footnote 38 | Review (narrative) | Yes, to summarize anti-stigma strategies for use in health care settings, in order to guide intervention | No, the authors do not specify their research design | No, a more systematic review with a quality assessment would have been more appropriate | No, the review describes key concepts without sufficient details to reproduce the content | No, the authors cite a very limited number of studies | No, synthesis of key theoretical concepts is not appropriate to guide intervention | No, there are no details on how analysis was conducted or what elements guided the synthesis | 1 |
| Mirabito et al. 2016Footnote 67 | Review (narrative) | Yes, to propose a novel conceptual framework and analyze its contribution to the understanding of marketplace stigma | No, the authors do not specify their research design | Yes, a summary of supporting theories and explanation of the proposed framework is appropriate | No, the authors do not describe how they arrived at this formulation of their conceptual framework | Yes, the authors provide an adequate explanation of their framework, with citations supporting each of the components | Yes, the authors have conducted an analysis of the implications of their framework on the understanding of stigma | No, there are no details on how analysis was conducted or what elements guided the synthesis | 4 |
| Morey 2018Footnote 56 | Review (narrative) | Yes, to describe the mechanisms by which anti-immigrant stigma exacerbates ethnic health disparities | No, the author does not specify a research design | Yes, a short description of the research on this topic is sufficient for the objectives | No, there is no description of how these findings were identified | Yes, the proposed mechanisms are well cited | Yes, a narrative summary of supporting evidence is appropriate | No, no explanation of how supporting information was analyzed or integrated is provided | 4 |
| Mukolo et al. 2010Footnote 28 | Review (narrative) | Yes, to describe the literature on stigma associated with children’s mental disorders and highlight gaps in empirical work | No, the authors simply call this paper a “review,” and it is not clear if they mean to be systematic | Yes, a narrative review is appropriate for the descriptive aims | Yes, the authors detail their search strategy (databases, date ranges, search terms) and inclusion/exclusion criteria | No, the concepts introduced are thoroughly cited, but many of their sources are from literature on adults | Yes, a narrative summary of results is appropriate for the aims | Yes, the authors describe how they appraised the convergence of definitions of critical dimensions of stigma | 5 |
| Nairn et al. 2011Footnote 27 | Review (narrative) | Yes, to provide a framework of the role of cultural mechanisms in media depictions of mental illness | No, the design is not clearly specified | Yes, the narrative review approach is appropriate for the objectives | No, the narrative review describes concepts without sufficient detail to reproduce the content | Yes, each concept is referenced, offering an overview of included sources | Yes, synthesis of key theoretical concepts is appropriate for the aim of the review | No, there are no details on how analysis was conducted or what elements guided the synthesis | 4 |
| Pescosolido et al. 2008Footnote 33 | Review (narrative) | Yes, to propose a novel conceptual framework describing the determinants of stigma, focussing on mental health | No, the authors do not specify their research design | Yes, a narrative review of existing evidence and of the components of the proposed framework is sufficient | No, the authors do not describe how they selected or appraised supporting works for this framework | Yes, each concept that the authors included in their framework is well referenced | Yes, a narrative summary of supporting evidence is sufficient | No, there is no explanation of how included works were synthesized in order to generate the framework | 4 |
| Phelan et al. 2014Footnote 77 | Review (narrative) | Yes, to propose a novel theory of stigma focussing on systemic aspects of stigma and their impact on health | Yes, the authors propose a narrative review of extant theories | Yes, a narrative summary is appropriate for the descriptive aims | No, the authors do not describe how the key works in stigma and status theory were identified | Yes, all concepts are thoroughly cited, and the first author is an authority in this field of research | Yes, a narrative summary of supporting evidence is sufficient for the descriptive aims | Yes, the authors describe their assessment process by identifying theoretical convergence | 6 |
| Schabert et al. 2013Footnote 50 | Review (narrative) | Yes, to develop a framework of the experiences, causes and consequences of diabetes stigma | Yes, the authors state that this is a narrative review | Yes, the narrative review approach is appropriate for the objective | No, the authors describe the search strategy (databases, search terms) but do not specify inclusion criteria | Yes, each concept is referenced, offering an overview of included sources | Yes, synthesis of key theoretical concepts is appropriate for the aim of the review | Yes, the authors explain how the extant literature was categorized | 6 |
| White Hughto et al. 2015Footnote 58 | Review (narrative) | Yes, to review the multiple levels of transgender stigma and how they influence health | No, the design is not clearly specified, it is defined simply as a “review” | Yes, the narrative review approach is appropriate for the objectives | No, the narrative review describes concepts without sufficient detail to reproduce the content | Yes, each concept is referenced, offering an overview of included sources | Yes, synthesis of key theoretical concepts is appropriate for the aim of the review | No, there are no details on how analysis was conducted or what elements guided the synthesis | 5 |
| Williams 2018Footnote 35 | Review (narrative) | Yes, to assess how personal, cultural and structural oppression affect individuals with affective distress, and the experience of self-stigma | No, the design is not clearly specified | Yes, the narrative review approach is appropriate for the objectives | No, the author does not describe how works were identified or selected | Yes, each concept is referenced, offering an overview of included sources | Yes, synthesis of key theoretical concepts is appropriate for the objectives | No, there are no details on how analysis was conducted or what elements guided the synthesis | 4 |
| Clement et al. 2013Footnote 36 | Review (systematic) | Yes, to assess the effects of mass media interventions on reducing mental health stigma | Yes, the authors conducted a systematic review of published literature | Yes, a systematic review is appropriate for the study aims | Yes, the authors list and justify selection criteria, list databases and provide a complete search strategy | Yes, the authors have identified and included a sufficient number of works to support their conclusions | Yes, a narrative synthesis and meta-analysis are appropriate for the study aims | Yes, the authors conducted a narrative synthesis of qualitative studies and meta-analysis of qualitative studies | 7 |
| Craig et al. 2017Footnote 49 | Review (systematic) | Yes, to explore the inclusion and conceptualization of stigma in research about TB in low incidence settings | Yes, the authors conducted a systematic mapping review to map/categorize the existing body of TB research | Yes, the systematic mapping review is appropriate for the goals of this study | Yes, clear description of search strategy (databases, search terms, inclusion criteria) | Yes, the authors use a detailed search strategy, and sufficient studies were identified to support each category in the mapping process | Yes, systematic mapping review of literature on TB-related stigma appropriate for the authors’ objectives | Yes, the authors list specific analytical questions and provide an overview of the articles that addressed each question | 7 |
| Darlington et al. 2017Footnote 43 | Review (systematic) | Yes, to analyze the state of knowledge regarding HIV-related stigma among women in the Southern US | Yes, the authors conducted a systematic review of published literature | Yes, a systematic review is appropriate for the study aims | Yes, the authors list databases, provide rough details about search strategy and list clear selection criteria | Yes, the authors thoroughly cite each concept they introduce with qualitative and quantitative studies | Yes, the narrative synthesis of studies is appropriate for the study aims | No, the authors do not mention how the contents of the included studies were analyzed or appraised in order to inform the synthesis | 6 |
| Katz et al. 2013Footnote 44 | Review (systematic) | Yes, to assess the relationship between the experience of HIV-related stigma and ART adherence | Yes, a systematic review and meta-analysis of published and unpublished literature | Yes, a systematic review is appropriate to describe a hypothesized causal mechanism | Yes, the authors provide a detailed description of their search (databases, search strategy, inclusion criteria, quality assessment) | Yes, the analysis was robust and well reported, and they identified sufficient works to conduct a meta-analysis | Yes, a meta-analysis and thematic meta-synthesis is appropriate for the objectives | Yes, the authors conducted a thematic meta-synthesis of qualitative studies, and meta-analysis of quantitative studies | 7 |
Abbreviations: ART, antiretroviral therapy; FASD, fetal alcohol spectrum disorder; HCV+, hepatitis-C-virus positive; HIV, human immunodeficiency virus; LGBT, lesbian, gay, bisexual, transgender; MSM, men who have sex with men; PLHIV, people living with human immunodeficiency virus; PrEP, pre-exposure prophylaxis; STBBI, sexually transmitted and blood-borne infection; TB, tuberculosis. |
|||||||||
Data analysis and synthesis
We performed a narrative synthesis of extracted data involving three analytic stages.Footnote 22 In the first stage, two authors conducted a thematic analysis of documented structural determinants of stigma.Footnote 23Footnote 24 Having become familiar with the data by generating initial summaries of structural determinants reported in included works during the data extraction process, these authors performed a thematic analysis, which involved identifying themes that linked structural determinants conceptually.Footnote 23Footnote 24 Themes were identified semantically (i.e. by interpreting factors that were explicitly mentioned in the texts rather than identifying underlying meanings) and inductively (i.e. without a predefined coding frame), through consensus.Footnote 25 We considered themes for which related structural factors were mentioned in at least two works, and that were internally coherent and conceptually distinct and definable.Footnote 24 Hereafter, these themes are described as “domains” of structural determinants.
At the second stage, we proposed a narrative synthesis of study types and characteristics and the identified domains and their relationship to the stigma process, as well as a visual conceptual framework of the domains and their relationship to the stigma process. The structuring of the elements in the conceptual framework was based both on the findings of included works and the structure of existing conceptual frameworks of the determinants of stigma.
The third and final stage consisted of summarizing the methodological quality of the included works. In order to provide a quantitative synopsis of quality appraisal results for this review, we considered studies with less than four “Yes” responses (< 60%) as weak, those receiving six or more “Yes” responses (> 85%) as strong, and the remainder as moderate. As these thresholds have not been validated, full annotated scoring results were also provided to complement quantitative summaries.
Results
The results of the narrative synthesis are presented here, beginning with a descriptive summary of study characteristics, followed by a summary of identified structural determinants.
Descriptive results
Study selection
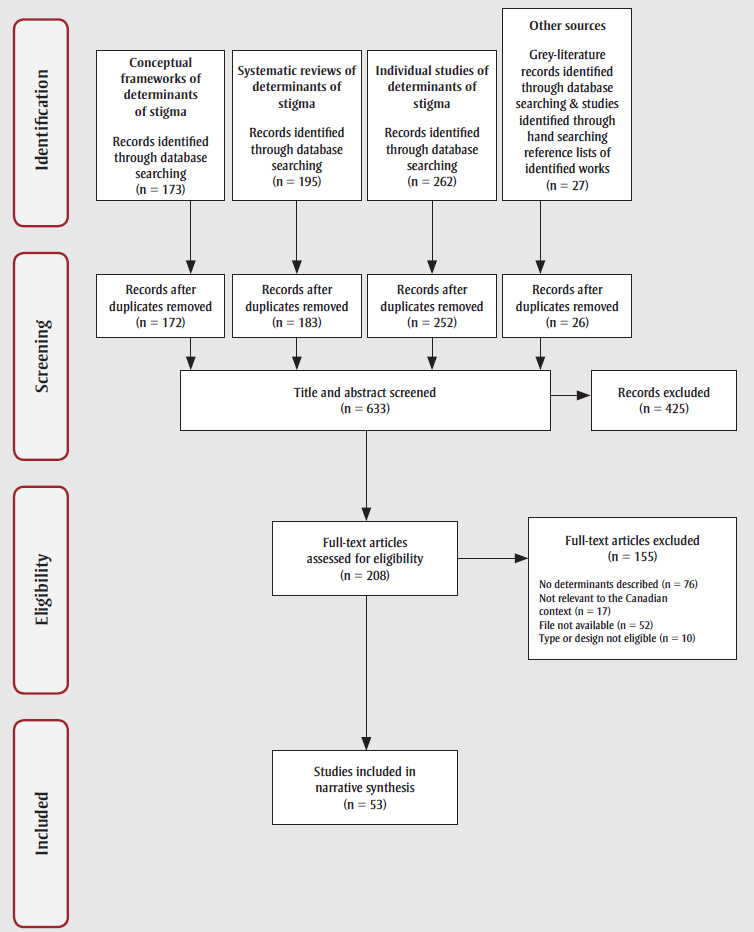
Overall, 657 works were identified through the search strategy. Figure 1 provides a summary of works identified. Four works—all grey literature sources—were written in French. After applying inclusion and exclusion criteria, 53 works were retained (Table 2). Most rejected works were those that did not document determinants of stigma that operate at a structural level. The retained works consisted of literature reviews (n = 37; 69%), and individual mixed-method (qualitative and quantitative; n = 4; 8%), qualitative (n = 5; 9%) and quantitative (n = 7; 13%) studies. Most reviews were not limited to a specific country setting, while individual studies were predominantly based in specific geographic regions including the United States (n = 14), Canada (n = 8) and Europe (n = 5) (Table 2).
Figure 1. Flow diagramFootnote a of data identification, selection and extraction
Text description: Figure 1
| Level (Top to Bottom) |
Position (Left to Right) | Arrow to | Text |
|---|---|---|---|
| 1 (Identification) | 1 | 2-1 | Conceptual frameworks of determinants of stigma Records identified through database searching (n = 173) |
| 2 | 2-2 | Systematic reviews of determinants of stigma Records identified through database searching (n = 195) |
|
| 3 | 2-3 | Individual studies of determinants of stigma Records identified through database searching (n = 262) |
|
| 4 | 2-4 | Other sources Grey-literature records identified through database searching & studies identified through hand searching reference lists of identified works (n = 27) |
|
| 2 (Screening) | 1 | 3-3 | Records after duplicates removed (n = 172) |
| 2 | 3-3 | Records after duplicates removed (n = 183) | |
| 3 | 3-3 | Records after duplicates removed (n = 252) | |
| 4 | 3-3 | Records after duplicates removed (n = 26) | |
| 3 (Screening) | 3 | 4-3, 3-5 |
Title and abstract screened (n = 633) |
| 5 | N/A | Records excluded (n = 425) | |
| 4 (Eligibility) | 3 | 5-3 | Full-text articles assessed for eligibility (n = 208) |
| 5 | N/A | Full-text articles excluded (n = 155) No determinants described (n = 76) Not relevant to the Canadian context (n = 17) File not available (n = 52) Type or design not eligible (n = 10) |
|
| 5 (Included) | 3 | N/A | Studies included in narrative synthesis (n = 53) |
Quality appraisal
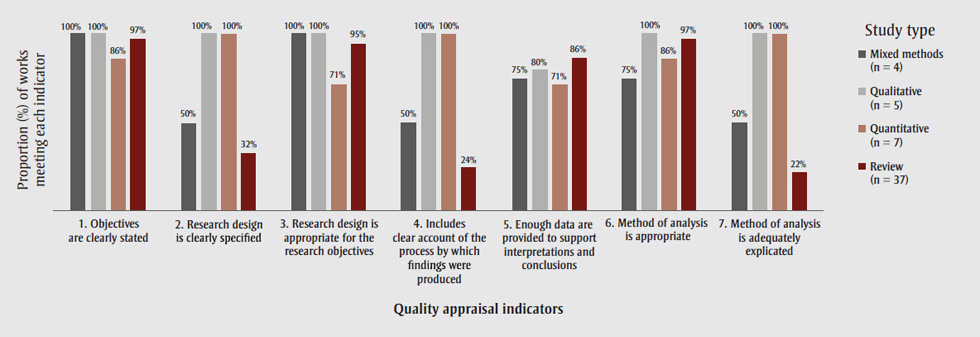
Most publications were moderate or strong in quality. The weakest element of the publications was a lack of detail on the design processes by which findings and interpretations were produced (Table 3). This element tended to be absent from works from the social sciences, which made up a large proportion of the included literature. This is a limitation of extant reviews of structural determinants of stigma. Figure 2A provides a summary of the mean score on each of the quality appraisal questions by study type, and Figure 2B provides an overview of the quality of works supporting each identified structural domain, described later on.
Figure 2. Summary of the quality appraisal assessment of identified works (N = 53), across study types and domains of structural determinants of stigma
Figure 2a. Proportion of works by study type meeting each quality appraisal indicator
Text description: Figure 2a
| Quality appraisal indicators | Proportion (%) of works meeting each indicator | |||
|---|---|---|---|---|
| Mixed methods (n=4) | Qualitative (n=5) | Quantitative (n=7) | Review (n=37) | |
| 1. Objectives are clearly stated | 100 | 100 | 86 | 97 |
| 2. Research design is clearly specified | 50 | 100 | 100 | 32 |
| 3. Research design is appropriate for the research objectives | 100 | 100 | 71 | 95 |
| 4. Includes clear account of the process by which findings were produced | 50 | 100 | 100 | 24 |
| 5. Enough data are provided to support interpretations and conclusions | 75 | 80 | 71 | 86 |
| 6. Method of analysis is appropriate | 75 | 100 | 86 | 97 |
| 7. Method of analysis is adequately explicated | 50 | 100 | 100 | 22 |
Figure 2b. Number and proportion of works supporting each identified domain of structual determinants by overall appraisal score
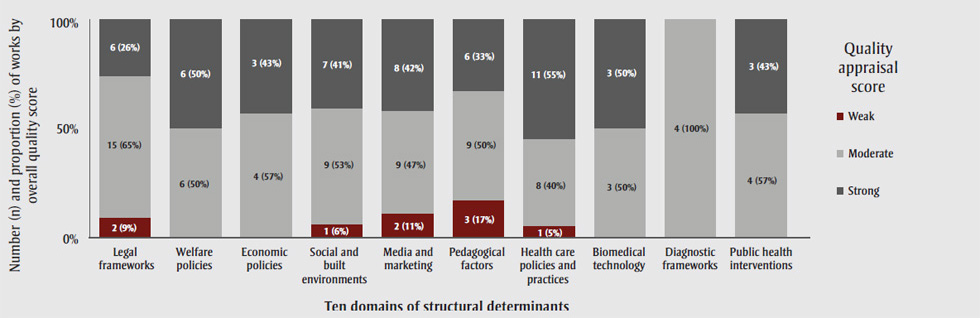
Text description: Figure 2b
| Ten domains of structural determinants | Number (n) and proportion (%) of works by overall quality score | ||
|---|---|---|---|
| Weak | Moderate | Strong | |
| Legal frameworks | 2 (9%) | 15 (65%) | 6 (26%) |
| Welfare policies | 0 (0%) | 6 (50%) | 6 (50%) |
| Economic policies | 0 (0%) | 4 (57%) | 3 (43%) |
| Social and built environments | 1 (6%) | 9 (53%) | 7 (41%) |
| Media and marketing | 2 (11%) | 9 (47%) | 8 (42%) |
| Pedagogical factors | 3 (17%) | 9 (50%) | 6 (33%) |
| Health care policies and practices | 1 (55%) | 8 (40%) | 11 (55%) |
| Biomedical technology | 0 (0%) | 3 (50%) | 3 (50%) |
| Diagnostic frameworks | 0 (0%) | 4 (100%) | 0 (0%) |
| Public health intervention | 0 (0%) | 4 (57%) | 3 (43%) |
Study characteristics
The identified works overwhelmingly cited Link and Phelan’sFootnote 1 conceptualization of stigma as a process driven by social, economic and political power inequities, through which attitudes, negative stereotypes and a sense of separation between groups can lead to discrimination and status loss. The reviewed literature explored many stigmatized experiences, identities, behaviours and health conditions (Table 2). Comprehensively, these were: individuals with mental health and substance use disorders;Footnote 26Footnote 27Footnote 28Footnote 29Footnote 30Footnote 31Footnote 32Footnote 33Footnote 34Footnote 35Footnote 36Footnote 37Footnote 38Footnote 39 individuals living with human immunodeficiency virus (HIV)Footnote 26Footnote 40Footnote 41Footnote 42Footnote 43Footnote 44Footnote 45Footnote 46 or other sexually transmitted or blood-borne infections (STBBI),Footnote 47 tuberculosis (TB),Footnote 48Footnote 49 diabetes,Footnote 50 epilepsy,Footnote 51 chronic painFootnote 52Footnote 53 or cancer—particularly types whose etiology may be attributable to patients’ behaviours;Footnote 54 vulnerable subpopulations such as migrants and racialized communities;Footnote 55Footnote 56 lesbian, gay, bisexual, transgender, queer and other (LGBTQ+) populations;Footnote 57Footnote 58 individuals experiencing poverty;Footnote 59 sex workers;Footnote 60 single mothers;Footnote 61 individuals labelled as obese or fat;Footnote 46Footnote 62 biological mothers of children diagnosed with fetal alcohol spectrum disorder;Footnote 63 and individuals who smoke.Footnote 64 Some authors highlighted that, although their research may have focussed on stigma pertaining to a specific condition or identity, individuals can experience multiple sources of stigma due to the intersection of multiple complex identities and life experiences.Footnote 47Footnote 60 These authors acknowledged that restricted study scope could represent a potential limitation to their studies.
Lastly, among the works reviewed, 15 proposed conceptual frameworks that graphically represented at least one upstream determinant of stigma (Table 2).Footnote 28Footnote 32Footnote 33Footnote 40Footnote 41Footnote 42Footnote 45Footnote 46Footnote 47Footnote 50Footnote 58Footnote 63Footnote 65Footnote 66Footnote 67 However, none were intended to provide a comprehensive summary of known structural determinants of stigma across populations. Identified frameworks were heterogeneous in form and content. However, most frameworks included an acknowledgement that stigma could be enacted at many levels, such as the individual (internalized), interpersonal, community, institutional and societal levels. Many frameworks also acknowledged that stigma is influenced by historical social inequities, such as those relating to systemic racism.Footnote 46
Structural determinants of stigma
Thematic analysis of the reviewed literature yielded 10 overall domains of structural determinants of stigma (Table 2): (1) legal frameworks; (2) welfare policies; (3) economic policies; (4) social and built environments; (5) media and marketing; (6) pedagogical factors; (7) health care practices and policies; (8) biomedical technology; (9) diagnostic frameworks; and (10) public health interventions. A narrative synthesis of these domains and their relationship with stigma follows.
Legal frameworks
The domain of “legal frameworks” refers to factors pertaining to enacted or proposed legislation, including broad bills of rights, as well as downstream elements of criminal justice systems such as factors pertaining to policing, courts and corrections. Twenty-four works referenced terms that fell under this domain.Footnote 29Footnote 31Footnote 32Footnote 34Footnote 35Footnote 43Footnote 45Footnote 46Footnote 47Footnote 48Footnote 51Footnote 54Footnote 56Footnote 57Footnote 58Footnote 60Footnote 61Footnote 66Footnote 67Footnote 68Footnote 69Footnote 70Footnote 71Footnote 72 Examples of terms describing structural determinants under this domain include (but are not limited to) “laws,”Footnote 32 “legislative action,”Footnote 43 “legal protections,”Footnote 46 “Acts” (e.g. the United Kingdom’s Mental Health Act or Equality Act),Footnote 35 “policing” and “sentencing.”Footnote 45 Terms related to legal frameworks were mentioned in six existing frameworks.Footnote 32Footnote 45Footnote 46Footnote 47Footnote 58Footnote 67
Overall, legal frameworks were identified as potential levers to prevent the discrimination and status loss components of the stigma process. Legislation that enshrines individual rights in relation to employment,Footnote 57Footnote 60 housing,Footnote 43 marriage,Footnote 66Footnote 69 or immigrationFootnote 56—to name some of the areas referenced in reviewed works—can prevent inequitable access to health and social resources.Footnote 67 On the other hand, factors relating to legal frameworks can also enable discrimination. This can occur when existing legislation fails to protect the rights of certain populations (people living with HIV are one prominent exampleFootnote 43), when legislation restricts rights for certain groups (e.g. barring individuals with mental illnesses from serving on juries,Footnote 34 or prohibiting individuals with epilepsy from drivingFootnote 51), or when components of the criminal justice system such as policing or sentencing affect certain populations more than others.Footnote 46 The laws introduced during North America’s “War on Drugs,” referenced in several studies, are one of the most illustrative examples of the latter. These laws were described as influencing the stigma process by perpetuating negative stereotypes of individuals who committed drug-related crimes (e.g. using or selling illicit substances)Footnote 34 and enabling status loss of Indigenous, Black and racialized communities through disproportionate policing and incarceration.Footnote 45Footnote 66
Welfare policies
The domain of “welfare policies” refers to factors relating to the presence of, eligibility for and relative coverage or “generosity” of government-based structures, services and benefit programs that offer social, health or economic support for those in need. A non-exhaustive list of terms that led to the categorization of this domain included “welfare state,” “insurance,”Footnote 33 “child welfare system,”Footnote 40 “benefits”Footnote 73 and “social security.”Footnote 56 Twelve works used terms related to welfare policy,Footnote 33Footnote 37Footnote 40Footnote 45Footnote 55Footnote 56Footnote 58Footnote 59Footnote 61Footnote 64Footnote 66Footnote 73 of which two also referred to these terms in proposed conceptual frameworks.Footnote 33Footnote 40
Overall, the provision and coverage of social supports (or lack thereof) was noted across the included works as contributing to the stigma process via two principle mechanisms: by shaping societal beliefs about service or benefit recipients, and by influencing vulnerable populations’ access to protective and life-sustaining resources. Two examples of these welfare-related mechanisms include policies that disqualify individuals from welfare benefits or services based on certain statuses, such as those limiting immigrants’ eligibility for social services based on documentation status or length of time since immigration,Footnote 56 and “War on Drugs” policies that disqualify offenders from social protections such as access to public housing.Footnote 45 Both types of policies were identified as reinforcing negative societal perceptions of those who do not “merit” societal support, therefore legitimizing exclusion and negative stereotypes.Footnote 33 Similar processes can occur if welfare coverage is restricted for certain conditions, such as when health insurance coverage is limited for mental health servicesFootnote 37 or gender-affirming procedures,Footnote 58 to name two examples. Policies that disqualify certain populations from access to social supports contribute to the stigma process by creating systematic gaps in care and status loss for affected populations.
Economic policies
The domain of “economic policies” refers to factors pertaining to governmental influence on features of economic landscapes, including policies relating to labour market wage, income redistribution policies or budgetary funding allocation across sectors. Though minimum wage limits are set through legislation, they are grouped under this domain because of their effects on economic conditions such as hiring practices and labour market participation—factors connected to the economic landscape of political jurisdictions.Footnote 74 Eight works referred to terms pertaining to this domain,Footnote 33Footnote 35Footnote 37Footnote 59Footnote 60Footnote 62Footnote 64Footnote 75 including one which integrated the concept of economic policies in its proposed conceptual framework.Footnote 33 Examples of terms relating to this domain included “funding,”Footnote 75 “tax,”Footnote 37 “investment,”Footnote 37 “economic development”Footnote 33 and “minimum wage.”Footnote 59
Overall, governmental influence on economic environments was described as influencing the stigma process by determining how equitably (or inequitably) economic resources are distributed within a population—thereby both influencing socioeconomic positioning of groups and sending the implicit message to disenfranchised groups that their disadvantaged state is not worth addressing through public investment. One example of how economic policies can influence status loss was that limited budgetary resource allocation to health services and workplace support programs for those experiencing mental health issues can lead to gaps in care and social and economic exclusion for those affected.Footnote 35Footnote 37Footnote 75
Social and built environments
The domain of “social and built environments” refers to the characteristics of communities and places, at an aggregate level, in which individuals live, work or play—including population prevalence of certain health, social or economic conditions or elements of physical environments. Although they are likely influenced by elements that fall under preceding domains, such as economic or welfare policies, we consider socioecological environmental characteristics as a distinct domain. Seventeen works included terms pertaining to this domain,Footnote 34Footnote 37Footnote 39Footnote 41Footnote 42Footnote 48Footnote 53Footnote 57Footnote 61Footnote 62Footnote 64Footnote 66Footnote 67Footnote 70Footnote 72Footnote 75Footnote 76Footnote 77 including three conceptual frameworks.Footnote 41Footnote 42Footnote 66 A non-exhaustive list of terms relating to this domain included “environmental hazards,”Footnote 66 “residential segregation,”Footnote 42 “neighborhood disorder,”Footnote 39 “prevalence” of a health or social condition (e.g. depression)Footnote 75 and availability of social meeting “spaces.”Footnote 41
Overall, studies describe how characteristics at the level of the local area and the community can influence the stigma process by contributing to both real and perceived social separation between groups and by generating social stratification in resource access. One example of these mechanisms is the way racialized and lower-income communities are segregated across residential neighbourhoods, which can reduce contact between stigmatized and nonstigmatized groups and reinforce perceptions of social differentiation.Footnote 42Footnote 77 These exclusionary structures can contribute to economic deprivation,Footnote 48 differential exposure to hazardous environmental conditions such as unsafe work conditions, pollution or infectious disease,Footnote 66 and inequalities in access to health care facilitiesFootnote 34 or places of education and employment for excluded groups.Footnote 37 In contrast, social environments such as workplaces or residential areas with greater social diversity can foster more interactions between population subgroups, shift societal perceptions and beliefs and reduce inequities in resource access.Footnote 67Footnote 75
Media and marketing
The domain of “media and marketing” refers to factors pertaining to the content development and regulation of communications strategies of various forms, such as news media, broadcasting or advertising, designed for the purposes of entertainment and sales, or to promote changes in individuals’ behaviours. Nineteen works used terms pertaining to this domain.Footnote 27Footnote 28Footnote 32Footnote 33Footnote 34Footnote 35Footnote 36Footnote 37Footnote 48Footnote 49Footnote 50Footnote 54Footnote 55Footnote 56Footnote 60Footnote 61Footnote 67Footnote 76Footnote 77 Examples of terms relating to this domain included “media portrayals,”Footnote 32 “media coverage,”Footnote 37 “media context,”Footnote 33 “commercial”Footnote 67 and “social marketing.”Footnote 50 Five of the identified conceptual frameworks explicitly mentioned media- and marketing-related terms.Footnote 32Footnote 33Footnote 46Footnote 50Footnote 67
Media content and social marketing endeavours can influence the stigma process by shaping societal attitudes and beliefs, and by reinforcing or countering negative stereotypes, interpretations and attributions of blame. Media content can also serve as a proxy for social interaction with stigmatized groups. If direct contact with stigmatized populations is rare, media may act as the primary or sole source of information that impacts judgments made in everyday life about these individuals.Footnote 32Footnote 77 To illustrate, one example is media portrayals of people with mental illnesses that depict these individuals as dangerous, unpredictable and criminal, thereby inciting fear and perceptions of social differentiation (or “othering”).Footnote 27Footnote 28Footnote 37 Another example is media portrayals that reinforce beliefs that certain groups are to blame for the harms they experience, and are therefore less deserving of social support and inclusion.Footnote 48Footnote 54Footnote 60 These narratives can legitimize discrimination towards marginalized groups.Footnote 27Footnote 32Footnote 35Footnote 77
Media content can also reduce stigma by normalizing and promoting a greater understanding of certain behaviours or conditions.Footnote 28Footnote 48 Media content presenting positive and inclusive messaging, and including factual information about the causes, treatments and experiences of individuals with mental illness, can shift population-level misconceptions and negative stereotypes.Footnote 32
Pedagogical factors
The domain of “pedagogical factors” pertains to the structure, design and implementation of educational content (e.g. curricula) and teaching initiatives, as well as educational institutions. A sample of terms relating to this domain included “trainings,”Footnote 58 “curricula”Footnote 37 and “educational programs.”Footnote 68 Eighteen works referenced terms that fell under this domain.Footnote 29Footnote 30Footnote 31Footnote 32Footnote 34Footnote 37Footnote 38Footnote 40Footnote 43Footnote 46Footnote 50Footnote 51Footnote 52Footnote 53Footnote 55Footnote 58Footnote 68Footnote 72 Pedagogical factors were referenced in three conceptual frameworks.Footnote 32Footnote 50Footnote 58
These works described how both the form and the content of educational material can influence the stigma process. Overall, much like media content, pedagogical factors can influence the stigma process by shaping societal attitudes and beliefs. Across studies, it was noted that pedagogical material that promotes or enables direct contact between the public and stigmatized individuals,Footnote 38Footnote 50Footnote 51 that tackles misinformationFootnote 32 including negative stereotypesFootnote 29 and that normalizes stigmatized behaviours can reduce stigma by increasing awareness and empathy.
In contrast the absence of training regarding certain health or social conditions can influence how care and services are delivered by professionals working in these fields, thereby contributing to discriminatory practices.Footnote 38 One salient example is the way insufficient training among health care providers on HIV transmission risk can lead to insensitive and discriminatory practices towards patients living with HIV.Footnote 43Footnote 55
Health care policies and practices
The domain of “health care policies and practices” refers to health system–level factors that pertain to the delivery of health care, including facility presence, accessibility and internal operational policies. Seventeen individual works referenced terms associated with this domain.Footnote 26Footnote 28Footnote 31Footnote 33Footnote 34Footnote 37Footnote 40Footnote 41Footnote 44Footnote 45Footnote 48Footnote 49Footnote 55Footnote 60Footnote 64Footnote 65Footnote 66 Of these, five proposed conceptual frameworks that referenced terms relating to this domain.Footnote 33Footnote 40Footnote 45Footnote 65Footnote 66 A non-exhaustive list of terms used included “health care system,”Footnote 33 “linkage to care,”Footnote 45 “healthcare quality”Footnote 66 and “institutional [health care] protocols.”Footnote 65
Overall, structural determinants relating to health care policies tended to fall under two categories: factors relating to the availability and relative accessibility of high-quality health care services, and factors pertaining to internal policies on health service organization and delivery. An example of the former is systemic differences in the availability of prompt,Footnote 28Footnote 65 high-quality health care across communities, according to region of residence,Footnote 40Footnote 66 financial capacity,Footnote 44 and linguistic or cultural background.Footnote 34 Examples of health care initiatives that may reduce stigma are programs that improve the accessibility of services, such as policies that help patients navigate health systems and adhere to treatment plans,Footnote 44 and outreach activities (e.g. home visits) for underserved populations.Footnote 40
Within clinical settings, institutional policies and structures can also contribute to discrimination against certain populations. Salient examples include physical structures, such as open-plan waiting rooms, and inter-staff communication policies that fail to protect patient’s confidentiality by allowing diagnoses to be overhead by others. These kinds of policies and structures can deter vulnerable populations from seeking care and can lead to the mistreatment of patients with stigmatized health conditions such as HIVFootnote 55 or TB.Footnote 48
Biomedical technology
The domain of “biomedical technology” refers to structural determinants that pertain to the development, existence, use and effects of technology or medical products that are provided to patients in clinical health settings to treat diagnosed health conditions. A sample of terms relating to this domain include “advent of effective treatment,”Footnote 48 “control of disease”Footnote 33 and “treatment side effects.”Footnote 54 Six works—including one conceptual frameworkFootnote 33—referenced determinants relating to this domain.Footnote 26Footnote 33Footnote 48Footnote 54Footnote 78Footnote 79
Overall, studies documented how the existence of biomedical technologies that can prevent, manage or treat health conditions such as HIV,Footnote 26 TB,Footnote 48 or cancer,Footnote 54 to name some examples, can influence the stigma process by changing the visibility of the condition, or by shifting societal beliefs around the dangerousness, severity and permanence of the disease as well as the risk of transmission. Studies also identified how the targeted promotion of biomedical treatments to certain populations because of their behaviours or risk profiles may lead to increased stigma. For example, guidelines that recommend that individuals engaging in riskier sexual activities use pre-exposure prophylaxis (PrEP) to prevent HIV infection may cause people to conflate the use of this technology with sexual promiscuity, resulting in potential and current users fearing and experiencing discrimination.Footnote 26
Diagnostic frameworks
The domain of “diagnostic frameworks” refers to structural determinants that pertain to developments in the understanding of disease etiology and classification. Seven works described determinants that relate to this domain,Footnote 33Footnote 35Footnote 46Footnote 50Footnote 58Footnote 63Footnote 79 two of whichFootnote 33Footnote 46 proposed a conceptual framework that referenced terms relating to this domain. Examples of terms falling under this domain included “diagnostic practices,”Footnote 63 “DSM” (Diagnostic and Statistical Manual of Mental Disorders),Footnote 79 “genetic causal information”Footnote 50 and “medicalization.”Footnote 58
Overall, developments in societal understanding of how diseases emerge can contribute to the stigma process by influencing societal perceptions of where responsibility for disease emergence should be placed. One example of this has been research findings that certain conditions such as mental health disorders or diabetes can be linked to underlying genetic factors. These developments in scientific knowledge can shift how societies attribute blame for incidence of these conditions.Footnote 33Footnote 50
Developments in societal understanding of how health and social conditions should be classified can contribute to the stigma process by influencing perceptions of what is considered abnormal. By labelling certain conditions as “disorders” or “diseases,” clinical diagnoses can imply the need for corrective treatment and facilitate the ostracizing of affected individuals. One illustrative example is how previous editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM) pathologized homosexuality and gender nonconformity, contributing to negative stereotypes of and discrimination against LGBTQ+ communities.Footnote 58
Public health interventions
The domain of “public health interventions” refers to policies, programs and initiatives led or mandated and financially supported by public health stakeholders. Seven works, including one conceptual framework,Footnote 50 described determinants relating to this domain.Footnote 42Footnote 49Footnote 50Footnote 60Footnote 63Footnote 67Footnote 77 Terms used in these studies included “health promotion initiatives,”Footnote 50 “public health initiatives”Footnote 63 and “community-based outreach interventions.”Footnote 42
Overall, studies described how public health interventions can influence the stigma process by shaping societal norms and beliefs both positively and negatively. For example, health promotion interventions that perpetuate messaging around the need to change certain individual behaviours (e.g. weight control, substance consumption) can have unintentional negative influences on societal beliefs by reinforcing narratives of blame and responsibility for individuals engaging in these behaviours or experiencing resulting health conditions.Footnote 26Footnote 50 One illustration of this was public health messaging of zero-tolerance of alcohol consumption during pregnancy. This messaging can perpetuate negative societal beliefs of pregnant individuals who drink or of mothers of children with fetal alcohol spectrum disorder, and can lead to hesitancy among pregnant individuals who do drink to consult health and social services.Footnote 63
Community-based public health interventions can also influence the discrimination and status loss components of the stigma process by intervening on resource distribution. One example of such interventions is community-based public health initiatives designed to improve access to health and harm reduction services for populations that may have less trust in medical establishments due to historical discrimination, such as individuals living with HIV or sex workers.Footnote 42Footnote 60 These types of interventions are believed to be protective against stigma as they promote respect and inclusivity, and represent sources of empowerment for vulnerable populations.Footnote 42
Conceptual framework
The ten domains of structural determinants are summarized in Figure 3. This figure is a simplified conceptual framework that depicts the structural determinant domains identified in the reviewed literature, and how they were described in relation to the stigma process as defined by Link and Phelan.Footnote 1 Three large arrows flow from the structural determinants to the stigma process. These arrows indicate how structural factors can influence the stigma process overall, and more precisely by shaping the psychosocial “drivers” of the stigma process, which include societal beliefs and stereotypes based in fear, normative judgment or blame as well as lived experiences of discrimination and status loss.Footnote 3Footnote 72
Figure 3. Conceptual framework of identified domains of structural determinants and their relationship with the stigma process
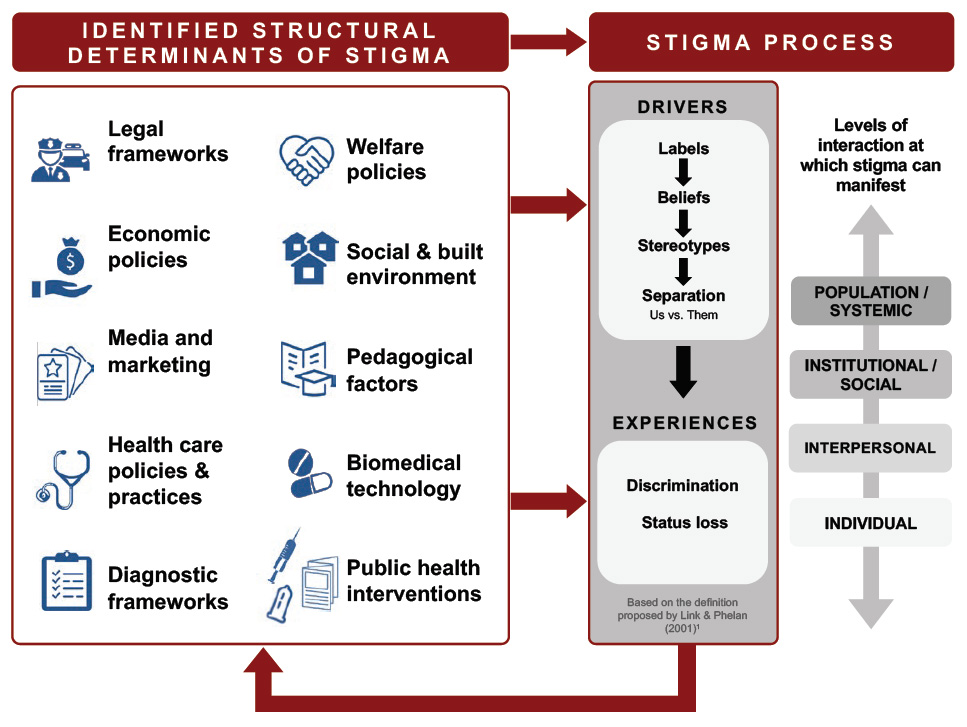
Note: This figure provides a visual summary of the narrative synthesis presented in this review. It should not be interpreted as providing a comprehensive summary of all possible structural determinant domains, nor as depicting firm causal ties between each of the domains and elements of the stigma process.
Text description: Figure 3
Figure 3. Conceptual framework of identified domains of structural determinants and their relationship with the stigma process
This figure demonstrates the conceptual framework of identified domains of structural determinants and their relationship with the stigma process. The 10 identified structural determinants of stigma are legal frameworks, economic policies, media and marketing, health car policies & practices, diagnostic frameworks, welfare policies, social & built environment, pedagogical factors, biomedical technology, and public health interventions. These determinants are linked to the stigma process at both its stages of drivers and experiences. Within the stigma process, it starts with drivers which are labels leading to beliefs leading to stereotypes leading to separation (us vs. them). From there drivers turn into experiences of discrimination and status loss. These experiences then manifest themselves on the structural determinants of stigma. Additionally, levels of interaction at which stigma can manifest include population/systemic, institutional/social, interpersonal, and individual.
In line with the reviewed conceptual frameworks and models, including the CPHO’s Stigma Pathways Model,Footnote 3 Figure 3 also includes a graphical representation of the levels of population interaction at which stigma can be enacted, from the individual (internalized) to the systems level. Further, many studies and existing frameworks acknowledged that stigma processes are influenced by historical social inequities and discrimination,Footnote 3Footnote 46Footnote 72 thus creating feedback loops between structural practices and stigma processes through time. To represent these dynamics, Figure 3 includes a large arrow that flows from the stigma process back to structural determinants.
Since this review did not involve an exhaustive literature search and further research is needed to confirm both the causal associations between factors and the effectiveness of various stigma-reduction interventions across populations and settings, Figure 3 should not be interpreted as providing a comprehensive summary of all possible structural determinant domains, nor as depicting firm causal ties between each of the domains and elements of the stigma process. Instead, it was designed to provide a visual summary of the narrative synthesis presented in this review that can be used as a tool to structure policy discussions on ways to orient public health interventions to reduce stigma in Canada and abroad.
Discussion
This rapid review was designed to identify and summarize structural determinants of stigma in Canada and other OECD settings, in order to guide future research and intervention. An analysis of findings from 53 works from peer-reviewed and grey-literature sources, 15 of which included proposed conceptual frameworks that mentioned at least one type of structural determinant of stigma, this review is the first known summary and conceptual framework of structural determinants of stigma across health and social conditions. Applying a thematic analysis of structural-level factors documented in the literature, we identified and defined 10 distinct domains of structural determinants of stigma. These domains were legal frameworks, welfare policies, economic policies, social and built environments, media and marketing, pedagogical factors, health care practices and policies, biomedical technology, diagnostic frameworks, and public health interventions.
This summary fills an important gap in the existing literature by bringing together findings from a wide range of fields of stigma research, and elucidating types of factors that operate at the contextual level to influence societal beliefs, negative stereotypes, discrimination or status loss across multiple social contexts and populations.Footnote 14 This review and the proposed conceptual framework are tools that can be used to structure future policy conversations; the ten domains of factors and the governance sectors to which they relate can be systematically considered when seeking to address and prevent stigma. As structural-level factors can contribute to social stratification and health inequities,Footnote 9 each identified domain merits attention.
Strengths and limitations
One strength of this rapid review is its focus on determinants of stigma across health outcomes and physical or social attributes. The resulting summary is therefore applicable to a wide range of substantive domains of public health and social policy. Another strength is its focus on structures that could theoretically be modified through intersectoral public health intervention, with potential population-level impacts on the stigma process.Footnote 9Footnote 15
Nonetheless, this review has certain limitations. Due to the non-exhaustive search strategy of the rapid review design, relevant studies—particularly individual qualitative or quantitative studies—may have been missed by our search strategy, and thus, certain examples of structural determinants may have been missed as well. However, given that the majority of published works included in this review are evidence summaries and frameworks of structural determinants, we expect that the contribution of missed studies is likely to be minimal.
Another limitation is that many of the works reviewed here did not include sufficient detail about the process by which their results were obtained and synthesized. The opacity of the data-generating process of these works calls into question the comprehensiveness of their findings. The resulting summary should therefore be used primarily as a conceptual guide rather than an exhaustive review. Including this element in future texts will be a necessary step for strengthening public health literature on stigma.
Finally, this review summarizes findings for the general context of OECD nations. We did not seek to explore structural determinants within a specific jurisdiction. Since the impacts of structural determinants on the stigma process may be heterogeneous across local contexts, future research and policy conversations on ways to address stigma should consider how local eco-social or political environments may influence the structural determinants of stigma or the effects of potential interventions on stigma reduction.
Conclusion
This review complements previously published summaries of the influence of stigma as a determinant of health. Here, the structural determinants of stigma as a social outcome occurring across health and social conditions were explored. A rapid review of existing evidence suggests that there are at least ten domains of structural determinants of stigma. The present review’s conceptual framework of these domains can be used as a tool to structure future policy conversation across sectors on ways to reduce stigma at a population level.
Acknowledgements
We would like to thank Lisa Glandon and the Information and Knowledge Management Division from the Health Canada Library, as well as Dr. Kimberly Gray, Michèle Boileau-Falardeau and Dr. Louis Turcotte for their contributions and feedback.
Conflicts of interest
The authors have no conflicts of interest to declare.
Authors’ contributions and statement
All authors contributed to the methodological design of the literature review. AB and BHMF conducted the literature review search and identified relevant works. All authors extracted data, analyzed identified works and drafted the article. AB and CBF revised the article.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.