
Evidence synthesis – Sleep timing and health indicators in children and adolescents: a systematic review

HPCDP Journal Home
Published by: The Public Health Agency of Canada
Date published: April 2022
ISSN: 2368-738X
Submit a manuscript
About HPCDP
Browse
Previous | Table of Contents | Next
Caroline Dutil, MScAuthor reference footnote 1Author reference footnote 2; Irina Podinic, BScAuthor reference footnote 1Author reference footnote 3; Christin M. Sadler, MScAuthor reference footnote 2; Bruno G. da Costa, PhDAuthor reference footnote 1; Ian Janssen, PhDAuthor reference footnote 4Author reference footnote 5; Amanda Ross-White, MLISAuthor reference footnote 6; Travis J. Saunders, PhDAuthor reference footnote 7; Jennifer R. Tomasone, PhDAuthor reference footnote 4; Jean-Philippe Chaput, PhDAuthor reference footnote 1Author reference footnote 2Author reference footnote 3
https://doi.org/10.24095/hpcdp.42.4.04
This article has been peer reviewed.
Author references
Correspondence
Jean-Philippe Chaput, Healthy Active Living and Obesity Research Group, Children’s Hospital of Eastern Ontario Research Institute, 401 Smyth Road, Ottawa, ON K1H 8L1; Tel: 613-737-7600 ext. 3683; Fax: 613-738-4800; Email: jpchaput@cheo.on.ca
Suggested citation
Dutil C, Podinic I, Sadler CM, da Costa BG, Janssen I, Ross-White A, Saunders TJ, Tomasone JR, Chaput JP. Sleep timing and health indicators in children and adolescents: a systematic review. Health Promot Chronic Dis Prev Can. 2022;42(4):150-69. https://doi.org/10.24095/hpcdp.42.4.04
Abstract
Introduction: To continue to inform sleep health guidelines and the development of evidence-based healthy sleep interventions for children and adolescents, it is important to better understand the associations between sleep timing (bedtime, wake-up time, midpoint of sleep) and various health indicators. The objective of this systematic review was to examine the associations between sleep timing and 9 health indicators in apparently healthy children and adolescents 5 to 18 years old.
Methods: Studies published in the 10 years preceding January 2021 were identified from searches in four electronic databases. This systematic review followed the guidelines prescribed in PRISMA 2020, the methodological quality and risk of bias were scored, and the summary of results used a best-evidence approach for accurate and reliable reporting.
Results: Forty-six observational studies from 21 countries with 208 992 unique participants were included. Sleep timing was assessed objectively using actigraphy in 24 studies and subjectively in 22 studies. The lack of studies in some of the health outcomes and heterogeneity in others necessitated using a narrative synthesis rather than a meta-analysis. Findings suggest that later sleep timing is associated with poorer emotional regulation, lower cognitive function/academic achievement, shorter sleep duration/poorer sleep quality, poorer eating behaviours, lower physical activity levels and more sedentary behaviours, but few studies demonstrated associations between sleep timing and adiposity, quality of life/well-being, accidents/injuries, and biomarkers of cardiometabolic risk. The quality of evidence was rated as “very low” across health outcomes using GRADE.
Conclusion: The available evidence, which relies on cross-sectional findings, suggests that earlier sleep timing is beneficial for the health of school-aged children and adolescents. Longitudinal studies and randomized controlled trials are needed to better advance this field of research. (PROSPERO registration no.: CRD42020173585)
Keywords: bedtime, wake-up time, midpoint of sleep, youth, public health, guideline
Highlights
- Later sleep timing is generally associated with poorer health outcomes in children and adolescents.
- Findings in this research area are based on observational studies.
- Longitudinal studies and randomized trials are needed to investigate the health effects of sleep timing and determine whether these effects are independent of sleep duration.
Introduction
To many people, getting a good night’s sleep is synonymous with sleeping a sufficient number of hours. There is no denying that sleep duration is an important component of physical and mental healthFootnote 1. Lack of sleep, often fuelled by a mismatch between the social and the internal clocks, has been associated with numerous adverse health outcomes in all agesFootnote 2Footnote 3Footnote 4.
Sleep experts agree that many characteristics of sleep, in addition to duration, are relevant for optimal health. The Canadian 24-Hour Movement Guidelines for Children and Youth were published in 2016 to provide clear public health guidelines for physical activity, recreational screen time and sleep for 5- to 17-year-oldsFootnote 5. Since then, in an effort to better inform the general population, many countries and organizations worldwide have adopted this holistic, streamlined approach and all-encompassing messaging for the movement behaviours across the full 24-hour periodFootnote 6. The sleep recommendations in the Canadian 24-Hour Movement Guidelines for Children and Youth include sleep duration targets and consistent bedtimes and wake-up times across the week to minimize sleep variabilityFootnote 2. While the guidelines emphasize more than one important sleep characteristic (i.e. duration, quality and consistency), they do not mention sleep timing.
Sleep timing refers to the time of day that sleep occurs; it is often measured using bedtime, wake-up time or midpoint of sleep. Much like sleep needs, sleep timing varies among people, and it can be affected by intrinsic and extrinsic factors such as genetics, age, health status, school/work schedule, lifestyle, travel across time zones and light exposure, resulting in bedtimes and wake-up times that differ from individual preferencesFootnote 7. A recent systematic review reported that later sleep timing in healthy adults was associated with overall poorer health outcomesFootnote 8. Whether sleep timing is also associated with health in the pediatric population has, to date, not been systematically examined, especially with the inclusion of multiple health indicators. The purpose of this systematic review was to examine the associations between sleep timing and various health indicators in apparently healthy children and adolescents to help inform public health sleep guidelines and the development of future evidence-based healthy sleep interventions in this population.
Methods
Protocol and registration
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement to reduce risk of bias, improve transparency and ensure a more complete reporting of the findingsFootnote 9. This systematic review was also registered with the International Prospective Register of Systematic Reviews (PROSPERO Registration No.: CRD42020173585).
Eligibility criteria
To identify the research question and facilitate the search strategy, we adopted the Participants, Interventions, Comparisons, Outcomes and Study design (PICOS) frameworkFootnote 10.
Population
Apparently healthy children and adolescents between 5 and 18 years old, including those with overweight/obesity, but excluding those with other diagnosed medical diseases/conditions. Studies with children younger than 5 years or older than 17.99 years were considered as long as the mean age of the sample was between 5 and 18 years.
To capture more generalizable findings, we excluded studies specifically targeting clinical populations with a diagnosed sleep disorder or other diagnosed medical disease/condition. Also excluded were studies that focussed exclusively on a subset of the general population of school-aged children and adolescents, such as orphans, teen pregnancy, inpatient or institutionalized settings, athletes or individuals with a cognitive or a physical disability. Studies with mixed populations, that is, with individuals who met and did not meet the eligibility criteria, were included if the results pertaining to the population of interest were reported separately.
Intervention/exposure
The intervention or exposure of interest was sleep timing, which refers to the time of day that sleep occurs. For experimental studies, the intervention needed to target sleep timing exclusively and not multiple health behaviours simultaneously. Sleep timing is generally reported as sleep onset/sleep offset, bedtime/wake-up time or midpoint of sleep. Studies using objective (e.g. polysomnography, actigraphy/accelerometry) or subjective (e.g. self-report) measures of sleep timing (or both) were eligible. Only studies that quantified sleep timing were included. For example, we excluded studies examining diurnal preference (e.g. morningness/eveningness), chronotype (e.g. morning lark vs. night owl) or sleep consistency (e.g. sleep variability, social jetlag, catch-up sleep). These studies on other sleep characteristics are outside the scope of the present systematic review.
Comparison/control
Different levels of sleep timing were used as the comparator. However, a comparator or control group was not required for inclusion.
Outcomes
We agreed on a total of 9 health outcomes that targeted a comprehensive range. Of these, we deemed that 5 were critical (primary outcomes) and 4 were important (secondary outcomes). The 5 critical health outcomes were adiposity; emotional regulation (e.g. anxiety, depressive symptoms, stress, mood, hyperactivity/impulsivity); cognitive function and academic achievement (e.g. learning, memory, attention, concentration, grades); quality of life and well-being; and accidents/injuries. The 4 important health outcomes were biomarkers of cardiometabolic risk (e.g. insulin sensitivity/resistance, glucose tolerance, blood pressure, triglycerides); sleep duration and quality; eating behaviour; and physical activity and sedentary behaviour.
Study designs
All published or in-press peer-reviewed, observational or experimental studies were eligible for inclusion. Longitudinal studies with any follow-up length were eligible, but sleep timing had to be measured at least once in children or adolescents aged between 5 and 18 years old. There were no sample size restrictions.
Information sources and search strategy
To ensure a balance of sensitivity and specificity, the search strategy was developed by a research librarian (ARW) with expertise in systematic review searching; the search strategy was reviewed by a second research librarian (MS). The following electronic bibliographic databases were searched for relevant sources: Ovid MEDLINE, Ovid EMBASE, Ovid PsycINFO and EBSCO Cumulative Index to Nursing & Allied Health Literature (CINAHL). The search terms included these keywords for the subject headings and for sleep measurement: (1) headings: “Sleep” AND “Sleep Timing OR Midpoint of Sleep OR Sleep Consistency OR Regular Sleep OR Sleep Variability OR Sleep Schedule OR Catch-up Sleep OR Sleep Routine” OR “Bedtime OR Waketime”; and (2) sleep measurement: “Polysomnography” AND “Accelerometer OR Accelerometry” AND “Actigraphy” AND “Sleep Report OR Sleep Questionnaire OR Sleep Diary OR Sleep Eval OR Sleep Log OR Sleep Journal.”
The results were limited to full-text articles published in the previous 10 years. The initial search, conducted in March 2020, was for studies published from 1 March 2010 to 4 March 2020, in humans (children and adolescents), in English or French. Excluded were case studies and grey literature (e.g. conference abstracts, book chapters and dissertations). We decided on this limited date range to better manage the scope and to focus on the most recent and relevant body of evidence. The publication language was limited to English and French for reasons of feasibility; a recent meta-epidemiological study reported that excluding non-English publications does not impact conclusionsFootnote 11. An updated search was performed in January 2021 for studies published between 4 March 2020 and 13 January 2021. Finally, the reference lists of the included studies were reviewed to verify that no articles may have been missed during the search. The full search strategy is available online.
Selection process
To remove duplicates, bibliographic records were imported into Reference Manager software (Thompson Reuters, San Francisco, CA, US). The individual bibliographical records were then imported into Covidence (Veritas Health Innovation, Melbourne, AU) for level 1 and level 2 screening. During level 1 screening, two reviewers (CD, CMS or BGC), working independently, screened the titles and abstracts of all the potentially relevant articles. Two reviewers (CD, CMS or J-PC), working independently, then reviewed all the full-text articles that passed the level 1 screening. Any discrepancies were resolved via discussion until the reviewers reached consensus. Agreement among the reviewers during the selection process was evaluated using Cohen’s κFootnote 12.
Microsoft Excel and Word (2007; Microsoft Corp., Redmond, WA, US) were used for data extraction. Data extraction was completed, in an unblinded manner, by one reviewer, and verified by another (CD, IP). Important features were extracted for each included article: authors’ names; publication year; country of study; study design; sample size; participants’ age range, mean age and school grade; exposure; comparator; outcome measurement; results; and covariates. When multiple models were reported on the same outcome measurement, results from the most fully adjusted model were extracted. We also reported on whether studies reported differences in effect by age, sex, race/ethnicity, socioeconomic status, weight status or sleep duration (when sleep duration was not the outcome of interest). See Figure 1 for the PRISMA 2020 flow diagramFootnote 9 for the identification and selection of studies.
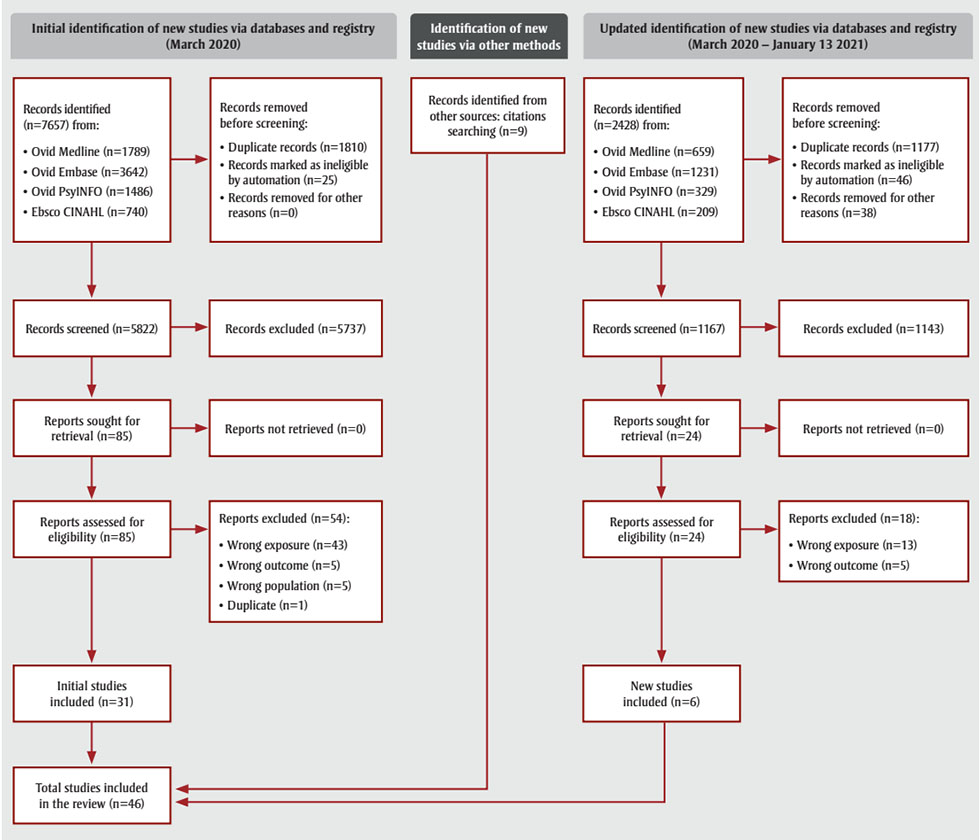
Figure 1 - Text description
This figure depicts the PRISMA flow diagram for selection of studies in this systematic review.
Studies were identified via databases and registry (March 2020), via other methods, and via databases and registry (March 2020 – January 13, 2021).
From the initial identification of new studies via databases and registry (March 2020), 7657 records were identified:
- Ovid Medline (n = 1789)
- Ovid Embase (n = 3642)
- Ovid PsyINFO (n = 1486)
- Ebsco CINAHL (n = 740)
Of these, the following records were removed before screening:
- Duplicate records (n = 1810)
- Records marked as ineligible by automation (n = 25)
- Records removed for other reasons (n = 0)
5822 records were therefore screened, of which 5737 were excluded. As a result, 85 reports were sought for retrieval (n = 0 reports not retrieved), and 85 reports were assessed for eligibility. Of those, 54 reports were excluded for the following reasons:
- Wrong exposure (n = 43)
- Wrong outcome (n = 5)
- Wrong population (n = 5)
- Duplicate (n = 1)
This resulted in n = 31 initial studies included.
From the studies identified via other methods, n = 9 records were identified from other sources through citations searching.
From the updated identification of new studies via databases and registry (March 2020 – January 13, 2021), 2428 records were identified from:
- Ovid Medline (n = 659)
- Ovid Embase (n = 1231)
- Ovid PsyINFO (n = 329)
- Ebsco CINAHL (n = 209)
Of these, the following records were removed before screening:
- Duplicate records (n = 1177)
- Records marked as ineligible by automation (n = 46)
- Records removed for other reasons (n = 38)
1167 records were therefore screened, of which 1141 were excluded. As a result, 24 reports were sought for retrieval (n = 0 reports not retrieved), and 24 reports were assessed for eligibility. Of those, 18 reports were excluded for the following reasons:
- Wrong exposure (n = 13)
- Wrong outcome (n = 5)
This resulted in n = 6 new studies included.
In the end, n = 46 total studies were included in the review.
Abbreviation: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Risk of bias and study quality assessment
The quality of primary research contributing to each health outcome was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) frameworkFootnote 13. In accordance with the Cochrane Handbook, the risk of bias assessment was completed for all included studies individually and by outcomeFootnote 14. GRADE groups the quality of evidence into four categories (“high,” “moderate,” “low” and “very low”); the rating begins at “high” for randomized studies and at “low” for all other studies, including nonrandomized experiments and all types of observational studies. The quality of evidence can be upgraded one level if there are no serious limitations and if there is a large magnitude of effect or evidence of a dose–response relationship. Conversely, the quality of evidence can be downgraded if there are serious limitations across studies (e.g. serious risk of bias, inconsistency of relative treatment effects, indirectness, imprecision, lack of evidence or other factors)Footnote 13. The quality of evidence assessment was conducted by two authors (CD and IP) and verified by the remainder of the review team, including a systematic review methodology expert (ARW). Disagreements were resolved by discussion among the team members.
Results
Description of studies
A total of 10 085 records were identified via the original and updated searches of the relevant electronic bibliographic databases (see Methods and Figure 1). After the removal of duplicates, a total of 6989 unique records remained for the level 1 title and abstract screening. The interrater reliability for the level 1 screening process was assessed for substantial agreement (κ > 0.70)Footnote 12.
Following level 1 screening, a total of 109 reports were sought for retrieval and assessed for eligibility. The level 2 eligibility review of the full-text articles excluded 72 articles, with 37 articles meeting the inclusion criteria. Out of the 72 articles excluded, 56 were excluded for having the wrong exposure, 10 for having the wrong outcome, 5 for having the wrong population and 1 for being a duplicate. The interrater reliability for the level 2 eligibility review of the full-text articles was assessed at near-perfect agreement (κ > 0.85)Footnote 12. See Supplementary Table 1 for the complete list of full-text articles excluded. Reviewing the reference lists of included studies generated an additional 9 studies.
Of the 46 observational studies included, 5 were longitudinal and 41 were cross-sectional. Data were collected in 21 countries and included 208 992 unique participants. Twenty studies were included for a single outcome, and 26 were included for two or more outcomes. Sleep timing was assessed objectively, using an actigraphy device, in 24 studies, and subjectively, using questionnaires, sleep diaries or interviews (by proxy or self-report), in 22 studies. Sleep timing was assessed as midpoint of sleep in 14 studies, bedtime in 20 studies and a combination of bedtime/wake-up time or sleep onset/offset in 4 studies. Multiple measurements of sleep timing were independently analyzed in 8 studies. Variation of the effect between sleep timing and health outcomes caused by factors such as age, sex, race/ethnicity, socioeconomic status, weight status and sleep duration (when sleep duration was not the outcome) was only reported in 3 studies, partially addressed (mainly age and/or sex) in 13 studies and not reported in 30 studies.
Because of the small number of studies reporting some outcomes and the heterogeneity across studies in other outcomes, meta-analyses were not possible and we structured narrative syntheses around each health indicator to convey the findings. Population subgroups were defined as children (5–12 years) and adolescents (13–18 years), when possible.
Data synthesis
The full data extraction and findings of the individual studies, sorted by outcome and study design, are reported in Supplementary Tables 2 and 3 for the critical and important health outcomes, respectively. The summarized findings for the individual studies, sorted by outcome and study design, are in Tables 1 and 2 for the critical and important outcomes, respectively. Quality of evidence assessment, sorted by outcome and study design, are in Table 3 for all outcomes. Finally, a high-level summary of findings is presented in Table 4 for all outcomes, sorted by outcome and study design. In Table 4, studies are classified as having mixed findings if (1) the association between sleep timing and the outcome was not consistent across measurements; (2) the measurements of sleep timing did not show consistent associations with the outcome; and (3) the association between sleep timing and the outcome showed variation based on sex, age or other factors.
| Study design and no. / No. of participants / age range | Measurement of sleep timing (no. of studies) | Findings |
|---|---|---|
| Adiposity | ||
| Longitudinal (n = 3) 7756 participants 4–18 years |
Objectively, using an actigraphy device (n=1) Subjectively, by self-report (n = 1) and proxy-report (n = 1) |
Hierarchical linear models revealed a significant longitudinal association between self-reported later bedtime and increased BMI z-score from adolescence to adulthood (β = 0.035, p < 0.05)Footnote 15. In children, adjusted linear regression analyses revealed that a higher total number of times that children were in proxy-reported late bedtime groups at data collection timepoints was significantly associated with higher BMI z-score (p < 0.001) and waist circumference (p = 0.03) at 8–9 yFootnote 16. No significant longitudinal associations were found between objectively measured sleep onset or midpoint of sleep and BMI z-scoreFootnote 17. |
| Cross-sectional (n = 17) 38 798 participants 5–18 years |
Objectively, using an actigraphy device (n = 10) Subjectively, by self-report (n = 5) and proxy-report (n = 2) | In a sample of children and adolescents, multivariable linear regression revealed that those in the late-sleep timing groups, established via self-report, had higher BMI z-score relative to those in the early-bed/early-rise group (late-bed/early-rise: β = 0.17, 95% CI: 0.00–0.35, p = 0.05; late-bed/late-rise: β = 0.20, 95% CI: 0.06–0.34, p = 0.007)Footnote 18. In a sample of adolescents, general linear modelling showed that objectively measured later corrected midpoint of sleep was significantly associated with greater waist-to-height ratio (β = 0.015, 95% CI: 0.003–0.028, p < 0.05); however, no significant association was found between corrected midpoint of sleep and BMIFootnote 19. In a sample who self-reported their sleep timing, multivariable logistic regressions revealed that the odds of overweight or obesity were 1.55 for the late-bed/early-rise group of children and 1.47 for the late-bed/late-rise group of adolescents, and the odds of obesity were 1.89 for the late-bed/early-rise group of children and 2.16 for the late-bed/late-rise group of adolescents, compared to participants in the early-bed/early-rise groupFootnote 20. In 5-year-old children, analysis of covariance revealed that proxy-reported earlier bedtime (before or at 20:00), was significantly associated with lower BMI z-score (p < 0.01), but no significant association was found between wake-up time and BMI z-scoreFootnote 21. In a sample of adolescents, multivariable logistic regression revealed that self-reported later weekend midpoint of sleep was significantly associated with higher BMI z-score in females only (<3:30: reference; 4:00 to 4:29: OR = 1.81; 95% CI: 0.90–3.63; 4:30 to 5:04: OR = 1.82; 95% CI: 0.96–3.47; ≥5:05: OR = 1.68; 95% CI: 0.85–3.33, p = 0.04). Weekday midpoint of sleep was not associated with BMI z-scoreFootnote 22. In children, proxy-reported late compared to normal midpoint of sleep over the whole week was significantly associated with higher fat mass percentage and waist circumference, but was not associated with BMI z-score or the sum of the skinfoldsFootnote 23. In a sample of children with obesity, multivariate linear regression analyses revealed that objectively measured later bedtime on weekdays was associated with greater percent overweight (β = 6.17, 95% CI: 1.42–10.92, p < 0.05), percent over 95th BMI percentile (β = 4.60, 95% CI: 1.07–8.13, p < 0.05), BMI (β = 1.03, 95% CI: 0.22–1.85, p < 0.05) and waist circumference (β = 2.06, 95% CI: 0.23–3.88, p < 0.05). Objectively measured later weekday wake-up time was also significantly associated with higher BMI (β = 0.85, 95% CI: 0.00061–1.70, p < 0.05) and waist circumference (β = 2.03, 95% CI: 0.13–3.93, p < 0.05). Neither objectively measured weekend bedtime nor weekend wake-up time was significantly associated with any of the adiposity outcomes. Of the proxy-reported sleep-timing measures, only later weekday bedtime was significantly associated with higher percent over 95th BMI percentile (β = 4.33, 95% CI: 0.038–8.63, p < 0.05) and BMI (β = 1.01, 95% CI: 0.021–2.00, p < 0.05)Footnote 24. 10 studies reported no significant associations between objectivelyFootnote 25Footnote 26Footnote 27Footnote 28Footnote 29Footnote 30Footnote 31Footnote 32 and subjectivelyFootnote 33Footnote 34 measured sleep timing and adiposity. |
| Emotional regulation | ||
| Longitudinal (n = 2) 6331 participants 4–18 years |
Subjectively, by self-report (n = 1) and proxy-report (n = 1) | In adolescents, self-reported later school-year bedtime at timepoint 1 (T1; Grades 7–12) and later summertime bedtime at timepoint 2 (T2; Grades 8–12) were associated with higher odds of emotional distress at timepoint 3, 6–8 y later in young adulthood (T1 school-year bedtime: OR = 1.35, 95% CI: 1.0–1.8, p < 0.05; T2 summertime bedtime: OR = 1.35, 95% CI: 1.1–1.8, p < 0.05)Footnote 35. In children, adjusted linear regression analyses revealed that a higher total number of times children were in proxy-reported late bedtime groups at data collection timepoints (from never to 3 times) was significantly associated with more parent-reported (p = 0.03) and teacher-reported (p = 0.05) behavioural problems at 8–9 yFootnote 16. |
| Cross-sectional (n = 7) 106 225 participants 7–20 years |
Objectively, using an actigraphy device (n = 2) Subjectively, by self-report (n = 5) | In children, logistic regression revealed that self-reported bedtime after 22:00, compared to bedtime before or at 21:00, was associated with an increased odds of self-reported depressive symptoms (≤21:00: reference; 22:00–23:00: OR = 1.89, 95% CI: 1.0–3.6, p < 0.05; >23:00: OR = 4.66, 95% CI: 2.1–10.2, p < 0.01)Footnote 36. In adolescents and young adults, adjusted Poisson regression modelling revealed that, compared to those with a self-reported bedtime at ~22:00 or earlier, those with bedtime at ~22:30 had better depression scores (β = −0.1, 95% CI: −0.2 to −0.1, p < 0.0001), while those with a bedtime at ~23:30 or later had worse depression scores (β = 0.5, 95% CI: 0.5–0.6, p < 0.0001). In addition, going to bed at ~23:30 or later, compared to ~22:00 or earlier, was associated with increased odds of having anxiety or nervousness during the last 6 months. Going to bed at ~22:30 or later, compared to ~22:00 or earlier, was associated with increased odds of being irritated and having tantrums during the last 6 monthsFootnote 37. In 17-year-olds, Tobit regression modelling revealed that objectively measured later midpoint of sleep was significantly associated with 2 out of 10 youth self-report scales: more thought problems (β = 0.9, 95% CI: 0.01–1.8, p < 0.05) and more rule-breaking behaviour (β = 1.5, 95% CI: 0.6–2.4, p < 0.001). Later midpoint of sleep was also significantly associated with 2 out of 6 Diagnostic and Statistical Manual of Mental Disorders-oriented scales: more affective problems (β = 1.2, 95% CI: 0.05–2.3, p < 0.05) and more conduct problems (β = 1.2, 95% CI: 0.2–2.1, p < 0.05)Footnote 38. In a sample of adolescents, self-reported later bedtime was significantly correlated with higher anxiety (r(256) = 0.16, p < 0.05) and depressed mood (r(383) = 0.20, p < 0.01)Footnote 39. In a sample of adolescents with overweight or obesity, objectively measured later bedtime on weekdays, but not weekends, was associated with increased self-report of behavioural problem symptoms (β = 0.52, p = 0.01)Footnote 40. In a sample of children and adolescents, self-reported later weekday and weekend bedtimes, but not wake-up times, were each correlated with higher subjective depression scores (r(499) = 0.130, p = 0.003 and r(499) = 0.088, p = 0.049, respectively)Footnote 41. In adolescents, self-reported earlier wake-up time was significantly correlated with low subjective academic stress (r(479) = 0.12, p < 0.01)Footnote 42. |
| Cognitive function and academic achievement | ||
| Longitudinal (n = 2) 6331 participants 4–18 years |
Subjectively, by self-report (n = 1) and proxy-report (n = 1) | Longitudinal associations revealed that self-reported later school-year bedtime at T1 (mean age 15.4 y) and T2 (mean age 16.4 y) was associated with lower high-school cumulative GPA (β = −0.27, 95% CI: −0.37 to 0.17, p < 0.001, and β = −0.13, 95% CI: −0.24 to 0.023, p < 0.01, respectively). Summertime bedtime was not associated with cumulative GPAFootnote 35. In children, no significant longitudinal associations were found between proxy-reported sleep-timing group and verbal cognition, non-verbal cognition, language literacy and mathematical thinkingFootnote 16. |
| Cross-sectional (n = 5) 123 372 participants 7–20 years |
Subjectively, by self-report (n = 4) and proxy-report (n = 1) | In a sample of adolescents, there was an increased odds of poor GPA in those who self-reported typical weekday bedtime before 22:00 (OR = 1.74, 95% CI: 1.31–2.33) and after 00:00 (00:00–00:59: OR = 1.6, 95% CI: 1.37–1.91; 01:00–01:59: OR = 2.19, 95% CI: 1.71–2.81; 2:00 or later: OR = 2.76, 95% CI: 1.93–3.94), relative to bedtime between 22:00 and 22:59Footnote 43. In a sample of adolescents and young adults, self-reported bedtime at approximately 22:30 or later, relative to 22:00 or earlier, was associated with increased odds of self-reported trouble with following class education, completing homework assignments, preparing for examinations, writing tasks and reading tasks. In addition, bedtime at approximately 23:00 or later, relative to 22:00 or earlier, was associated with increased odds of having trouble with reading tasksFootnote 37. In adolescents, hierarchical multiple regression analyses revealed that self-reported later bedtime (not waketime) was significantly associated with lower college entrance exam scores (β = 0.133, p < 0.01). No associations were found between bedtime or wake-up time and subjective academic performanceFootnote 42. 2 studies reported no significant associations between subjectively measured sleep timing and cognitive performance and academic achievement outcomesFootnote 41Footnote 44. |
| Quality of life and well-being | ||
| Longitudinal (n = 1) 3631 participants 4–9 years |
Subjectively, by proxy-report (n = 1) | In children, adjusted linear regression analyses revealed that a higher total number of times children were placed in proxy-reported late bedtime groups at data collection timepoints (from never to 3 times) was significantly associated with poorer proxy-reported psychosocial (p = 0.001) and physical health (p = 0.002) functioning at 8–9 yFootnote 16. |
| Cross-sectional (n = 1) 6266 participants 9–11 years |
Objectively, using an actigraphy device (n = 1) | In an international sample of children, no overall associations were found between objectively measured weekday or weekend midpoint of sleep and health-related quality of life scoreFootnote 45. |
| Accidents/injuries | ||
| Cross-sectional (n = 1) 103 859 participants 14–20 years |
Subjectively, by self-report (n = 1) | In adolescents and young adults, logistic regressions revealed that, relative to those with self-reported bedtime at ~22:00 or earlier, the odds of reporting accidents requiring medical attention during recess and in other classes were lower among those with bedtime at ~23:00. A greater decrease in odds of having accidents on the way to school was observed in those with bedtime at ~23:00, than in those with bedtime at ~22:30, relative to those with bedtime at ~22:00 or earlier. There was no association found between bedtime and accidents requiring medical attention during gym classFootnote 37. |
Abbreviations: BMI, body mass index; CI, confidence interval; GPA, grade point average; no., number; y, years. |
||
| Study design and no. / No. of participants / age range | Measurement of sleep timing (no. of studies) | Findings |
|---|---|---|
| Biomarkers of cardiometabolic risk | ||
| Cross-sectional (n = 7) 3089 participants 8–19 years |
Objectively, using an actigraphy device (n = 6) Subjectively, by self-report (n = 1) |
In children and adolescents, adjusted linear regression analyses indicated that objectively measured later midpoint of sleep on weekends (β = 0.049, 95% CI: 0.004–0.093, p = 0.03), but not on weekdays (β = 0.041, 95% CI: 0.005–0.087, p = 0.08), was associated with higher insulin resistance, estimated using the Homeostatic Model Assessment of Insulin Resistance. In girls, each hour increase in weekday and weekend midpoint of sleep represented a significant increase in insulin resistance (β = 0.091, 95% CI: 0.027–0.16, p = 0.006, and β = 0.08, 95% CI: 0.017–0.14, p = 0.01, respectively)Footnote 46. In children, after adjusting for covariates, analyses of covariance revealed that, on average, participants with objectively measured bedtime before 22:30 had significantly better triglyceride/high-density lipoprotein cholesterol ratio (p = 0.026) than participants with bedtime later than 23:15. There was no significant association between bedtime category and blood insulin level or mean arterial pressureFootnote 27. In children, simple linear regression revealed that later midpoint of sleep was significantly associated with lower diastolic blood pressure (β = −0.002, p = 0.04); no significant associations were found between midpoint of sleep and systolic blood pressure, apolipoprotein B/A1 or glycoprotein acetylsFootnote 28. In children and adolescents, adjusted multiple linear regression analyses revealed that objectively measured later bedtimes (total, during the week and on the weekend) were significantly associated with higher systolic blood pressure z-score (total: β = 0.22, p = 0.02; weekday: β = 0.21, p = 0.02; weekend: β = 0.23, p = 0.02). No associations were found between bedtime and insulin resistance, triglycerides z-score, high-density lipoprotein-C z-score, low-density lipoprotein-C or diastolic blood pressure z-scoreFootnote 29. In a sample of adolescents with overweight or obesity, simple linear regression analyses showed that objectively measured earlier weekday bedtime was significantly associated with better fasting insulin resistance (p = 0.04) but was not associated with the Matsuda Index (p = 0.23)Footnote 47. 2 studies reported no significant associations between objectivelyFootnote 30 and subjectivelyFootnote 33 measured sleep timing and cardiometabolic risk factors including blood pressure, fasting serum levels of glucose and insulin, and dyslipidemia. |
| Sleep duration and quality | ||
| Longitudinal (n = 1) 783 participants 6–10 years |
Objectively, using an actigraphy device (n = 1) | In children, no significant longitudinal associations were found between objectively measured sleep onset or midpoint of sleep and sleep durationFootnote 17. |
| Cross-sectional (n = 10) 112 043 participants 5–20 years |
Objectively, using an actigraphy device (n = 3) Subjectively, by self-report (n = 6) and proxy-report (n = 1) |
In a sample of children and adolescents, self-reported earlier midpoint of sleep on both school and weekend nights was correlated with better self-reported sleep quality (r = 0.16, p = 0.03 and r = 0.26, p = 0.002, respectively). No significant association was found between midpoint of sleep on both school and weekend nights and subjectively measured sleep durationFootnote 48. In children, objectively measured later sleep onset and earlier sleep offset were significantly correlated with decreased total sleep time (r(1229) = −0.60 and r(1229) = 0.16, respectively)Footnote 25. In adolescents and young adults, adjusted Poisson regression modelling revealed that bedtime at ~22:30 or later, compared to ~22:00 or earlier, was associated with more sleep quality problems (~22:30: β = 0.04, 95% CI: 0.02–0.05, p < 0.0001; ~23:00: β = 0.08, 95% CI: 0.07–0.09, p < 0.0001; ≥23:30: β = 0.2, 95% CI: 0.2–0.2, p < 0.0001) and with an increased odds of having trouble falling asleep during the last 6 monthsFootnote 37. In children and adolescents, self-reported later bedtime was associated with decreased self-reported sleep durationFootnote 20. In a sample of adolescents, self-reported later bedtime was found to be significantly correlated with lower self-reported total sleep time and with greater report of unrefreshing sleep, r(306) = −0.50, p < 0.001 and r(306) = 0.22, p < 0.001, respectivelyFootnote 49. In children, a significant correlation was found between objectively measured later bedtime and shorter total sleep time (r = −0.61, p < 0.001)Footnote 31. Children in the proxy-reported late midpoint-of-sleep group had significantly less total sleep duration, by approximately 15 min during weekdays and during the whole week, compared to children in the normal midpoint-of-sleep group (p < 0.01)Footnote 23. In a sample of children, fractional multinomial logit models revealed significant associations between objectively measured later bedtime (30 min above the mean compared to 30 min below the mean) and less total sleep time by 35.6 min/night at age 5 and by 39.0 min/night at age 7 (p < 0.05)Footnote 50. 2 studies reported no significant associations between subjectively measured sleep timing and sleep durationFootnote 15Footnote 51. |
| Eating behaviours | ||
| Cross-sectional (n = 13) 42 138 participants 5–18 years |
Objectively, using an actigraphy device (n = 7) Subjectively, by self-report (n = 5) and proxy-report (n = 1) |
In a sample of children and adolescents, self-reported later weeknight bedtime was associated with an increased odds of reporting missing breakfast (9–11 years: OR = 4.5, 95% CI: 3.3–6.0; 12–14 years: OR = 4.7, 95% CI: 4.1–5.4; 15–17 years: OR = 4.1, 95% CI: 2.3–7.5) and consuming junk food ≥5 times in a week (9–11 years: OR = 2.7, 95% CI: 2.0–3.5; 12–14 years: OR = 2.9, 95% CI: 2.6–3.3; 15–17 years: OR = 2.1, 95% CI: 1.4–3.3)Footnote 52. In a sample of children, objectively measured later bedtime and sleep onset time were both significantly associated with higher self-reported restrained eating score (β = 0.40, p < 0.05 and β = 0.41, p < 0.05, respectively). No significant associations were found between sleep timing and emotional or external eating behavioursFootnote 53. In an international sample of children, objectively measured later bedtime was associated with less healthy diet pattern (β = −0.07, 95% CI: −0.11 to −0.02, p < 0.01) and more unhealthy diet pattern (β = 0.08, 95% CI: 0.04–0.13, p < 0.001)Footnote 54. In an international sample of children, objectively measured later bedtime was associated with greater frequency of cola and soft drink consumption per week (p < 0.01), while earlier bedtime was associated with higher frequency of energy drink and sports drink consumption (for both, p < 0.01)Footnote 55. In a sample of children and adolescents, multivariable linear regression revealed that, compared to those in the early-bed/early-rise self-reported sleep-timing group, those in the two late-bed groups had significantly lower total Dietary Guideline Index for Children and Adolescents scores (late-bed/early-rise: β = −3.09, 95% CI: −5.32 to −0.86, p = 0.007; late-bed/late-rise: β = −3.99, 95% CI: −5.66 to −2.32, p < 0.001). No significant association was found between sleep-timing group and energy intakeFootnote 18. In a sample of children, those in late-sleep groups had significantly lower fruits and vegetables dietary pattern scores (late-sleep/early-wake: mean = −0.1; late-sleep/late-wake: mean = −0.06; p < 0.05) than those in the early-sleep/early-wake group (mean = 0.19). Children in the late-sleep/late-wake group, compared to the early-sleep/early-wake group, also reported significantly lower weekly frequency of consumption of fruits and vegetables (mean = 16 vs. mean = 19, mean difference [95% CI]: −2.9 [−4.9 to −0.9], p < 0.05) and higher weekly frequency of consumption of sugar-sweetened beverages (mean = 7 vs. mean = 5, mean difference [95% CI]: 1.8 [0.2 to 3.3], p < 0.05), after adjusting for covariates. No significant associations were found between sleep-timing group and snack patterns or extra consumptionFootnote 26. In children, adjusted linear regression models revealed that objectively measured later bedtime was associated with greater fat (β = 0.02, p < 0.02) and lower carbohydrate (β = −0.02, p < 0.05) intake daily. No association was found between bedtime and daily caloric intake or daily protein intake. Later bedtime was associated with greater after-dinner caloric intake (β = 0.81, p < 0.01) in the form of protein (β = 0.08, p < 0.04) and fat (β = 0.37, p < 0.02), but not carbohydrate. Later bedtime was also associated with later timing of the last (β = 0.57, p < 0.001) and first (β = 0.76, p < 0.001) meals of the dayFootnote 31. Among children and adolescents who self-reported their midpoint of sleep, those in the late (vs. early) midpoint-of-sleep group had a significantly higher probability of consuming sweet and caffeinated beverages and sugary, salty and fatty foods, starting in the afternoon and for the rest of the day. No association was found between sleep-timing group and the probability of consumption of vegetables, proteins, fruits and carbohydrates. Those in the early (vs. late) midpoint-of-sleep group were more likely to report not skipping breakfast (96% vs. 30%, respectively, X2 [2, N = 55] = 26.7, p < 0.01). No other associations were found between sleep-timing group and the two other mealsFootnote 51. In children, analyses of variance revealed that being in the proxy-reported late midpoint-of-sleep group on weekdays (p < 0.05) and weekend days (p < 0.01) was associated with an increased cumulative number of self-reported eating risk factorsFootnote 23. 4 studies reported no significant associations between objectivelyFootnote 24Footnote 29 and subjectivelyFootnote 15Footnote 56 measured sleep timing and eating behaviours. |
| Physical activity and sedentary behaviours | ||
| Longitudinal (n = 1) 1059 participants 7–12 years |
Objectively, using an actigraphy device (n=1) | In children, fixed effect models revealed that an incremental increase by 30 min in objectively measured sleep onset was significantly associated with less time spent in LPA, moderate physical activity, MVPA and VPA (by 12, 3.5, 6.2 and 0.4 min, respectively) and more sedentary time (by 31 min) (all p < 0.001)Footnote 57. |
| Cross-sectional (n = 15) 14 642 participants 5–18 years |
Objectively, using an actigraphy device (n=10) Subjectively, by self-report (n=4) and proxy-report (n=1) |
In a sample of children and adolescents with obesity, after adjusting for covariates, linear regression revealed a significant association between later midpoint of sleep and daily amount of screen time (β = 105.7, 95% CI: 36.4–175.1, p < 0.01). However, no significant associations were found between sleep timing and time spent in MVPA or sedentary timeFootnote 56. In children and adolescents, self-reported later midpoint of sleep on school days was significantly associated with higher total time spent watching TV, using a tablet, using a smartphone and watching TV at night (all p < 0.04) as well as lower smartphone use during the day (p = 0.001). No association was found between midpoint of sleep on school days and 4 of the screen-time use outcomes. In addition, later weekend midpoint of sleep was significantly associated with higher total time spent watching TV, using a smartphone, watching TV at night, using a cell phone at night (all p < 0.02) and lower tablet and smartphone use during the day (both p < 0.05). Weekend midpoint of sleep was not associated with 3 of the screen-time use outcomesFootnote 48. In an international sample of children, adjusted analyses revealed that objectively measured later bedtime was associated with less time spent in MVPA (β = −1.08, 95% CI: −1.13 to −1.03, p < 0.0001), more time spent in sedentary behaviour (β = 0.36, 95% CI: 0.31–0.41, p < 0.0001) and higher screen-time score (β = 1.19, 95% CI: 1.14–1.25, p < 0.0001)Footnote 54. In a sample of children, those in both objectively measured late-wake sleep-timing groups were significantly less active (early-sleep/late-wake: mean = 72 min/day; late-sleep/late-wake: mean = 70 min/day) than those in the early-sleep/early-wake group (mean = 81 min/day). In addition, children in the late-sleep/late-wake group were significantly less active than those in the late-sleep/early-wake group (late-sleep/late-wake: mean = 70 min/day; late-sleep/early-wake: mean = 79 min/day). No significant association was found between objectively measured sleep timing and meeting screen-time guidelinesFootnote 26. In children, fixed interindividual analysis revealed that objectively measured later sleep onset was associated with less objectively measured time spent in MVPA per hour (β = –0.012, p = 0.001), independent of total sleep timeFootnote 58. In children, adjusted linear regression models revealed significant associations between objectively measured later midpoint of sleep (β = –0.11, p < 0.05), earlier bedtime (β = 0.10, p < 0.05) and later wake-up time (β = −0.13, p < 0.05) and less time spent in LPA. Also, later midpoint of sleep (β = 0.08, p < 0.05) and later wake-up time (β = 0.10, p < 0.05), but not bedtime, were significantly associated with more time spent being sedentary. No significant associations were found between sleep-timing variables and VPA, MVPA and moderate PAFootnote 32. In children at timepoint 1 (mean age 12.3 y), objectively measured later midpoint of sleep was significantly associated with lower PA (r(165) = −0.10, p = 0.03), LPA (r(165) = −0.10, p = 0.04), MVPA (r(165) = −0.10, p = 0.04) and higher sedentary behaviour (r(165) = 0.12, p = 0.02). At timepoint 2 (mean age 16.9 y), no significant associations were found between sleep timing and PA or sedentary behaviourFootnote 59. In children and adolescents who self-reported their sleep timing, the late-bed groups (vs. the early-bed/early-rise group) had the highest odds of lower PA and higher sedentary behaviour. No significant differences in odds of outcome were found between the two early-bed groups on each outcome studied. Compared to participants in the early-bed/early-rise group, the odds of low MVPA were 1.77 for the late-bed/late-rise group and 1.58 for the late-bed/early-rise group; the odds of high amounts of screen time were 2.92 for the late-bed/late-rise group and 1.94 for the late-bed/early-rise group; and the odds of both high amounts of screen time and low MVPA were 2.87 for the late-bed/late-rise group and 2.10 for the late-bed/early-rise group. In addition, on average, the early-rise groups engaged in significantly more minutes of MVPA, VPA, play and active transport per day and had higher daily pedometer step counts than the late-rise groups. The late-bed groups engaged in significantly more minutes of total sedentary time, screen time, watching television, playing videogames and computer timeFootnote 20. In children, fractional multinomial logit models at age 5 y revealed significant associations between later bedtime (30 min above the mean vs. 30 min below the mean) and more sedentary time and LPA time (10.1 and 21.6 min/day, respectively), but not with MVPA. At age 7 y, there were significant associations between later bedtime (30 min above the mean vs. 30 min below the mean) and more sedentary, LPA and MVPA time (14.7, 23.2 and 5.3 min/day, respectively)Footnote 50. In children, objectively measured later weekday bedtime was associated with self-reported screen time that was longer by an average of 3.19 (1.42) h/week (p < 0.05). No significant associations were found between objectively or subjectively measured bedtime or wake-up time and time spent in MVPAFootnote 24. 5 studies reported no significant associations between objectivelyFootnote 25Footnote 31Footnote 60 and subjectivelyFootnote 15Footnote 23 measured sleep timing. |
Abbreviations: LPA, light physical activity; MVPA, moderate-to-vigorous physical activity; PA, physical activity; no., number; VPA, vigorous physical activity; y, years. |
||
| Health outcome | Study design | No. of studies | No. of participants | Quality assessment indicator | Quality (GRADE)Footnote b |
||||
|---|---|---|---|---|---|---|---|---|---|
| Risk of bias | Inconsistency | Indirectness | Imprecision | OtherFootnote a | |||||
| Critical health outcomes | |||||||||
| Adiposity | Longitudinal | 3 | 7756 | Serious riskFootnote c | No serious risk | No serious risk | No serious risk | None | Very low |
| Cross-sectional | 17 | 38 798 | No serious risk | Serious riskFootnote d | No serious risk | No serious risk | None | Very low | |
| Emotional regulation | Longitudinal | 2 | 6331 | Serious riskFootnote c | No serious risk | No serious risk | No serious risk | None | Very low |
| Cross-sectional | 7 | 106 225 | Serious riskFootnote c | No serious risk | No serious risk | No serious risk | None | Very low | |
| Cognitive function and academic performance | Longitudinal | 2 | 6331 | Serious riskFootnote c | Serious riskFootnote c | No serious risk | No serious risk | None | Very low |
| Cross-sectional | 5 | 123 372 | Serious riskFootnote c | No serious risk | No serious risk | No serious risk | None | Very low | |
| Quality of life and well-being | Longitudinal | 1 | 3631 | No serious risk | Only one study | No serious risk | Serious riskFootnote e | None | Very low |
| Cross-sectional | 1 | 6266 | No serious risk | Only one study | No serious risk | Serious riskFootnote e | None | Very low | |
| Accidents/injuries | Cross-sectional | 1 | 103 859 | Serious riskFootnote c | Only one study | No serious risk | Serious riskFootnote e | None | Very low |
| Important health outcomes | |||||||||
| Biomarkers of cardiometabolic risk | Cross-sectional | 7 | 3089 | No serious risk | Serious riskFootnote c | No serious risk | No serious risk | None | Very low |
| Sleep duration and quality | Longitudinal | 1 | 783 | No serious risk | Only one study | No serious risk | Serious riskFootnote e | None | Very low |
| Cross-sectional | 10 | 112 043 | Serious riskFootnote c | No serious risk | No serious risk | No serious risk | None | Very low | |
| Eating behaviour | Cross-sectional | 13 | 42 138 | Serious riskFootnote c | No serious risk | No serious risk | No serious risk | None | Very low |
| Physical activity and sedentary behaviour | Longitudinal | 1 | 1059 | No serious risk | Only one study | No serious risk | Serious riskFootnote e | None | Very low |
| Cross-sectional | 15 | 14 642 | Serious riskFootnote c | No serious risk | No serious risk | No serious risk | None | Very low | |
Abbreviations: GRADE, Grading of Recommendations Assessment, Development and Evaluation; no., number.
|
|||||||||
| Health outcome | No. and type of studies / No. of participants / age range | Summary of findings |
|---|---|---|
| Critical health outcome | ||
| Adiposity | 3 longitudinal 7756 4–18 years |
1 study reported a longitudinal association between later bedtime during adolescence and higher BMI z-score later in adolescence and adulthood |
| 1 study reported a longitudinal association between reoccurring late bedtime over multiple timepoints and higher BMI z-score and waist circumference in children | ||
| 1 longitudinal study reported null findings | ||
| 17 cross-sectional 38 798 5–18 years |
1 study reported that children and adolescents in the late-to-bed groups had higher BMI z-score than those in the early-bed/early-rise group | |
| 1 study found that children and adolescents in the late-to-bed groups had greater odds of overweight and obesity than those in the early-to-bed/early-to-rise group | ||
| 1 study with mixed findings reported an association between later midpoint of sleep and greater waist-to-height ratio, but not BMI, in adolescents | ||
| 1 study with mixed findings reported an association between later bedtime, but not wake-up time, and higher BMI z-scores in 5-year-old children | ||
| 1 study with mixed findings reported an association between later weekend midpoint of sleep, but not weekday midpoint of sleep, and increased odds of higher BMI z-score in female (but not male) children and adolescents | ||
| 1 study with mixed findings reported that children in the late-sleep group had higher fat mass percentage and waist circumference but not higher BMI z-scores or the sum of the skinfolds | ||
| 1 study with mixed findings reported an association between later weekday, not weekend, bedtime and greater adiposity in children with obesity | ||
| 10 studies reported null findings | ||
| Emotional regulation | 2 longitudinal 6331 4–18 years |
1 study reported a longitudinal association between reoccurring late bedtime over multiple timepoints and higher behavioural problems in children |
| 1 study with mixed findings reported a longitudinal association, between both late school-year and summertime bedtime, but not at all time points, and higher odds of emotional distress 6–8 years later in late adolescence or early adulthood | ||
| 7 cross-sectional 106 225 7–20 years |
1 study in children reported an association between bedtime after 22:00 and increased odds of higher depressive symptoms | |
| 1 study in adolescents reported that, compared to a bedtime at ~22:00 or earlier, bedtime between ~22:30 and before 23:00 is associated with better depression score, while bedtime at ~23:00 or later is associated with worse depression scores, greater odds of having anxiety or nervousness, and greater odds of being irritated and having tantrums | ||
| 1 study in adolescents reported an association between later bedtime and higher depressed mood and anxiety scores | ||
| 1 study in adolescents with obesity reported an association between later bedtime and higher behavioural problems score | ||
| 1 study in adolescents reported an association between later wake-up time and greater academic stress | ||
| 1 study with mixed findings reported an association between later bedtime, but not wake-up time, and increased depression score in children and adolescents | ||
| 1 study with mixed findings reported an association between later midpoint of sleep and psychiatric problems, including more thought problems, more rule-breaking behaviour, more affective problems and more conduct problems, but not with a majority of the scales, in adolescents | ||
| Cognitive function and academic performance | 2 longitudinal 6331 4–18 years |
1 study with mixed findings reported a longitudinal association between later school-year bedtime, but not summertime bedtime, and lower grades in adolescents |
| 1 longitudinal study reported null findings | ||
| 5 cross-sectional 123 372 7–20 years |
1 study in adolescents reported an association between bedtimes before 22:00 or after 00:00 with increased odds of lower grades relative to bedtime between 22:00 and 22:59 | |
| 1 study in adolescents reported an association between bedtime at ~22:30 or later and increased odds of trouble with following class education, completing homework assignments, preparing for examinations, and writing tasks, while bedtime at ~23:00 or later is also associated with increased odds of having trouble with reading tasks | ||
| 1 study with mixed findings reported a significant association between later bedtime, but not waketime, and lower college entrance exam scores, in adolescents | ||
| 2 studies reported null findings | ||
| Quality of life and well-being | 1 longitudinal 3631 4–9 years |
1 study reported a longitudinal association between reoccurring late bedtime over multiple timepoints and poorer psychosocial and physical health functioning in children |
| 1 cross-sectional 6266 9–11 years |
1 study reported null findings | |
| Accidents / injuries | 1 cross-sectional 103 859 14–20 years |
1 study with mixed findings reported associations between bedtime at ~23:00 (relative to bedtime at ~22:00 or earlier) and lower odds of having an accident at recess, in the classroom, and on the way to school in adolescents. No association was found between bedtime and accidents during gym class |
| Important health outcome | ||
| Biomarkers of cardiometabolic risk | 7 cross-sectional 3089 8–19 years |
1 study with mixed findings reported that, in children and adolescent boys and girls, later midpoint of sleep on weekends, but not on weekdays, is associated with higher insulin resistance. In girls, each hour increase in weekday and weekend midpoint of sleep represented a significant increase in insulin resistance |
| 1 study with mixed findings reported that, in children, a bedtime before 22:30 is associated with better triglyceride/high-density lipoprotein cholesterol ratio compared to a bedtime later than 23:15. No significant association was found between bedtime category and blood insulin level nor mean arterial pressure | ||
| 1 study with mixed findings reported that, in children, later midpoint of sleep is associated with lower diastolic blood pressure, but no significant associations were found between midpoint of sleep and systolic blood pressure, apolipoprotein B/A1 or glycoprotein acetyls | ||
| 1 study with mixed findings reported that, in children and adolescents, later bedtime is associated with higher systolic blood pressure z-score, but that there were no associations between bedtime and insulin resistance, triglycerides z-score, high-density lipoprotein-C z-score, low-density lipoprotein-C or diastolic blood pressure z-score | ||
| 1 study with mixed findings reported a significant association between an earlier bedtime and better fasting insulin resistance but not with the Matsuda Index in adolescents with overweight or obesity | ||
| 2 studies reported null findings | ||
| Sleep duration and quality | 1 longitudinal 783 6–10 years |
1 longitudinal study reported null findings |
| 10 cross-sectional 112 043 5–20 years |
1 study in children reported an association between earlier sleep onset and later offset with longer total sleep time 1 study in adolescents reported an association between a bedtime at ~22:30 or later and lower sleep quality, relative to a bedtime at ~22:00 or earlier 1 study in children and adolescents reported an association between later bedtime and lower sleep duration 2 studies in children reported a significant association between later bedtime and less total sleep time 1 study in adolescents reported significant associations between later bedtime and less total sleep time and more reports of unrefreshing sleep 1 study in children reported an association between later midpoint of sleep and less total sleep duration 1 study with mixed findings reported associations between earlier midpoint of sleep during both school and weekend nights and better sleep quality, but not sleep duration, in children and adolescents 2 studies reported null findings |
|
| Eating behaviour | 13 cross-sectional 42 138 5–18 years |
1 study in children and adolescents reported an association between later weeknight bedtime with increased odds of missing breakfast and of frequent junk food consumption 1 study in children reported associations between later bedtime and less healthy and more unhealthy diet patterns 1 study in children reported associations between later midpoint of sleep on weekdays and weekend and an increased cumulative number of self-reported eating risk factors 1 study with mixed findings reported associations between later bedtime and sleep onset and higher restrained eating score, but no other significant associations between sleep timing and all other eating behaviours, in children 1 study with mixed findings reported associations between later bedtime and greater frequency of cola and soft drinks consumption, and between earlier bedtime and greater frequency of energy and sports drink consumption, in children 1 study with mixed findings reported associations between children in the late-sleep/late-wake group, compared to children in the early-sleep/early-wake group, and lower fruits and vegetables dietary score, lower weekly frequency of consumption of fruits and vegetables and higher weekly frequency of consumption of sugar-sweetened beverages, but the sleep-timing groups were not associated with snacking patterns or extra consumption 1 study with mixed findings reported associations between the 2 late-to-bed groups, compared to the early-to-bed/early-to-wake group, and lower total dietary score but not energy intake, in children and adolescents 1 study with mixed findings reported associations between later bedtime and higher daily fat intake, lower daily carbohydrate intake, greater caloric intake after dinner and later timing of breakfast and dinner, but no associations with daily total caloric intake or protein intake, in children 1 study with mixed findings reported associations between later midpoint of sleep and higher sustained probability of consuming sweet and caffeinated beverages and sugary, salty and fatty foods, from the afternoon onwards, but no associations with the probability of consuming vegetables, proteins, fruits or carbohydrates, in children and adolescents 4 studies reported null findings |
| PA and sedentary behaviour | 1 longitudinal 1059 7–12 years |
1 study in children reported a longitudinal association between an incremental increase in sleep onset and less time spent in PA at all intensities and more time spent in sedentary behaviour the following day |
| 15 cross-sectional 14 642 5–18 years |
1 study in children reported that later bedtime is associated with less time spent in MVPA and more time spent being sedentary and having more screen time 1 study in children reported that, at 5 years old, later bedtime is associated with more sedentary time and more LPA, but at 7 years old, it is also associated with more MVPA 1 study in children and adolescents reported numerous associations between later midpoint of sleep and more screen time across most devices on both week and weekend days 1 study in children reported an association between later sleep onset and less MVPA 1 study in children and adolescents reported associations between the late-to-bed sleep groups, compared to the early-to-bed/early-to-wake group, and lower odds of PA and higher odds of sedentary behaviours 1 study with mixed findings reported an association between later midpoint of sleep and more screen time, but not with time spent in MVPA or sedentary time, in children and adolescents with obesity 1 study with mixed findings reported associations between children in the late-to-wake sleep groups, compared to children in the early-to-bed/early-to-wake group, and less time spent being active but not with meeting the screen-time guidelines 1 study with mixed findings reported associations between later midpoint of sleep at 12 years old and lower amounts of PA overall, of LPA and of MVPA and more sedentary behaviour, but no associations were found at 17 years old 1 study with mixed findings reported associations between children’s later midpoint of sleep, earlier bedtime and later wake-up time and less time spent in LPA, but not with higher intensities of PA. Later midpoint of sleep and later wake-up time, but not bedtime, are also associated with more time spent being sedentary 1 study with mixed findings reported an association between later weekday bedtime, but not wake-up time, with more screen time, but not with MVPA, in children 5 studies reported null findings |
|
Abbreviations: BMI, body mass index; LPA, light physical activity; MVPA, moderate-to-vigorous physical activity; PA, physical activity. |
||
Adiposity
A total of 20 observational studies—3 longitudinal and 17 cross-sectional studies—examined the association between sleep timing and adiposity in children and adolescents 4 to 18 years old. Two of the 3 longitudinal studies reported that later sleep timing was associated with higher adiposityFootnote 15Footnote 16, while the third reported null findingsFootnote 17. Of the 17 cross-sectional studies investigating the association between sleep timing and adiposity, 10 reported null findings; of these, 2 studies only investigated BMIFootnote 28Footnote 31, 1 study only investigated waist circumferenceFootnote 27 and 7 studies used BMI and at least one additional measure of adiposityFootnote 25Footnote 26Footnote 29Footnote 30Footnote 32Footnote 33Footnote 34. Five studies reported mixed findings in the associations between sleep timing and adiposityFootnote 19Footnote 21Footnote 22Footnote 23Footnote 24. Two studies that assigned participants to one of four sleep-timing groups by dichotomizing bedtimes and wake-up times reported a significant association between sleep-timing groups and an adiposity outcome. Relative to the early-bed/early-rise group, those in the late-to-bed sleep-timing groups had higher BMI z-scoreFootnote 18 and greater odds of having overweight and obesityFootnote 20.
The quality of evidence for the 3 longitudinal studies investigating the association between sleep timing and adiposity was downgraded from low to very low due to a serious risk of bias. The quality of the evidence for the 17 cross-sectional studies investigating this association was downgraded from low to very low due to inconsistency in the findings.
Emotional regulation
A total of 9 observational studies—2 longitudinal and 7 cross-sectional—reported on the association between sleep timing and emotional regulation in children and adolescents 4 to 20 years old. In children, being categorized as having a late bedtime over multiple timepoints was significantly associated with more behavioural problemsFootnote 16. The other longitudinal study reported mixed findings between sleep timing at different time points and emotional distressFootnote 35. Eight cross-sectional studies were initially extracted, but to avoid inflating the results in the emotional regulation outcome, one of the studies by Short and colleaguesFootnote 49 was removed as the authors published twice on the same outcome measurement, using the same sample and the same statistical analysis. The study by Short et al.Footnote 39 had the highest number of outcome measurements within the emotional regulation health outcome and was therefore retained (see Supplementary Table 2). Of the remaining 7 cross-sectional studies, 2 reported mixed findingsFootnote 38Footnote 41. Three studies reported that later bedtime was associated with more behavioural problemsFootnote 40, depressive symptomsFootnote 36Footnote 39 and anxietyFootnote 39. Compared to a bedtime at approximately 22:00 or earlier, bedtime between 22:30 and 23:00 was associated with lower depression symptoms among adolescents, while bedtime at 23:00 or later was associated with higher depression symptoms, anxiety or nervousness, feeling irritated and having tantrumsFootnote 37. Wang and colleaguesFootnote 42 reported that in Grade 12 adolescents, an earlier wake-up time was associated with less academic stress.
The quality of evidence for the 2 longitudinal studies and the remaining 7 cross-sectional studies investigating the association between sleep timing and emotional regulation was downgraded from low to very low due to serious risk of bias.
Cognitive function and academic achievement
Of the 7 studies reporting on cognitive function/academic performance in children and adolescents 4 to 20 years old, 2 were longitudinal and 5 were cross-sectional. One longitudinal study reported null findings between sleep timing and cognitive performanceFootnote 16, while the other reported mixed findings, with only school-year bedtime across the timepoints associated with academic performanceFootnote 35. Of the 5 cross-sectional studies, 2 studies reported null findingsFootnote 41Footnote 44, 1 study reported mixed findingsFootnote 42 and 2 studies reported significant associationsFootnote 37Footnote 43. In a large sample of older adolescents aged 14 to 20 years, compared to a bedtime between 22:00 and 22:59, bedtimes before 22:00 or after 00:00 were associated with increased odds of poor academic performanceFootnote 37. Among adolescents aged 16 to 19 years, compared to a bedtime at 22:00 or earlier, later bedtimes were associated with difficulties following in class, completing homework assignments, preparing for exams and with writing and reading tasksFootnote 43.
The quality of evidence was downgraded from low to very low due to serious risk of bias and inconsistency in the findings for the 2 longitudinal studies and due to serious risk of bias for the 5 cross-sectional studies.
Quality of life and well-being
Two studies, one longitudinal and the other cross-sectional, reported on the association between sleep timing and quality of life and well-being. Longitudinal findings revealed that reoccurring late bedtime over multiple timepoints was associated with lower psychosocial and physical health functioning in children aged 4 to 9 yearsFootnote 16. The cross-sectional study, in children aged 9 to 11 years, reported null findings for the overall association between midpoint of sleep and health-related quality of lifeFootnote 45.
The quality of evidence for both studies was downgraded from low to very low, due to serious risk of imprecision for the longitudinal study and for the cross-sectional study.
Accidents/injuries
A single cross-sectional study reported on the association between sleep timing and accidents/injuries. A bedtime at approximately 23:00 for adolescents was associated with the lowest odds of having an accident at recess, in the classroom and on the way to school, relative to a bedtime at 22:00 or earlier; however, no association was reported between sleep timing and accidents during gym classFootnote 37.
The quality of evidence was downgraded from low to very low due to serious risk of bias and imprecision.
Biomarkers of cardiometabolic risk
Seven cross-sectional studies examined the association between sleep timing and biomarkers of cardiometabolic risk (e.g. insulin, lipid profile, blood pressure) in children and adolescents between 8 and 19 years old. Out of these 7 studies, 2 reported null findingsFootnote 30Footnote 33 and 5 reported mixed findingsFootnote 27Footnote 28Footnote 29Footnote 46Footnote 47.
The quality of the evidence for the 7 cross-sectional studies was downgraded from low to very low due to inconsistency in the findings.
Sleep duration and quality
Initially, 12 studies were extracted for the sleep duration and quality health outcome; however, to avoid inflating the results in this outcome, one of the studies by Short and colleaguesFootnote 39 was removed because the authors published twice on the same outcome measurement and using the same sample and statistical analysis. The study by Short et al.Footnote 49 had the highest number of measurements within the sleep duration and quality health outcome and was therefore retained (see Supplementary Table 3).
A total of 11 observational studies, 1 longitudinal and 10 cross-sectional, examined the association between sleep timing and sleep duration and quality. The longitudinal study reported null findings between sleep timing and sleep duration in childrenFootnote 17. Of the 10 cross-sectional studies in children and adolescents 5 to 20 years old, 5 studies reported that later bedtime, wake-up time or midpoint of sleep were associated with significantly shorter total sleep timeFootnote 20Footnote 23Footnote 25Footnote 31Footnote 50; 1 reported that later bedtime was associated with shorter total sleep time as well as lower quality of sleepFootnote 49; 1 reported that later bedtime was associated with more sleep quality problemsFootnote 37; 1 reported mixed findings with a significant association between later midpoint of sleep and lower sleep quality, but no association between midpoint of sleep and sleep durationFootnote 48; and 2 reported null findings between sleep timing and sleep durationFootnote 15Footnote 51.
The quality of evidence for the longitudinal study was downgraded from low to very low due to imprecision in the findings. The quality of the evidence for the cross-sectional studies was downgraded from low to very low due to serious risk of bias.
Eating behaviours
A total of 13 cross-sectional studies examined the association between sleep timing and eating behaviours in children and adolescents between 5 and 18 years old. Of these 13 studies, 4 reported null findingsFootnote 15Footnote 24Footnote 29Footnote 56; 6 reported mixed findingsFootnote 18Footnote 26Footnote 31Footnote 51Footnote 53Footnote 55; and 3 reported significant associationsFootnote 23Footnote 52Footnote 54. In children and adolescents aged 9 to 17 years, later bedtime was associated with greater consumption of junk food and missing breakfast more oftenFootnote 52. Later bedtime was also associated with a higher amount of unhealthy food consumption and a lower amount of healthy food consumption in children aged 9 to 11 yearsFootnote 54. In children aged 6 to 10 years, a later midpoint of sleep was associated with a higher eating risk factor scoreFootnote 23.
The quality of evidence for the studies with the eating behaviour health outcome was downgraded from low to very low due to serious risk of bias.
Physical activity and sedentary behaviour
A total of 16 observational studies, including 1 longitudinal and 15 cross-sectional studies, examined the association between sleep timing and physical activity and sedentary behaviour. Antczak and colleagues’Footnote 57 longitudinal findings showed that later bedtime in children was associated with significantly higher sedentary time and lower amount of physical activity at all intensities. Of the 15 cross-sectional studies, 5 reported null findingsFootnote 15Footnote 23Footnote 25Footnote 31Footnote 60; 5 reported mixed findingsFootnote 24Footnote 26Footnote 32Footnote 56Footnote 59; and 5 reported significant associations between sleep timing and physical activity and sedentary behaviourFootnote 20Footnote 48Footnote 50Footnote 54Footnote 58. Two studies in children and adolescents reported that later bedtime was significantly associated with less moderate-to-vigorous physical activity and more sedentary behaviours including screen timeFootnote 20Footnote 54. A study that measured bedtime and physical activity and sedentary behaviour at two different time points reported that later bedtime was associated with more sedentary time and more light physical activity at age 5 years; at age 7 years, later bedtime was also associated with more sedentary time and more light physical activity but also with more moderate-to-vigorous physical activityFootnote 50. One study showed that later weekday and weekend midpoint of sleep was associated with more screen time across multiple devices in children and adolescentsFootnote 48. In children, 2 studies reported that later bedtime and sleep onset, independent of sleep duration or wake-up time, were associated with less physical activityFootnote 58.
The quality of evidence was downgraded from low to very low due to imprecision for the longitudinal study and due to serious risk of bias for the cross-sectional studies.
Discussion
Many characteristics of sleep are important for good health. We conducted the present systematic review to improve understanding of the association between sleep timing and health in a population of children and adolescents. Our objectives were to update the knowledge for the sleep recommendations in the Canadian 24-Hour Movement Guidelines for Children and YouthFootnote 5 and to provide evidence that can be used to better inform the development of future evidence-based healthy sleep interventions.
This systematic review synthesized peer-reviewed scientific evidence from 46 observational studies, including 5 longitudinal and 41 cross-sectional studies, across 21 countries. Overall, the findings suggest that later sleep timing may be associated with poorer emotional regulation, cognitive function/academic performance, eating behaviours, lower sleep duration and quality, and lower physical activity and higher sedentary behaviours. The findings were sparse or less consistent for the associations between sleep timing and adiposity, quality of life/well-being, accidents/injuries and cardiometabolic risk. The quality of the evidence was rated as very low according to GRADE for all outcomes.
The majority of studies that examined the critical outcomes reported on adiposity (n = 20), while studies on accidents/injuries (n = 1) and quality of life/well-being (n = 2) were underrepresented. Studies reporting on the important health outcomes were more evenly spread with 16 studies reporting on the physical activity and sedentary behaviour outcome, 13 on eating behaviour, 11 on sleep duration/quality and 7 on cardiometabolic risk (Table 3).
The evidence presented for the association between sleep timing and adiposity is inconsistent, as more than half of the studies reported null findings (n = 11), which mirrors findings from a recently published systematic review by Chaput et al. in adultsFootnote 61. Another finding in both this review and Chaput et al.’sFootnote 61 systematic review was that later sleep timing was associated with lower physical activity and higher sedentary behaviour. In addition, both these systematic reviews identified a lack of studies investigating the association between sleep timing and accidents/injuries or quality of life/well-being in their respective populations.
The findings between the two systematic reviews differed for some outcomes. Our current findings indicate that later sleep timing was generally associated with poorer emotional regulation and cognitive function/academic performance in children and adolescents, whereas in adults the associations for mental health and cognitive function were inconsistentFootnote 61. In children and adolescents, more studies are needed to confirm these associations (especially longitudinal studies and randomized trials), including the mechanisms behind them.
Some of the health outcomes we considered in this systematic review differed from those chosen for the adult populationFootnote 61. For example, we reviewed the association between sleep timing and eating behaviour in this paper. In children and adolescents, later sleep timing was associated with poorer eating behaviours; this is of concern given that eating behaviours are also independently associated with health outcomesFootnote 62. In addition, as children and adolescents do not always have full control over their eating behaviours, investigating the moderating effect of socioeconomic status, parental figure influence and family structure in the association between sleep timing and eating behaviours of children and adolescents is essential.
In the articles included in this present review, sleep timing was mainly assessed using bedtime, wake-up time, midpoint of sleep or a combination of dichotomized bedtime and wake-up times divided into four different sleep-timing groups. None of these measurements of sleep timing account for sleep duration; in fact, very few studies adequately controlled for sleep duration in their analyses. Controlling for sleep duration is important given the well-established associations between short sleep duration and higher adiposity, lower emotional regulation, lower academic achievement, lower quality of life/well-beingFootnote 2, lower cognitive performanceFootnote 63 and altered brain functions and structuresFootnote 64.
Not surprisingly, one of the most consistent findings in the present systematic review is the association between later sleep timing and shorter sleep duration (given that school start times are fixed). In addition to controlling for sleep duration in observational studies, this research area requires intervention studies that modify sleep timing. Our systematic review did not identify even a single intervention study that focussed on sleep timing. Future intervention studies should try to manipulate sleep timing while maintaining a constant sleep duration (e.g. sleep duration of 8 hours in adolescents, with one group sleeping from 22:00 to 6:00 and the other from 00:00 to 8:00) to understand the effects of sleep timing, independent of sleep duration, on health outcomes.
Strengths and limitations
Our findings should be interpreted in light of the following limitations. The low number of studies and their heterogeneity made comparisons problematic and meta-analyses ill-advised for all health outcomes. Opting for a narrative synthesis prevents adequate weighting of the included studies. In addition, we could not assess publication bias, which is a pervasive problem in the reporting of scientific findings. However, choosing to only include studies published in the last 10 years could have somewhat mitigated that risk, as many more journals have published null findings more frequently in recent years.
A strength of this review is our comprehensive search strategy. However, the studies selected for this review were not without limitations; the quality of evidence included was rated as very low according to GRADE, even considering that GRADE defaults all study designs other than randomized trials to “low quality.” The contributing factors for the quality of evidence included study design (mainly cross-sectional studies), serious risk of bias, imprecision and inconsistency. In addition, only a few of the included studies adequately controlled for sleep duration, which makes it difficult to interpret the findings. A large proportion of the included studies relied on a small sample size or used statistical analyses (e.g. correlations) that prevented controlling for important covariates. Almost half of the studies (n = 22) used a subjective assessment for sleep timing, with many using a single question or a questionnaire with unknown psychometric properties. Although this means that more than half of the studies (n = 24) used an objective measure of sleep timing, the number of nights recorded differed greatly across studies.
Conclusion
The evidence suggests that later sleep timing may be associated with poorer health outcomes in children and adolescents, namely emotional regulation, cognitive function/academic performance, sleep duration/quality, eating behaviours and physical activity and sedentary behaviours. However, the findings have predominantly been generated from cross-sectional evidence and studies with stronger designs are needed to investigate the association between sleep timing and health outcomes independent of sleep duration in the pediatric population.
No bedtime recommendation can be proposed based on the available evidence as the evidence presented was modest and the findings reported mostly linear associations. Nevertheless, having an early enough bedtime that allows children and adolescents to meet sleep duration recommendations would be a sensible public health recommendation based on the current findings and the body of evidence that links short sleep duration to adverse health outcomes.
Registration of the protocol
PROSPERO registration no. CRD42020173585; available online. No amendment was made to the protocol or information that was provided at registration.
Acknowledgements
This work was supported in part by an Early Researcher Award from the Ministry of Research and Innovation. We would like to thank Margaret Sampson, a former research librarian, for taking the time to review our search strategy; we wish her a happy retirement.
Conflicts of interests
No competing interests are declared by the authors.
Authors’ contributions and statement
CD, CMS, BGC and JPC screened the papers.
CD and IP extracted the data and performed the quality assessment.
CD drafted the final version of the manuscript under the guidance of JPC.
All authors were involved in the study conception and reviewed and approved the final version of this article for publication.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.