
Original quantitative research – Impact of substance-related harms on injury hospitalizations in Canada, from 2010 to 2020

HPCDP Journal Home
Published by: The Public Health Agency of Canada
Date published: March 2023
ISSN: 2368-738X
Submit a manuscript
About HPCDP
Browse
Previous | Table of Contents | Next
Stephanie Toigo, MSc; Steven R. McFaull, MSc; Wendy Thompson, MSc
https://doi.org/10.24095/hpcdp.43.3.03
This article has been peer reviewed.
Author references
Public Health Agency of Canada, Ottawa, Ontario, Canada
Correspondence
Stephanie Toigo, Injury Surveillance, Centre for Surveillance and Applied Research, Public Health Agency of Canada, 785 Carling Avenue, Ottawa, ON K1A 0K9; Email: stephanie.toigo@phac-aspc.gc.ca
Suggested citation
Toigo S, McFaull SR, Thompson W. Impact of substance-related harms on injury hospitalizations in Canada, from 2010 to 2020. Health Promot Chronic Dis Prev Can. 2023;43(3):130-8. https://doi.org/10.24095/hpcdp.43.3.03
Abstract
Introduction: Injuries continue to be a leading cause of death and contribute significantly to hospitalizations each year in Canada. Substance use has been associated with an increase in intentional and unintentional injuries, resulting in hospitalizations. This study examines trends in injury hospitalizations with a co-occurring substance diagnosis, to quantify the burden of injuries and identify at risk populations.
Methods: We analyzed Discharge Abstract Database data between 2010/11 and 2020/21, for clinical and demographic information about hospital discharges across Canada. We used ICD-10 codes to identify injury hospitalizations with co-occurring substance diagnostic codes, by injury intent and substance type. Rates, proportions, age-specific rates and age-standardized rates were calculated, trends quantified using average annual percent change and results stratified by sex and age group.
Results: From 2010/11 to 2020/21, unintentional injuries accounted for over half of all substance-related injury hospitalizations. Substance-related injuries accounted for 12% of total injury hospitalizations over this period. Overall, substance-related injury hospitalizations with co-occurring use of stimulants, opioids, cannabinoids and alcohol increased significantly among males and females. Unintentional substance-related, injury hospitalizations were more common later in life, and intentional substance-related injuries were more common among adolescents and young adults.
Conclusion: These results highlight key demographic groups with higher rates of substance-related injury hospitalizations that would benefit from targeted prevention efforts.
Keywords: surveillance, trends, Canada, unintentional injury, intentional injury, alcohol, polysubstance, psychoactive substances
Highlights
- Injuries with a substance diagnosis accounted for 12% of total injury hospitalizations in Canada over the past 11 years.
- Between 2010/11 and 2020/21, substance-related injury hospitalizations increased significantly.
- Polysubstance (multiple substance group codes, e.g. cannabinoids and alcohol, during an episode of care), alcohol and unspecified psychoactive substances were the substance groups most frequently reported with injury hospitalizations.
- Injury hospitalizations with the use of polysubstance and unspecified psychoactive substances were more frequent among children and youth.
- Alcohol and opioid-related injury hospitalizations were more frequent among older adults.
Introduction
Injuries have been a leading cause of death in Canada over the past two decades.Footnote 1 Injuries contribute significantly to hospitalization rates each year (600 per 100 000 people), with over 270 000 injury-related hospitalizations in the 2018/19 fiscal year.Footnote 2
Injuries are often grouped by intent: unintentional injuries, which are injuries that occur without intention to harm, versus intentional injuries, that are the result of purposeful harm to oneself or another person.Footnote 3 Injuries can be further classified by their external cause. In 2018/19, the largest proportion of unintentional injuries, by external cause, included unintentional falls, poisonings and motor vehicle collisions. Non-fatal suicide attempts and self-inflicted injuries made up the largest proportion of intentional injuries.Footnote 2
It is well-known that substance use contributes to injuries, regardless of cause.Footnote 4Footnote 5 Studies have reported that the odds of experiencing an intentional injury when consuming substances are much greater than of experiencing an unintentional injury.Footnote 4Footnote 5 In addition, compared to when not using any substances, using alcohol alone or with other drugs increases the likelihood of an intentional injury by 4 to 18 times.Footnote 4Footnote 5 Alcohol- and cannabis-related injuries have been consistently studied over a number of years.Footnote 5Footnote 6Footnote 7Footnote 8Footnote 9 In more recent years, research has also found a positive association between opioid use and injuries.Footnote 10Footnote 11Footnote 12
We analyzed trends in injury hospitalizations in Canada that co-occurred with a substance use diagnosis from 2010/11 to 2020/21 (each fiscal year lasts from 1 April to 31 March). We describe substance-related injury hospitalizations by age group, sex, injury intent and substance type. Analyzing trends using national hospitalization data provides a better understanding of the burden and pattern of injuries, allowing for greater focus on prevention.
Methods
Data source and case definition
This study utilized data from the Discharge Abstract Database (DAD), a national database managed by the Canadian Institute for Health Information (CIHI). The DAD collects administrative, clinical and demographic information on hospital discharges, from all provinces and territories except Quebec. Our study focussed on acute care inpatient discharge records. We excluded injuries due to the adverse effects of drugs or surgical or medical errors. We also excluded any uncertain or secondary diagnoses. Uncertain diagnoses are those that are suspect or questionable; secondary diagnoses are those that did not receive treatment or that did not contribute significantly to the episode of care.Footnote 13
The DAD uses the International Classification of Diseases, 10th Revision (ICD-10) codes to classify reported diagnoses and interventions. These codes classify injuries, conditions and situations that may be risk factors to health.Footnote 13
Case identification
We first identified all injury-related hospitalizations in the DAD by searching all 25 diagnosis fields for external cause of injury codes. An injury hospitalization is defined as any entry in the DAD where one of the external causes of injury (codes as listed in Chapter 20 of the ICD-10Footnote 13) has been recorded. The framework for selecting and grouping external cause of injury codes is based on methodology used by CIHI and the US Centers for Disease Control and Prevention.Footnote 14 ICD-10 codes used to classify external cause of injuries have been grouped by intent: unintentional; intentional (self-harm, assault, self-inflicted injury); legal intervention (injuries inflicted by the police or other law-enforcing agents in the course of arresting lawbreakers or maintaining order) or undetermined intent. We excluded entries where the intent overlapped (0.4% of injury hospitalizations) to prevent misclassification.
See Figure 1 for a visual representation of the process we used in this study to identify cases in the DAD.
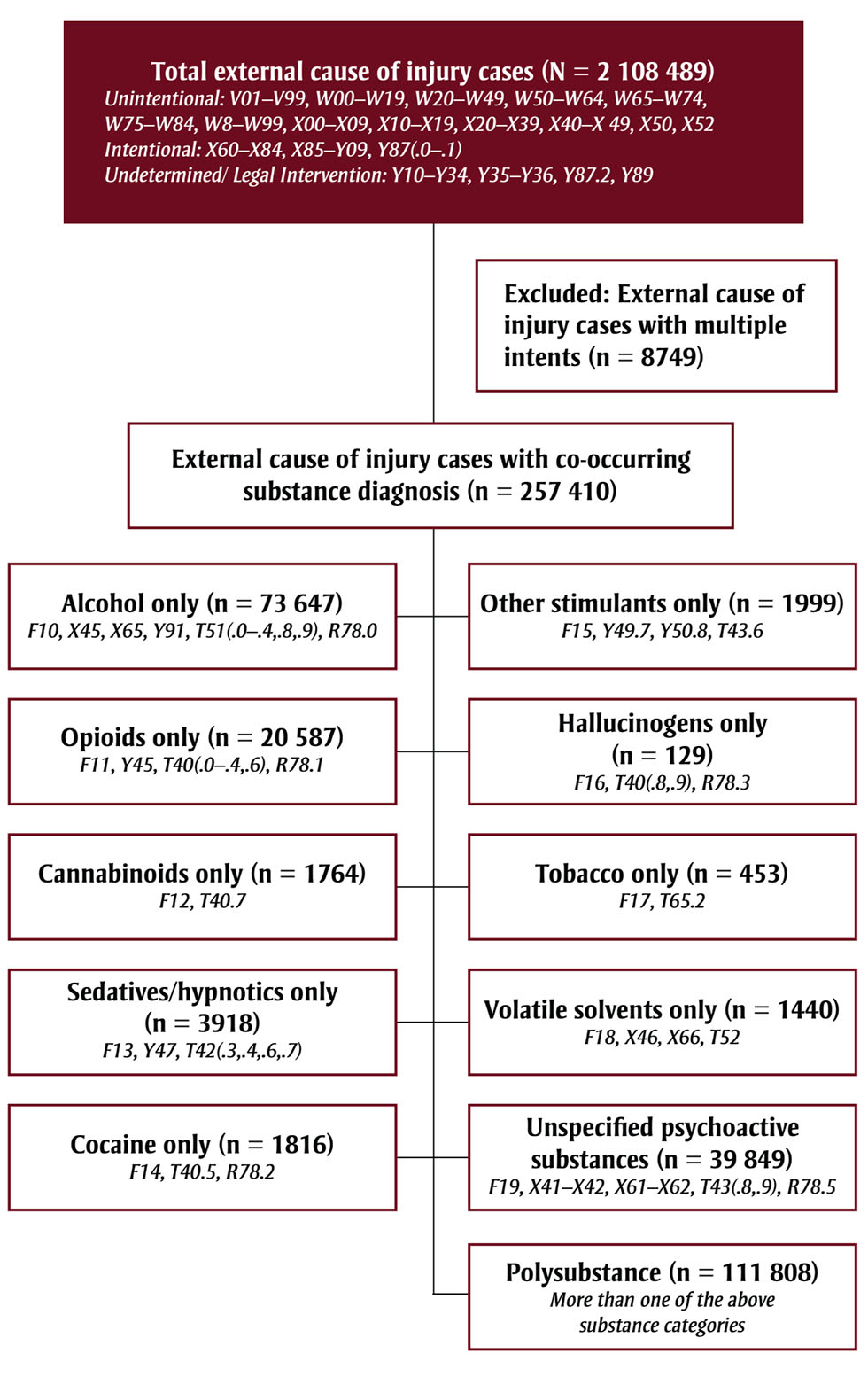
Figure 1 - Text description
This figure illustrates the selection process of cases for inclusion in the article.
Phase 1: A total of N = 2 108 489 cases of external causes of injury were found in the discharge abstract database. The figure shows that the following ICD-10 codes were included:
- Unintentional: V01–V99, W00–W19, W20–W49, W50–W64, W65–W74, W75–W84, W8–W99, X00–X09, X10–X19, X20–X39, X40–X 49, X50, X52
- Intentional: X60–X84, X85–Y09, Y87(.0-.1)
- Undetermined/ Legal Intervention: Y10–Y34, Y35–Y36, Y87.2, Y89
Phase 2: A total of n = 8749 were excluded because they were classified as external cause of
injury cases with multiple intents.
Phase 3: Out of the remaining cases, a new total of n = 257 410 was identified as having an external cause of injury cases with co-occurring substance diagnosis. The new total is broken down as follows:
- n = 73 647 were identified as alcohol-only (ICD-10 codes F10, X45, X65, Y91, T51(.0–.4,.8,.9), and R78.0).
- n = 20 587 were identified as opioids-only (ICD-10 codes F11, Y45, T40(.0-.4,.6) and R78.1).
- n = 1764 were identified as cannabinoids-only (ICD-10 codes F12, T40.7).
- n = 3918 were identified as sedatives/hypnotics-only (ICD-10 codes F13, Y47,T42(.3,.4,.6,.7)).
- n = 1816 were identified as cocaine-only (ICD-10 codes F14, T40.5, R78.2).
- n = 1999 were identified as other stimulants-only (ICD-10 codes F15, Y49.7, Y50.8, T43.6).
- n = 129 were identified as hallucinogens-only (ICD-10 codes F16, T40(.8,.9) R78.3).
- n = 453 were identified as tobacco-only (ICD-10 codes F17, T65.2).
- n = 1440 were identified as volatile solvents-only (ICD-10 codes F18, X46, X66, T52).
- n = 39 849 were identified as unspecified psychoactive substances (ICD-10 codes F19, X41–X42, X61–X62, T43(.8,.9), R78.5).
- n = 111 808 were identified as polysubstance (i.e. more than one of the above substance categories).
Abbreviation: ICD-10, International Classification of Diseases, 10th Revision.
Abbreviation: ICD-10, International Classification of Diseases, 10th Revision.
We applied substance diagnostic codes to the extracted injury cases to identify injury hospitalizations that had a co-occurring substance diagnostic code for the episode of care. Throughout this article, we refer to substance-related injury hospitalizations as injury hospitalizations that have a co-occurring substance diagnostic code recorded for the episode of care. A hospitalization with both an injury and a substance diagnostic code does not necessarily mean that the substance was a direct cause of the injury; causality should not be assumed.
The substance groups we identify in this study are alcohol, opioids, cannabinoids, sedatives or hypnotics, cocaine, other stimulants (including caffeine), hallucinogens, tobacco, volatile solvents, unspecified psychoactive substance and polysubstance (see Figure 1). The term “polysubstance” refers to multiple substance group codes (e.g. cannabinoids and alcohol) recorded for a patient during the episode of care.
Statistical analyses
We analyzed substance-related injury hospitalizations that occurred over an 11-year period between 2010/11 and 2020/21. The primary variables analyzed were age group, sex (male and female), fiscal year, external cause of injury and substance type. Results were disaggregated by sex, but because of low counts for the “other” category, we could only present data for males and females. Gender was not a variable available in the DAD at the time of this analysis.
We calculated age-specific rates per 100 000 population using Statistics Canada population estimates over the 11-year period. Age-standardized rates per 100 000 were directly standardized to the 2011 Canadian population. Since the DAD captures all hospitalization records in Canada (excluding Quebec), confidence intervals (CIs) did not need to be calculated as there is no real level of uncertainty around the estimates.
We quantified annual trends in age-standardized rates using annual percent change (APC) and average annual percent change (AAPC).Footnote 15 Age-standardized rates that changed significantly over the time period are identified by an APC or AAPC that differs significantly from zero (α = 0.05).
We used SAS EG version 7.1 (SAS Institute Inc., Cary, NC, US) for all descriptive analyses and to calculate age-specific rates. We used Joinpoint Regression Program version 4.7.0.0 (SEERStat, NCI, Bethesda, MD, US) to analyse injury and substance use trends using age-standardized rates, by sex and fiscal year. The Joinpoint software fits the simplest Joinpoint regression model using the permutation test; this allows the identification of inflection points within the series with multiple weighted segments. We calculated 95% CIs for each segment to highlight the random error around the modelled APC.Footnote 15
Results
Overview of substance-related injury hospitalizations
Between 2010/11 and 2020/21, there were 2 099 740 acute inpatient hospitalizations for injuries of any external cause in Canada (excluding Quebec). Females accounted for 52.4% (n = 1 100 808) of these injuries, of which 11.2% (n = 123 642) were substance related. Of the 998 932 injury hospitalizations of males, 13.4% (n = 133 768) had a substance-related diagnosis.
Poisoning injuries overall made up 5.1% of unintentional injury hospitalizations and 59.0% of intentional injury hospitalizations.
Of the total substance-related injury hospitalizations (n = 257 410), 53.5% were classified as unintentional injuries, 40.2% as intentional injuries and 6.3% as legal interventions or undetermined-intent injuries. A larger proportion of males than of females were hospitalized for unintentional substance-related injuries, while females made up a higher proportion of intentional substance-related injury hospitalizations.
The substance groups most commonly reported along with injury hospitalizations were polysubstance (males: 20.6%; females: 22.9%), alcohol (males: 19.4%; females: 9.2%) and unspecified psychoactive substances (males: 5.9%; females: 9.6%). Alcohol, opioids, sedatives, unspecified psychoactive substances and polysubstance together made up over 90% of substance-related injury hospitalizations for each age group (see Figure 2). The substances most frequently consumed concurrently with another substance were sedatives (45.1%), opioids (42.4%) and alcohol (28.3%).
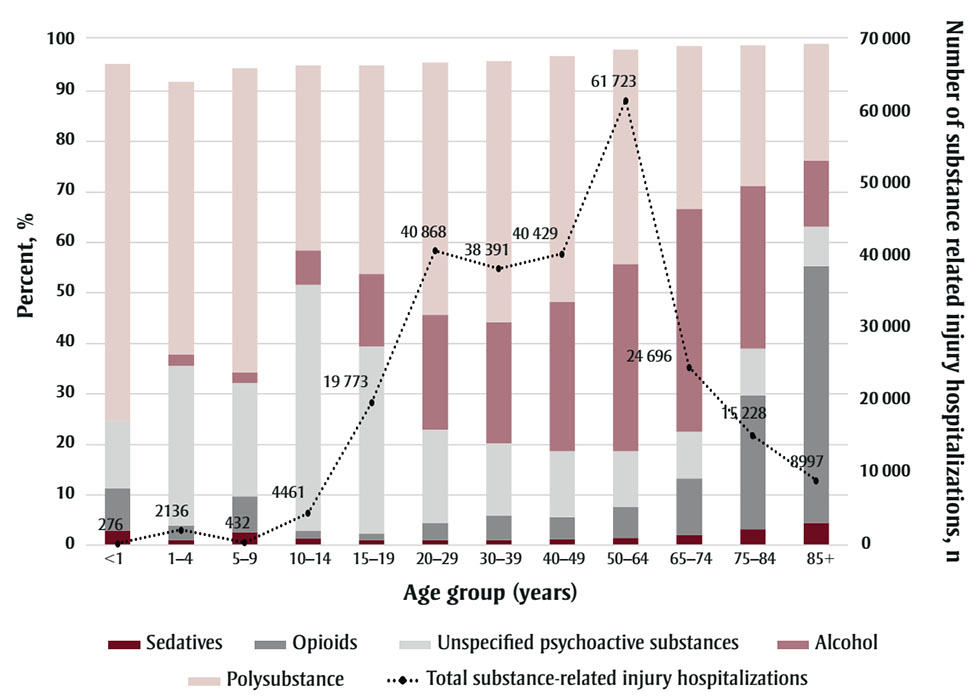
Figure 2 - Text description
| Age groups | Total substance-related injury hospitalizations (n) | % Alcohol | % Opioids | % Sedatives | % Polysubstance | % Unspecified psychoactive substances |
|---|---|---|---|---|---|---|
| <1 | 276 | Not available | 8.3 | 2.9 | 70.7 | 13.4 |
| 1-4 | 2136 | 2.3 | 2.9 | 1.0 | 53.9 | 31.6 |
| 5-9 | 432 | 2.1 | 7.2 | 2.5 | 60.2 | 22.5 |
| 10-14 | 4461 | 6.8 | 1.6 | 1.3 | 36.6 | 48.7 |
| 15-19 | 19773 | 14.4 | 1.3 | 1.1 | 41.3 | 37.0 |
| 20-29 | 40868 | 22.8 | 3.4 | 1.0 | 50.0 | 18.5 |
| 30-39 | 38391 | 24.0 | 4.8 | 1.1 | 51.7 | 14.4 |
| 40-49 | 40429 | 29.6 | 4.4 | 1.2 | 48.7 | 13.1 |
| 50-64 | 61723 | 37.2 | 6.1 | 1.5 | 42.4 | 11.0 |
| 65-74 | 24696 | 44.2 | 11.2 | 2.0 | 32.2 | 9.3 |
| 75-84 | 15228 | 32.3 | 26.5 | 3.2 | 27.8 | 9.2 |
| 85+ | 8997 | 13.1 | 51.0 | 4.4 | 23.2 | 7.7 |
Polysubstance use most frequently co-occurred with injury hospitalizations in younger age groups, among whom most of the injuries were unintentional. Unspecified psychoactive substance-related injury hospitalizations were also common among youth, among whom they were unintentional for 88.7% of those aged 10 to 14 years and for 87.7% of those aged 15 to 19 years.
Alcohol use most frequently co-occurred with injury hospitalizations among older adults aged 65 to 74 years and 75 to 84 years, with 93.5% and 96.4%, respectively, of these injuries being unintentional. For those aged 85 years plus, opioid use most frequently co-occurred with injury hospitalizations, and 98.5% of these injuries were unintentional.
Trends in substance-related injury hospitalizations
From 2010/11 to 2020/21, age-standardized rates of substance-related injury hospitalizations of males increased significantly, by 2.1%. Among females, age-standardized rates of substance-related injury hospitalizations increased significantly from 2010/11 to 2016/17, by 2.6%, and then decreased significantly from 2016/17 to 2020/21, by 2.4% (see Figure 3), resulting in an overall significant increase of 0.6% from 2010/11 to 2020/21. In comparison, rates of total injury hospitalizations decreased significantly during this period.
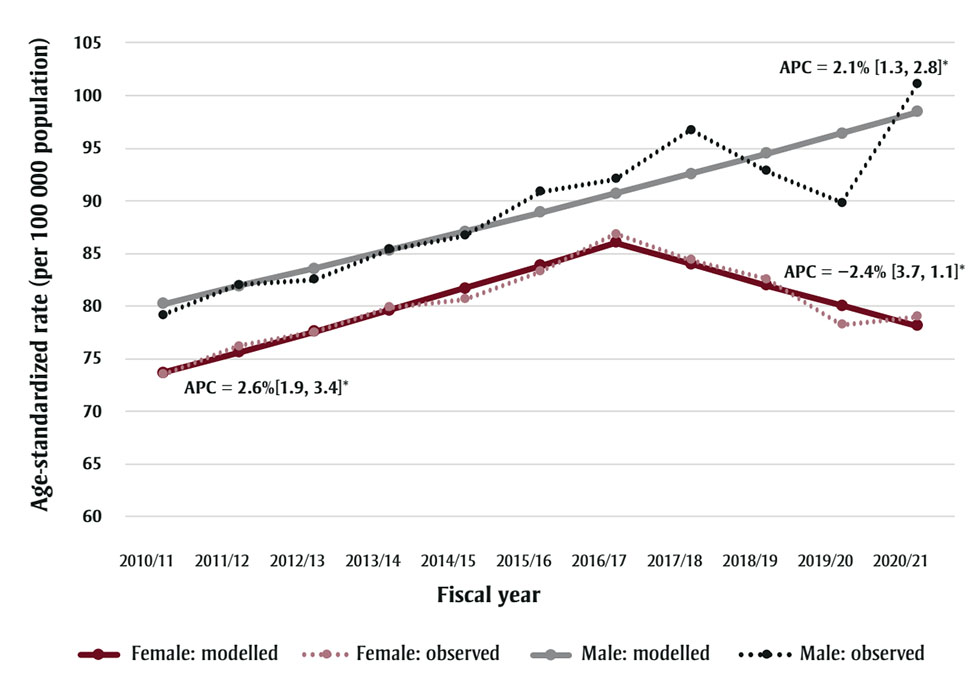
Figure 3 - Text description
| Females | Males | ||||||
|---|---|---|---|---|---|---|---|
| Fiscal year | Observed Age-Standardized Rate | Standard Error | Modeled Age-Standardized Rate | Fiscal Year | Observed Age-Standardized Rate | Standard Error | Modeled Age-Standardized Rate |
| 2010/11 | 73.53 | 0.75 | 73.67 | 2010/11 | 79.19 | 0.79 | 80.23 |
| 2011/12 | 76.21 | 0.76 | 75.6 | 2011/12 | 82.02 | 0.8 | 81.89 |
| 2012/13 | 77.5 | 0.76 | 77.58 | 2012/13 | 82.52 | 0.8 | 83.58 |
| 2013/14 | 79.9 | 0.77 | 79.62 | 2013/14 | 85.36 | 0.81 | 85.31 |
| 2014/15 | 80.64 | 0.77 | 81.71 | 2014/15 | 86.68 | 0.81 | 87.07 |
| 2015/16 | 83.3 | 0.78 | 83.85 | 2015/16 | 90.84 | 0.82 | 88.86 |
| 2016/17 | 86.87 | 0.79 | 86.05 | 2016/17 | 92.08 | 0.82 | 90.7 |
| 2017/18 | 84.36 | 0.78 | 83.99 | 2017/18 | 96.73 | 0.84 | 92.57 |
| 2018/19 | 82.59 | 0.76 | 81.98 | 2018/19 | 92.83 | 0.81 | 94.48 |
| 2019/20 | 78.22 | 0.74 | 80.02 | 2019/20 | 89.83 | 0.79 | 96.43 |
| 2020/21 | 79.02 | 0.74 | 78.1 | 2020/21 | 101.05 | 0.84 | 98.42 |
For males, age-standardized rates of substance-related injury hospitalizations involving polysubstance, alcohol, opioids, stimulants and cannabinoids significantly increased between 2010/11 and 2020/21. For females, rates of injury hospitalizations involving alcohol, unspecified psychoactive substances, opioids, stimulants and cannabinoids significantly increased (see Table 1). For males only sedatives and volatile solvents showed significantly declining trends and for females only sedatives showed declining trends over this period.
| Substance type | Prevalence, n (%) |
AAPC (95% CI), % | |
|---|---|---|---|
| Males | Females | ||
| Polysubstance | 111 808 (43.4) | +3.3 (2.1, 4.6)Footnote * | +0.0 (0.6, 0.7) |
| Alcohol | 73 647 (28.6) | +0.9 (0.1, 1.7)Footnote * | +0.9 (0.1, 1.7)Footnote * |
| Unspecified psychoactive substances | 39 849 (15.5) | +0.3 (−0.6, 1.3) | +1.7 (0.3, 3.2)Footnote * |
| Opioids | 20 587 (8.0) | +3.4 (1.8, 5.1)Footnote * | +1.0 (0.3, 1.7)Footnote * |
| Sedatives | 3918 (1.5) | −5.3 (−7.0, −3.4)Footnote * | −7.7 (−10.0, −5.3)Footnote * |
| Stimulants | 1999 (0.8) | +21.8 (18.3, 25.4)Footnote * | +18.4 (12.9, 24.3)Footnote * |
| Cocaine | 1816 (0.7) | +1.2 (−2.0, 4.5) | −3.6 (−7.9, 0.9) |
| Cannabinoids | 1764 (0.7) | +6.2 (3.7, 8.7)Footnote * | +7.6 (4.6, 10.6)Footnote * |
| Volatile solvents | 1440 (0.6) | −5.8 (−7.8, −3.7)Footnote * | +0.2 (−3.1, 3.6) |
| Tobacco | 453 (0.2) | +1.8 (−7.0, 11.5) | −3.9 (−13.4, 6.5) |
| Hallucinogens | 129 (0.1) | +0.2 (−6.2, 7.0) | Not available |
Substance-related injury hospitalizations across age groups
Among males, intentional substance-related injury hospitalizations peaked at age 20 to 29 years. Among females aged 15 to 19 years, the peak in intentional substance-related injury hospitalizations was about three times that of males in the same age group (see Figure 4).
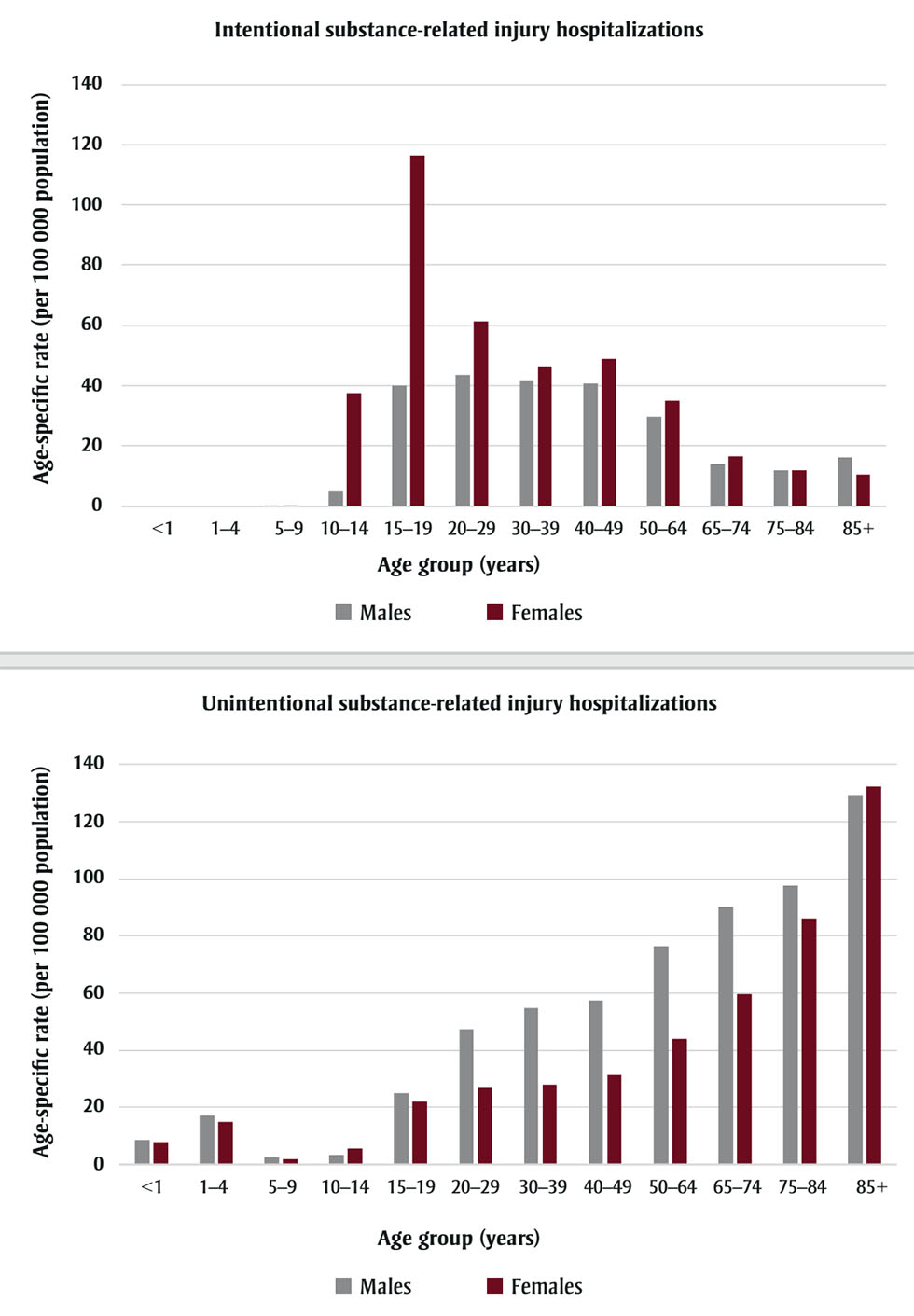
Figure 4 - Text description
| Age group | Males with intentional substance-related injury hospitalizations (rate per 100 000 population) | Females with intentional substance-related injury hospitalizations (rate per 100 000 population) | Males with unintentional substance-related injury hospitalizations (rate per 100 000 population) | Females with unintentional substance-related injury hospitalizations (rate per 100 000 population) |
|---|---|---|---|---|
| <1 | Not available | Not available | 8.65 | 8.01 |
| 1-4 | Not available | Not available | 17.12 | 15.00 |
| 5-9 | 0.07 | 0.07 | 2.85 | 2.08 |
| 10-14 | 5.13 | 37.40 | 3.56 | 5.64 |
| 15-19 | 40.06 | 116.29 | 24.91 | 21.99 |
| 20-29 | 43.66 | 61.38 | 47.24 | 26.95 |
| 30-39 | 41.78 | 46.31 | 54.64 | 28.13 |
| 40-49 | 40.76 | 48.92 | 57.40 | 31.51 |
| 50-64 | 29.65 | 34.92 | 76.32 | 44.15 |
| 65-74 | 14.07 | 16.44 | 90.00 | 59.72 |
| 75-84 | 11.87 | 11.87 | 97.60 | 86.09 |
| 85+ | 16.03 | 10.52 | 129.33 | 132.25 |
The peak in unintentional substance-related injury hospitalizations occurred for both men and women at age 85 years plus. Overall, across all age groups, unintentional substance-related injury hospitalizations were more frequent among males, whereas intentional substance-related injury hospitalizations were more frequent among females.
Falls (65.8%) and motor vehicle collisions (11.4%) were the two most frequent external causes of unintentional injury hospitalizations between 2010/11 and 2020/21. The age-specific rates of total unintentional injury hospitalizations increased with age and were highest for those aged 85 years plus (men: 5315.4/100 000; women: 7112.2/100 000).
Age-specific rates of substance-related fall injury hospitalizations were highest for those aged 85 years and older, at a rate of 87.4/100 000 for men and 93.2/100 000 for women. Age-specific rates of substance-related motor vehicle collision injury hospitalizations were highest among those aged 20 to 29 years, with a hospitalization rate of 7.2/100 000 for men and 3.2/100 000 for women. Alcohol use co-occurred most frequently with fall (65.9%) and motor vehicle collision injuries (63.0%).
Age-specific rates of total intentional injury hospitalizations were slightly higher for males than females, except for females aged 10 to 14 years and 15 to 19 years, among whom intentional injuries were substantially higher. The age-specific rates of total intentional injuries peaked for men aged 20 to 29 years (139.6/100 000) and for girls aged 15 to 19 years (244.5/100 000).
Substance-related assault injury hospitalizations were recorded more frequently for males, and substance-related self-inflicted injury hospitalizations for females. Substance-related assault injuries peaked at 30 to 39 years at a rate of 9.9/100 000 for men and 3.2/100 000 for women. Substance-related self-inflicted injuries peaked among males and females aged 15 to 19 years at a rate of 35.8 and 114.4/100 000, respectively.
Among assault-related injury hospitalizations, alcohol use accounted for 68.8% of substance-related hospitalizations; among self-inflicted injury hospitalizations, polysubstance use accounted for 60.1% of substance-related injury hospitalizations.
Discussion
This study shows the recent trends in substance-related injury hospitalizations in Canada across age groups (<1 to ≥85 years). Our results reveal that unintentional injuries accounted for more than half of all substance-related injury hospitalizations from 2010/11 to 2020/21. During this period, there was a significant increase in substance-related injury hospitalizations overall, with stimulants, opioids, cannabinoids and alcohol showing a significant increase among both males and females.
Unintentional substance-related injury hospitalizations increased with age, while intentional substance-related injuries occurred more frequently among adolescents and young adults (age 15–19 and 20–29 years). Males had higher rates of unintentional substance-related injury hospitalizations related to falls and motor vehicle collisions than did females. Females had higher rates of self-inflicted substance-related intentional injury hospitalizations, while males had higher rates of assault injuries.
We found that polysubstance was the most frequently reported substance in almost all the age groups. Zuckermann et al.Footnote 16 observed an increase in use of more than one substance among Canadian high school students between 2013/14 and 2017/18. The Canadian Institute for Health Information reported that cannabis, unknown substances (including mixed substances) and alcohol were the three substance groups most commonly indicated with hospital stays for harms caused by substance use by youth aged 10 to 24 years,Footnote 17 which is in line with our findings.
Consuming multiple substances simultaneously has been attributed with increased adverse health outcomes and adds additional treatment complexity for health care providers.Footnote 18 This may explain the high rates of injury hospitalizations co-occurring with polysubstance use diagnoses in our study.
Our results indicate that injury hospitalizations co-occurring with opioid use were most prevalent among older adults aged 85 years plus, whereas previous studies observed that adults aged 65 years plus had the second highest prevalence of opioid use (11.3%) after adults aged 25 to 64 years (12.1%).Footnote 19Footnote 20 This difference in results may be due to factors such as age, pre-existing comorbidities and injury severity that require additional interventions or treatments.
Our findings show an overall increase in injury hospitalizations of both males and females co-occurring with substance use since 2010/11. There is little Canadian surveillance reporting on overall trends in substance-related hospitalizations or injury hospitalizations with substance use. Previous Canadian surveillance reports indicate that hospitalizations for harms due to any substance use increased from 2007 to 2014Footnote 21 and from 2017 to 2020.Footnote 22 US surveillance shows that the prevalence of substance use disorders among hospitalizations has increased from 2014 to 2018 by about 57%.Footnote 23
The high prevalence of alcohol use in Canada that other studies reportFootnote 20Footnote 21Footnote 24 aligns with our study results. We found alcohol to be the second most frequently reported substance associated with injury hospitalizations and that approximately 28% of all substance-related injuries involve only alcohol. Beverage alcohol is legal and readily accessible in Canada,Footnote 21 which likely explains the high prevalence of alcohol-related injury hospitalizations that we observed. Any stigma surrounding alcohol use is likely less apparent than for other substances, and individuals may be less apprehensive about seeking medical attention for injuries related to alcohol than for illegal substances.
We found that cannabinoids account for less than 1% of all substance-related injury hospitalizations, which is low relative to the proportion of the Canadian and North American population using cannabis.Footnote 20Footnote 25Footnote 26 Trends in the prevalence of cannabis use in Canada, prior to legalization in 2018, remained stable among youth and increased among adults.Footnote 27Footnote 28 After legalization, cannabis use by youth aged 15 to 17 years decreased, while use increased slightly among adults aged 18 years and older.Footnote 26 Prior to legalization, individuals may have chosen not to seek medical care while under the influence of cannabis to avoid legal repercussions.Footnote 29Footnote 30 Yet, despite being commonly considered less harmful than other psychoactive substances, cannabis can have adverse effects, especially in terms of effects on psychomotor skills.Footnote 31Footnote 32 Other countries have reported an increase in cannabis hospitalizations after legalization;Footnote 31 our results, in contrast, show increasing cannabis hospitalizations since 2010/11, with no significant changes after legalization in Canada.
Globally, the annual prevalence of illicit drug use was highest for stimulants, opioids and cocaine.Footnote 25 In Canada, overall use of illegal drugs (including cocaine, ecstasy, methamphetamines, hallucinogens and heroin) and stimulants has increased over the last several years, while use of psychoactive pharmaceuticals, sedatives and opioids has remained unchanged.Footnote 19Footnote 20Footnote 24Footnote 33 Although self-reported opioid pain reliever use in Canada has remained relatively stable since 2011,Footnote 19Footnote 20 our results show a significant increase in opioid-related injury hospitalizations over the study period. This may be due to the effects of consuming opioids contaminated with, for example, fentanyl or other synthetic opioids. Fentanyl and other synthetic opioids are very potent, and when consumed unknowingly or in combination with other substances, increase the toxicity of the substance.Footnote 18Footnote 34 In addition, stigma or apprehension about the legal ramifications of use of illegal substances may influence an individual’s decision to seek medical care.
Our results show that patterns in the rates of substance-related unintentional and intentional injury hospitalizations differ across age groups. In the case of intentional substance-related injury hospitalizations, a notable peak was observed among adolescents and young adults, particularly females aged 15 to 19 years. The most frequent external cause of injury among adolescents and young adults are those that are self-inflicted. Higher rates of self-inflicted injury hospitalizations, emergency department visits and suicide mortality among youth are well documented.Footnote 35Footnote 36Footnote 37 Lethality in self-inflicted injuries is higher among males than females, which may explain the higher rates of substance-related intentional injury hospitalizations among females than among males, as our study did not capture deaths that occur pre-admission to hospital.Footnote 38
Polysubstance use co-occurred most frequently with self-inflicted injuries, whereas alcohol use co-occurred more frequently with assault injuries. Polysubstance was most frequently identified with hospitalizations for substance harms among those aged 10 to 24 years,Footnote 17 which aligns with the age groups most frequently hospitalized for substance-related self-inflicted injuries in our study. The prevalence of self-reported past-year alcohol use in Canada was highest among those aged 25 to 34 years,Footnote 21Footnote 39 which aligns with the peak in substance-related assault injuries among those aged 20 to 29 years and 30 to 39 years we found.
We found that substance-related unintentional injuries increased consistently with age, and that falls, the most frequent external cause of unintentional injuries, also increased with age. This aligns with recent Canadian surveillance that reported that fall injury hospitalizations increase with age and are most frequent among those aged 80 years plus.Footnote 3 Certain psychotropic medications taken alone or with other medications or substances, such as alcohol, are associated with higher risk of falls in older adults.Footnote 11Footnote 40Footnote 41 The side-effects of some of these medications result in drowsiness, dizziness and hypotension, which can increase the risk of falls.Footnote 41 In addition, older adults may have comorbidities and frailties that increase the severity of injury after a fall.Footnote 41
We also found that alcohol was the substance most frequently co-occurring with motor vehicle injury hospitalizations. Impaired driving continues to be one of the leading factors in motor vehicle collisions in Canada, with over 85 000 incidents of police-reported impaired driving reported in 2019.Footnote 42Footnote 43 Males (77%) and young adults aged 20 to 34 years (44%) are most frequently charged with alcohol- and drug-impaired driving;Footnote 43 this may explain the observed peak in unintentional substance-related motor vehicle collision injuries for those aged 20 to 29 years and the higher rates in men than in women.
Since the start of the COVID-19 pandemic, patterns of hospitalizations have changed in Canada, with fewer overall hospitalizations.Footnote 44 Still, the number of substance-related hospitalizations increased by 5% between March and September 2020 compared with the same period in 2019 (n = 76 948 vs. 80 954).Footnote 44 These patterns likely reflect changes in human behaviour as a result of widespread lockdowns to curb the spread of COVID-19.Footnote 45Footnote 46Footnote 47 Because of the impact of the pandemic on hospitalizations during 2020/21, results for this fiscal year should be interpreted with caution.Footnote 47
Limitations
The DAD excludes hospitalization data from Quebec, which accounts for approximately 23% of the Canadian population.Footnote 48 Furthermore, these results only include injuries resulting in acute care hospitalizations, and not deaths or emergency department visits.
Several substance-related ICD-10 codes are categorized under mental and behavioural disorders, and for diagnosis, rely on a categorical approach based on self-reported or clinically observable symptoms.Footnote 49Footnote 50 Substance diagnostic codes are only reported in cases where the substance was a significant contributor in the overall diagnosis or episode of care, which may lead to an underrepresentation in the number of injuries that had a co-occurring substance diagnosis. As a result, there is also potential for under- or over-reporting of substance diagnostic codes, as health care providers may have an implicit bias that would influence whether they consider a substance as significantly contributing towards a patient’s episode of care.
An additional limitation, inherent to administrative data, is the inability to determine temporality between substance and injury diagnostic codes in a single episode of care, which means that causality cannot be assumed. Although our study provides an overview of injury hospitalizations with co-occurring substance use diagnoses, the exact relationship between injuries and substances cannot be interpreted.
Conclusion
Injuries with a co-occurring substance diagnosis have accounted for 12% of total injury hospitalizations over the last 11 years. Our results highlight demographic groups that have higher rates of substance-related injury hospitalizations, and therefore would benefit from targeted prevention efforts. Given the evolving opioid epidemic, continued alcohol use and the increased prevalence of polysubstance use, understanding the relationship between substance consumption and injuries is essential in order to implement public health policy and programs for prevention.
This study is part of a larger project that focusses on substance-related injury hospitalizations prior to and during the COVID-19 pandemic.
Acknowledgements
The authors would like to thank Xiaoquan Yao, André Champagne, Mélanie Varin and Anne-Marie Lowe for their helpful feedback throughout the course of the project.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Authors’ contributions and statement
ST, SRM and WT conceptualized the project and methodology.
ST conducted the analysis and led the writing of the manuscript.
All authors provided feedback on the draft and reviewed and approved the final manuscript.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.