
Reducing the health impact of sexually transmitted and blood-borne infections in Canada by 2030: A pan-Canadian STBBI framework for action

Download the alternative format
(PDF format, 6.2 MB, 25 pages)
Organization: Public Health Agency of Canada
Published: 2018-06-29
Cat.: HP40-214/2018E-PDF
ISBN: 978-0-660-26528-5
Pub.: 180067
Related Topics
- Accelerating our response: Government of Canada five-year action plan on sexually transmitted and blood-borne infections
- In-brief: Accelerating our response: Government of Canada five-year action plan on sexually transmitted and blood-borne infections
- Infographic: Pan-Canadian STBBI framework for action
- Sexual health
- Hepatitis C
- HIV and AIDS
Updated: July 9, 2018
Table of Contents
- Introduction
- Purpose and scope
- State of STBBI in Canada
- An approach to address STBBI in Canada
- Pan-Canadian STBBI framework for action
- Conclusion
- Annex A
- Annex B
- Annex C
- References
Introduction
The term sexually transmitted and blood-borne infection (STBBI) describes an infection that is either sexually transmitted or transmitted through blood. This includes, but is not limited to: human immunodeficiency virus (HIV), hepatitis B (HBV) and C (HCV), chlamydia, gonorrhea, syphilis, and human papilloma virus (HPV).
For many years, people living with HIV and viral hepatitis, people from key populations, Indigenous organizations, health professionals, community-based and other civil society organizations, researchers, activists, and governments have all worked together to address sexually transmitted and blood-borne infections (STBBI) in Canada and internationally. Together, we have strengthened our collective capacity to raise awareness, reduce stigma, modify behaviours, and change social environments that contribute to STBBI transmission and improve the quality of life of those living with, at risk of, or affected by, STBBI.
Scientific research has offered us a better understanding of disease transmission and risk factors and as a result, new tools are available to prevent, diagnose, and treat STBBI, and to provide support to those managing chronic infections. These advances have enabled countless people to live longer and healthier lives.
Despite these advances, STBBI remain a significant health concern in Canada even though they are largely preventable, treatable and in many cases, curable. STBBI levy a significant physical, emotional, social and economic cost to individuals, communities, and society.
Rates of certain STBBI continue to rise in Canada and global momentum to eliminate new infections is building. To this end, Canada has endorsed the United Nations' Sustainable Development Goals, as well as the Joint United Nations Program on HIV/AIDS (UNAIDS) and the World Health Organization's (WHO) global health sector strategies to address HIV, viral hepatitis, and sexually transmitted infections (STI) which call on countries to work towards the elimination of STBBI as a health concern by 2030. Footnote * Endnote 1
To reduce new infection and reinfection, improve health outcomes for people living with or affected by these infections, and contribute to global progress, Canada must focus efforts on prevention, testing, treatment, as well as ongoing care and support. We also need to harness new technologies, leverage opportunities to better integrate prevention and care efforts across the continuum, and better coordinate our efforts.
How the pan-Canadian STBBI framework for action was developed
In 2016 and 2017, the Public Health Agency of Canada (PHAC) released an online survey and held face-to-face meetings about STBBI prevention, testing, care/treatment, and support. This consultation process included people living with HIV and hepatitis, people from key populations, representatives of First Nations, Inuit, and Métis organizations, clinicians and other health professionals, community-based and civil society organizations, researchers, provincial and territorial governments, and representatives of the pharmaceutical industry. In addition to identifying opportunities for action to reduce and control STBBI, special attention was given to engaging and balancing gender and age perspectives among a variety of populations such as: people living with HIV and/or hepatitis and affected communities; Indigenous Peoples; gay and bisexual men; people who use drugs; transgender persons; people with experience in the prison environment; people from countries where HIV or viral hepatitis are endemic; and sex workers.
This information was analyzed and forms the basis of the Pan-Canadian STBBI Framework for Action.
Purpose and scope
Purpose of the pan-Canadian STBBI framework for action
The Pan-Canadian STBBI Framework for Action sets out an overarching and comprehensive approach that will support and contribute to achieving global STBBI targets. The Pan-Canadian STBBI Framework for Action provides a vision, strategic goals, and guiding principles to support cohesive action to address STBBI in Canada across all sectors with an emphasis on four pillars: prevention, testing, initiation of care and treatment, and ongoing care and support.
The Pan-Canadian STBBI Framework for Action also identifies key opportunities for action related to each pillar and acknowledges the foundational support provided by increased surveillance, research, knowledge mobilization, and regular monitoring and evaluation to the success of any policy, program, or intervention to address STBBI.
Scope of the pan-Canadian STBBI framework for action
The Pan-Canadian STBBI Framework for Action provides a roadmap for collaborative and complementary actions to reduce the impact of STBBI in Canada and to contribute to the global efforts to end AIDS, viral hepatitis, and sexually transmitted infections as major health concerns.
State of STBBI in Canada
In Canada, the number of newly diagnosed HIV and HCV infections has remained relatively stable nationally in recent years, though there are variations at the regional level and among specific communities. An estimated 65,000 people were living with HIV in Canada as of the end of 2014, of whom an estimated 20% were unaware of their status.Endnote 2 Gay, bisexual, and other men who have sex with men represented approximately 2.5% of the male population (15 years and older) and yet accounted for almost 50% of those living with HIV infection and more than 50% of new infections in Canada in 2014.Endnote 3 Similarly, Indigenous Peoples represented only 4.3% of the general population, but accounted for 10.8% of new HIV infections in 2014.Endnote 3 Endnote 4 The latest HIV medications have led to better individual and population health outcomes, have almost eliminated the progression of HIV infection, and have prevented onward disease transmission. Today, the life expectancy of people living with HIV is approaching that of the general population.
As of 2011, an estimated 221,000 to 246,000 Canadians had a chronic HCV infection of which an estimated 44% were unaware of their status.Endnote 5 Efforts to address these infections have benefited from advances in prevention, and great strides have been made in the treatment of HCV which has further supported prevention by reducing onward transmission. Recently introduced treatments for HCV are highly effective, with rates of cure generally over 90%. However, this does not reduce the need for prevention interventions.
The numbers of newly diagnosed chlamydia, gonorrhea and syphilis infections have increased consistently since the mid-1990s, despite numerous health interventions designed to prevent, diagnose and treat these infections.Endnote 6 Between 2005 and 2014, there was a 49% increase in the reported rate of chlamydia, a 61% increase in the reported rate of gonorrhea, and a 95% increase in the reported rate of syphilis.Endnote 6
A range of social, epidemiological, and other factors contribute to trends in STBBI rates in Canada. These factors include, but are not limited to:
- Many are unaware of their infection because of the asymptomatic nature of some infections.
- Misperception of risk.
- Lack of holistic, comprehensive, and consistent sexual health education.
- Use of alcohol or drugs.
- Inconsistent or incorrect use of condoms.
- Implementation of more accurate diagnostic tests.
A holistic approach to STBBI prevention, treatment, care and support involves talking about sex and gender openly and without judgement.
An approach to address STBBI in Canada
A shared responsibility
The success of the Pan-Canadian STBBI Framework for Action depends on the commitment of all partners and stakeholders working within their respective roles (Annex A). No one sector or government can reduce the health impact of STBBI alone--it will require collaboration to succeed. It is expected that partners across Canada, in various sectors, can identify how and where they can best contribute to these collective efforts, based on local epidemiology and context. Key partners include (among others) people living with HIV and viral hepatitis, key populations, governments, communities, civil society, academia and research sectors, the private sector, and health and front-line providers.
Key populations disproportionately affected by STBBI:
- People living with HIV or hepatitis C and related conditions
- Indigenous Peoples
- Gay and bisexual men
- People who use drugs
- Transgender persons
- People with experience in the prison environment
- People from countries where HIV, HBV and HCV are endemic
- People engaged in the sale, or the purchase of sex
Note: A sex and gender-based lens should be applied to these populations
An integrated approach
To reduce the health impact of STBBI in Canada, it is critical to deliver the most effective interventions, tailored to the needs of people at greatest risk for infection in communities where STBBI are most concentrated. STBBI share common risk factors, behaviours for transmission, and common transmission routes; as such, an integrated approach to prevention and control is most effective. At the same time, it is recognized that infection-specific approaches are still appropriate in certain circumstances or communities.
The social determinants of health
STBBI do not affect all people equally. Vulnerability to, and resilience against, STBBI are both directly and indirectly influenced by the social determinants of health, including: education, income, employment, gender and gender norms, culture, unstable housing or homelessness, access to health services, and social environments. Individuals who have experienced systemic stigma, exclusion, marginalization, mental health issues and discrimination based on race, immigration status, sexual orientation, gender identity, drug use, or involvement in sex work may also be more vulnerable to STBBI. Canada's colonial history and continued health and social inequities experienced by Indigenous Peoples also contribute to STBBI vulnerability.
The Pan-Canadian STBBI Framework for Action can only be successful and build resilience to prevent the transmission of STBBI if it considers and addresses these contextual factors.
Resilience refers to the process of overcoming the negative effects of risk exposure, coping successfully with traumatic experiences and avoiding the negative trajectories associated with risks.Endnote 7
A focus on key populations
In Canada, it is well understood that STBBI disproportionately affect certain populations. Moreover, individuals within these key populations often experience overlapping epidemics, also known as "syndemics", driven by the impact of determinants of health along with stigma and discrimination.
A syndemic occurs when two or more health issues interact synergistically to contribute to increased health burden for individuals or communitiesEndnote 8.
Pan-Canadian STBBI framework for action
Vision
A Canada where STBBI are rare and people living with STBBI receive the care and support they need.
Desired outcome
To reduce the health impact of STBBI in Canada by 2030.
Strategic goals
The success of the Pan-Canadian STBBI Framework for Action will be measured against global STBBI targets (Annex B). Progress towards these targets will support the following broader strategic goals for Canada:
- Reduce the incidence of STBBI in Canada.
- Improve access to testing, treatment, and ongoing care and support.
- Reduce stigma and discrimination that create vulnerabilities to STBBI.
Guiding principles
The following principles will inform collective action to address STBBI in Canada to reach the strategic goals.
- Meaningful engagement of people living with HIV and viral hepatitis and key populations
- People living with HIV and viral hepatitis and key populations are meaningfully engaged in the development and implementation of policies and programs that affect them.
- Moving towards truth and reconciliation
- Policies and programs to address STBBI among Indigenous Peoples are developed by and with First Nations, Inuit and Métis peoples through a relationship grounded in mutual respect and rooted in an understanding and recognition of and responsiveness to the ongoing impacts of colonization, health and social consequences of residential schools, structural inequities and systemic racism.
- Integrated approach
- Interventions and programs are designed to address the complexity and interrelated nature of risk factors and transmission routes for STBBI while recognizing that disease-specific approaches may be appropriate in some cases.
- Cultural relevance
- Policies and programs to address STBBI reflect and respect cultural realities and practices while ensuring the safety of individuals and communities.
- Human rights
-
All people, regardless of their sexual orientation, race, culture, gender, abilities, or personal practices, are important and their human rights are recognized, respected and promoted.
- Health equity
- All people - regardless of sex, gender, race, income, sexual orientation, geographic location, status, age, or culture - have equitable accessEndnote 9 to quality information and services from qualified health professionals and other front-line providers.
Equitable access is about providing individuals with equal access to appropriate healthcare services based on their perceived need for care. Equitable access considers availability and quality of care.
- Multi-sectoral approach
- Multi-sectoral and multi-disciplinary approaches to prevention and care are embraced to improve collaboration and ensure interventions acknowledge the whole individual and their wellness needs.
- Evidence-based policy and programs
- Interventions and programs are consistently developed with, and guided by, the most recent surveillance data, research and other evidence.
An enabling environment
An enabling environment includes interrelated legal, social, cultural, physical and structural conditions that support successful STBBI programs, policies and actions.
An enabling environment creates the conditions needed to ensure equitable coverage, increase the uptake of services, and improve the quality of health services. An enabling environment can also establish conditions to overcome barriers such as poverty, homelessness, violence, social exclusion, marginalization, criminalization of some behaviours (e.g., drug use, purchase and trade of sex, and non-disclosure of HIV prior to sexual activity), physical setting, discrimination, stigma and inequity, which can have negative consequences for the health and mental health outcomes of people living with, or at risk of, STBBI.
Evidence shows that public policies and access to housing, taxation, immigration, education, employment and income programs have a direct impact on people living with or vulnerable to STBBI.
The extent to which an enabling environment can be established will directly impact the success of actions under all core pillars of the Pan-Canadian STBBI Framework for Action.
Creating an enabling environment: Opportunities for action
- Collect and use data about knowledge, behaviours, attitudes, and experiences related to stigma, discrimination, and barriers to services, to inform evidence-based policies, programs, and interventions.
- Support initiatives to eliminate homophobia, transphobia, racism, sexism, ableism, and other forms of stigma and discrimination associated with STBBI, including those that reduce stigma within the healthcare system, and feature sex and gender-based approaches.
- Review and revise laws, policies, and programs that affect determinants of health leading to an increased risk of STBBI transmission and/or limit the implementation and operation of effective STBBI-related programs and services.
- Support programs that facilitate access to basic needs including safe and affordable housing, income, education, health, employment and other social support services for people living with, at risk of or affected by STBBI and related health issues.
- Support initiatives that improve access to mental health services and harm reduction approaches that prevent or reduce the harms associated with drug use and unprotected sex.
Harm reduction refers to programs, policies, and practices that aim to prevent and control the spread of STBBI. The focus of harm reduction is on preventing or reducing harms associated with drug use and unprotected sex.
Core pillars
The Pan-Canadian STBBI Framework for Action is composed of four interconnected pillars that span the continuum of STBBI care: prevention, testing, initiation of care and treatment, and ongoing care and support. Coordinated action across all pillars will be required to accomplish the goals of the Pan-Canadian STBBI Framework for Action. As specific implementation plans and concrete actions are identified, links between components will be identified and leveraged to effectively achieve the Pan-Canadian STBBI Framework for Action's goals.
The Pan-Canadian STBBI Framework for Action's core pillars are supported by a strong foundation of surveillance, research, knowledge mobilization, and monitoring and evaluation.
Surveillance systems provide key information about the epidemiology of STBBI in Canada. They also help identify key populations and locations where action is needed to reduce the public health impact of STBBI. Surveillance can also contribute to monitoring and evaluation of policies, programs, and interventions.
Research is essential to develop STBBI related policies, programs, and interventions. The development of innovative interventions and treatment methodologies is necessary to reduce the health impact of STBBI.
Knowledge mobilization enhances the integration of information and evidence into programs and policies to prevent and control STBBI. It also supports more effective health services and products to strengthen the healthcare system overall.
Monitoring and evaluation determines progress and identifies gaps or limitations of policies, programs and interventions. All concrete actions identified as part of specific implementation plans must be regularly monitored and evaluated to measure their effectiveness in achieving goals.
Prevention
Programs and policies aimed at increasing knowledge, changing attitudes and behaviours, as well as supporting the uptake of existing and emerging prevention technologies are needed to reduce the number of new infections in Canada. Over the past several decades, our STBBI prevention toolbox has been significantly expanded as a result of scientific discoveries, vaccination programs (e.g., HBV and HPV), harm reduction initiatives, biomedical and technological advancements, as well as increased knowledge of effective interventions.
Comprehensive sexual health education, the consistent and correct use of condoms, vaccinations, and the consistent use of sterile drug equipment are critical to reducing new infections. Innovative biomedical interventions are also key to prevention. For example, antiretrovirals can be used by people living with HIV to maintain an undetectable viral load or by HIV-negative individuals at high risk for infection to lower their risk of becoming infected.
Culturally-appropriate interventions and those that meaningfully involve people living with HIV and viral hepatitis and key populations are necessary to reduce new infections. Furthermore, interventions that capitalize on new communication technologies, such as social media, should be considered.
Strengthening prevention: Opportunities for action:
- Improve access to effective prevention interventions, including safer-sex materials, harm reduction, testing, treatment and targeted vaccination programs.
- Research, implement, and evaluate innovative biomedical prevention interventions (e.g., new vaccines and PrEP) and continue to expand the reach of existing vaccines (e.g., HBV and HPV).
- Develop and disseminate holistic, scientifically accurate, culturally- and age-appropriate, and gender-responsive sexual health information, resources and curricula in school and community settings.
- Implement sustained interventions to facilitate empowerment and behaviour change among individuals who engage in risky behaviours.
- Equip health professionals and front-line providers with knowledge, skills, and resources to provide equitable access to prevention interventions - including the use of treatment to prevent STBBI transmission - vaccination, testing, treatment and contact investigation programs.
Testing
Facilitating early detection through the promotion and availability of testing, particularly for those at high risk, or who have previously been exposed, reinforces prevention. It is also the first stage to link people with treatment, care and support. Testing is critical to reduce the risk of long-term health effects for some STBBI and to prevent onward transmission. Recent scientific and technological advancements have improved early detection and can encourage people to access regular testing.
However, more needs to be done to eliminate barriers to access testing and address the low uptake and frequency of testing. New diagnostic methods, such as point-of-care testing, are now available. New technologies that simplify testing or diversify test settings increase accessibility and may remove discomfort that some individuals have with accessing testing through their primary healthcare provider. It is important to ensure that new and effective testing technologies are available in Canada and can be administered by a broad range of service providers. The development of protocols and guidelines to support the implementation of these technologies is also essential.
There are other factors that prevent individuals from accessing testing, including discomfort with test procedures, embarrassment, fear of a positive result, an absence of privacy or confidentiality, stigma, and a lack of an accessible or convenient location and/or hours of operation. Concerns about potential prosecution of individuals who do not disclose their HIV positive status to sexual partners may also discourage getting tested. Healthcare providers may be deterred from offering testing due to incorrect assumptions about their patient's risk for infection, a heavy case load, a lack of time for counselling, personal discomfort, a lack of confidence, and/or inadequate knowledge of new testing technologies.
Enhancing testing: Opportunities for action
- Provide health professionals and front-line service providers with knowledge, skills, and resources to implement person-centred, culturally-relevant, and integrated testing that respects patient privacy and rights.
- Ensure appropriate linkages to prevention, treatment, and care resources are provided to individuals who have been diagnosed with, or at risk of, a STBBI.
- Research, implement, and evaluate innovative and emerging testing technologies, testing approaches, and sustainable quality assurance systems.
- Improve availability of, and access to, evidence-based testing technologies and approaches in a variety of settings.
- Normalize the offer of STBBI testing among healthcare providers while individual rights to confidentiality, pre- and post- test counselling, and informed consent are respected.
Initiation of care and treatment
Timely engagement in care and treatment is critical to reduce infections and ensure optimal health and well-being of those affected. Early linkage to care and initiation of treatment are associated with increased survival, improved overall health, better quality of life, and a decreased risk of onward transmission. Over the past two decades, STBBI research and treatment advances have been numerous. For example, people are living longer with HIV because of highly effective antiretroviral therapies. These therapies now require fewer pills, have fewer adverse side effects, and can suppress viral loads to very low levels that improve health outcomes and can prevent onward transmission.
Treatments for HCV can cure the infection, are more tolerable, easier to adhere to with shorter courses of treatment and prevent onward transmission. When properly diagnosed, most STI can be treated rapidly and easily. Notwithstanding the individual benefits for people receiving treatment, effective treatment regimens can also help avert avoidable and significant costs to the publicly funded healthcare system in Canada.
Despite these advancements, inequities and gaps in accessing STBBI treatment options persist among jurisdictions. Marginalized individuals or individuals living in rural and remote areas often do not benefit from timely and seamless treatment and care. Lack of coverage for STBBI drugs may also prevent individuals from being treated. Moreover, concerns about confidentiality or privacy, fears of stigma, discrimination, loss of personal relationships and, in some cases, violence and personal and/or cultural beliefs about sexual health and/or treatment options can also affect or delay treatment.
Treating STBBI presents many challenges. The emergence of drug-resistant varieties (e.g., gonorrhea) is a growing challenge to effective treatment. Ongoing monitoring, comprehensive antimicrobial stewardship approaches, and the development of new drugs or other treatment options are required to preserve the effectiveness of current antibiotics and antivirals, and improve treatment outcomes.
Likewise, STBBI treatment challenges exist among people who frequently move between locations and jurisdictions. Working in silos, where different levels of government or different government departments have responsibility to provide care, make it difficult to share patient records, and maintain confidentiality. As a result, individuals may be lost to accessing or maintaining care and treatment. This can be an issue for Indigenous People who may have to travel to access care, for individuals who transition from pediatric to adult care, or for people transitioning to the community from the prison environment.
Ensuring access to care and treatment: Opportunities for action
- Develop holistic, culturally-appropriate, and gender-affirming information and education resources for people to facilitate early treatment.
- Identify and eliminate barriers that impede timely and affordable access to STBBI treatment, care and support.
- Address the health of the whole person by adopting holistic and coordinated approaches, developing multi-disciplinary outreach programs and strengthening electronic patient care systems.
- Provide health professionals and other front-line workers knowledge, skills, and resources to reach and engage people with appropriate and timely treatment.
- Expand the application of health-systems tools, including communications technologies and electronic health records management systems, to improve the quality of treatment care for people with STBBI.
- Enhance laboratory surveillance of drug-resistant STBBI to inform effective treatment, antimicrobial stewardship, and the development of new treatments.
Ongoing care and support
Strengthening support services and enhancing person-centred systems of care are critical for optimal health outcomes for those who live with chronic STBBI (i.e., HIV and HCV) or are at risk of co-infection. Consistent, ongoing, person-centred care and support that is rooted in harm reduction principles can mitigate or prevent the transmission of STBBI, reduce or prevent new infections, re-infections or co-infections, and ultimately provide better quality of life.
People living with STBBI represent different cultures, genders, orientations, and abilities. Services that reflect this diversity must address a range of psychological, emotional, cultural, physical health, and practical needs. Challenges in navigating the health system, lack of information about available services, a mistrust of care providers, and marginalized or criminalized status are barriers to care and support. Healthcare providers who lack information or knowledge about how to access a variety of services will have difficulty providing comprehensive care and support.
Life transitions can also result in service gaps and challenges (e.g., the transition of individuals from one health system to another, from pediatric to adult care, between correctional facilities or community-based care, and through the stages of immigration). Improving the continuum of care could further help individuals adhere to treatment and, in the case of HIV, maintain a suppressed viral load.
Services required by people living with HIV, HCV, or both often extend beyond the mandate of health professionals. Person-centred, holistic, and integrated care that focuses on the needs of the individual have been proven to be best practice. The incorporation of STBBI services into primary care clinics and the development of "wrap-around", interdisciplinary, multi-sectoral care models can also contribute to more effective, comprehensive, and seamless care and support.
Ensuring ongoing care and support: Opportunities for action
- Implement a person-centred approach to care and improve links to health and social support for people living with chronic STBBI.
- Empower people living with chronic STBBI to feel engaged in making health decisions by acknowledging and improving their health literacy and knowledge.
- Develop and implement interventions that retain and re-engage people with chronic STBBI with care and support services.
- Provide health professionals and other front-line providers with knowledge, skills, and resources to serve the diverse needs of their patients and to improve their ability to offer culturally-relevant and gender-affirming continuous care and treatment adherence.
- Develop or expand navigation resources, including electronic health records or peer navigators to improve the access of people affected by STBBI to treatment, ongoing care, referrals, support, and to re-engage in care if necessary.
Conclusion
Informed by people living with HIV and viral hepatitis and people from key populations, the Pan-Canadian STBBI Framework for Action provides a common roadmap to guide actions by Indigenous leadership/communities, civil society, health professionals, professional associations and licensing bodies, the private sector, and all levels of government. The Pan-Canadian STBBI Framework for Action is designed to be flexible in recognition of the variation in STBBI epidemiology across the country. Regular monitoring and ongoing adjustments over time are critical to achieving shared goals. That is why federal, provincial Footnote ‡, and territorial governments are committed to developing indicators and targets for Canada that will permit them to measure their progress and guide their respective priorities for all pillars of the Pan-Canadian STBBI Framework for Action. This will allow Canada to report regularly on its progress in meeting targets for STBBI reduction.
Canada will make significant progress towards reducing the health impact of STBBI by 2030, by focusing on these shared goals, using the principles and pillars of this Pan-Canadian STBBI Framework for Action as a guide, and by working across jurisdictions and diverse sectors, in keeping with their respective responsibilities.
Annex A: Roles and responsibilities in Canada relating to STBBI prevention, testing, treatment, and ongoing care and support
Many stakeholders play a role in the prevention of STBBI in Canada:
Participation in the development and implementation of policies and programs by people living with HIV and viral hepatitis and key populations is critical.
Indigenous Peoples identify health priorities of First Nations, Inuit, and Métis peoples; develop and implement policies, strategies, programs, and services to address these priorities.
Civil society, including community-based and other non-governmental organizations and activists, take action to advance the prevention of STBBI and promotion of health by contributing to research and sharing knowledge of effective programs and services with other actors; delivering prevention, education and awareness initiatives; implementing initiatives to increase access to testing, treatment and ongoing care and support; and advocating for programs and services for affected individuals and communities.
Health professionals provide front-line care; request diagnostic tests; prescribe and dispense treatments; contribute to surveillance and monitoring; educate individuals on healthy living and infection prevention; and implement infection prevention initiatives.
Professional associations and licensing bodies establish standards and certification for their professions, prescribing guidelines, awareness and training of health service providers.
The academic sector undertakes research to better understand STBBI and to discover solutions to prevent, treat and cure infection; educates health professionals; and identifies new innovative approaches to prevention, testing and treatment for STBBI.
Local authorities, including local health authorities, are responsible for providing services or facilities to promote health, including sexual health; delivery of health services, including primary care, acute care (e.g., ambulatory care), home and community care, and mental health and addictions services; and STBBI surveillance.
The promotion and protection of health is an area of shared jurisdiction in Canada.
The role of the provincial and territorial governments includes promoting and protecting health, including sexual health. They are responsible for healthcare settings and the delivery of health and social services; inmates in provincial prisons; establishing policies, guidelines, and standards for healthcare settings; supporting medical education; implementing immunization programs for STBBI; supporting research and academic initiatives; managing laboratory services for STBBI; surveillance of STBBI; approving treatments for STBBI on medical formularies; facilitating community-based interventions; and establishing certification programs for health service providers.
The role of the federal government includes promoting and protecting health, including sexual health, while respecting provincial and territorial areas of jurisdiction. The Government of Canada is responsible for the Pan-Canadian surveillance of STBBI; developing policies and guidelines; delivering and funding healthcare services for federal populations, including First Nations people living on-reserve, Inuit communities south of the 60th parallel, serving members of the Canadian Forces, eligible veterans, inmates in federal penitentiaries and some groups of refugee claimants; supporting awareness and education of federally employed healthcare providers; providing national laboratory reference services and specialized testing; facilitating research and innovation to understand STBBI transmission and to support the development of new diagnostic and treatment tools; regulating the safety and effectiveness of new treatments, diagnostic technologies and prevention tools through the approval of drugs and other health products; facilitating community-based interventions; collaborating with provinces and territories; and, engaging with international partners.
The pharmaceutical industry and private sector support the development of new prevention, diagnostic and treatment technologies - supply drugs for the market - support community action - and provide public and professional education related to these products.
Annex B: Global targets for STBBI
HIV
By 2030:
- Zero new HIV infections
- Zero AIDS-related deaths
- Zero discrimination
By 2020:
- 90% of people living with HIV know their status
- 90% of people living with HIV who know their status are receiving treatment
- 90% of people on treatment have suppressed viral loads
- Fewer than 500,000 new HIV infections
- Elimination of HIV-related discrimination
Hepatitis
By 2030:
- 90% reduction in new cases of chronic viral hepatitis B and C infections
- 65% reduction in hepatitis B and C deaths
- 90% of viral hepatitis B and C infections are diagnosed
- 80% of eligible people receiving hepatitis B and C treatment
By 2020:
- 30% reduction in new cases of chronic viral hepatitis B and C infections
- 10% reduction in hepatitis B and C deaths
- 30% of viral hepatitis B and C infections are diagnosed
- 5 million people receiving hepatitis B treatment, and 3 million people receiving hepatitis C treatment
- Achieve and maintain up-to-date 90% coverage for vaccination of hepatitis B vaccine (3 doses)
Sexually transmitted infections
By 2030:
- 90% reduction of T. pallidum incidence globally
- 90% reduction in N. gonorrheae incidence globally
- 50 or fewer cases of congenital syphilis per 100,000 live births in 80% of countries
- Sustain 90% national coverage and at least 80% in every district (or equivalent administrative unit) in countries with the human papillomavirus vaccine in their national immunization programme
Source:
- World Health Organization. Global Health Sector Strategy on HIV for 2016-2021 - Towards Ending AIDS. [Internet] Geneva: WHO; 2016. Available from: http://apps.who.int/iris/bitstream/10665/246178/1/WHO-HIV-2016.05-eng.pdf?ua=1
- World Health Organization. Global Health Sector Strategy on Sexually Transmitted Infections, 2016-2021. Geneva: WHO; 2016. Available from: http://www.who.int/reproductivehealth/publications/rtis/ghss-stis/en/
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016-2021. Geneva: WHO; 2016. Available from: http://apps.who.int/iris/bitstream/handle/10665/246177/WHO-HIV-2016.06-eng.pdf?sequence=1
Annex C
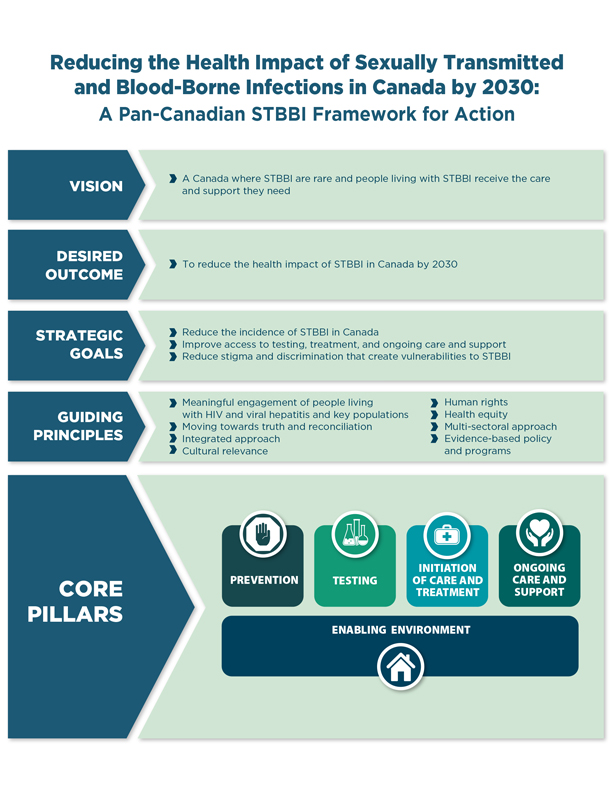
Figure 1 - Text description
The Pan-Canadian Sexually Transmitted and Blood-borne Infections Framework for Action sets out an overarching and comprehensive approach that will support and contribute to achieving global sexually transmitted and blood-borne infection targets.
With the vision of a Canada where sexually transmitted and blood-borne infections are rare and people living with sexually transmitted and blood-borne infections receive the care and support they need, the Pan-Canadian Sexually Transmitted and Blood-borne Infections Framework for Action has the desired outcome to reduce the health impact of sexually transmitted and blood-borne infections in Canada by 2030.
The three goals of the Pan-Canadian Sexually Transmitted and Blood-borne Infections Framework for Action are to:
- Reduce the incidence of sexually transmitted and blood-borne infections in Canada
- Improve access to testing, treatment, and ongoing care and support
- Reduce stigma and discrimination that create vulnerabilities to sexually transmitted and blood-borne infections
The following guiding principles will inform collective action to address sexually transmitted and blood-borne infections in Canada to reach the goals of the Pan-Canadian Sexually Transmitted and Blood-borne Infections Framework for Action.
- Meaningful engagement of people living with HIV and viral hepatitis and key populations
- Moving towards truth and reconciliation
- Integrated approach
- Cultural relevance
- Human rights
- Health equity
- Multi-sectoral approach
- Evidence-based policy and program
The core pillars of the Pan-Canadian Sexually Transmitted and Blood-borne Infections Framework for Action are grouped into four areas which further identify the key opportunities for action that span the continuum of sexually transmitted and blood-borne infection care. The four core pillars include prevention, testing, initiation of care and treatment, and ongoing care and support.
Central to the four core pillars is an enabling environment. Opportunities for action within the enabling environment help to create the conditions to support successful sexually transmitted and blood-borne infection programs, policies, and actions that eliminate stigma and discrimination, and increase uptake, equitable coverage, and quality of health services.
References
- Reference 1
-
World Health Organization. Global Health Sector Strategy on HIV for 2016-2021 - Towards Ending AIDS. [Internet] Geneva: WHO; 2016. Available from: http://apps.who.int/iris/bitstream/10665/246178/1/WHO-HIV-2016.05-eng.pdf?ua=1
- Reference 2
-
Public Health Agency of Canada. Summary: Measuring Canada's progress on the 90-90-90 HIV targets. [Internet] Ottawa (ON): PHAC; 2016. Available from: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/summary-measuring-canada-progress-90-90-90-hiv-targets.html
- Reference 3
-
Public Health Agency of Canada. Summary: Estimates of HIV incidence, prevalence and proportion undiagnosed in Canada, 2014. [Internet] Ottawa (ON): 2015. Available from: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/summary-estimates-hiv-incidence-prevalence-proportion-undiagnosed-canada-2014.html
- Reference 4
-
Statistics Canada. Aboriginal peoples in Canada: First Nations People, Métis and Inuit. Ottawa (ON): Statistics Canada; 2016. http://www12.statcan.gc.ca/nhs-enm/2011/as-sa/99-011-x/99-011-x2011001-eng.cfm
- Reference 5
-
Trubnikov M, Yan P, Archibald C. Estimated prevalence of Hepatitis C Virus infection in Canada, 2011. Can Comm Dis Rep. 2014;40(19): ISSN 1481-8531. Available from: https://www.canada.ca/en/public-health/services/reports-publications/canada-communicable-disease-report-ccdr/monthly-issue/2014-40/ccdr-volume-40-19-december-18-2014/ccdr-volume-40-19-december-18-2014-2.html
- Reference 6
-
Public Health Agency of Canada. Report on sexually transmitted infections in Canada: 2013 – 2014. [Internet] Ottawa: PHAC; 2017. Available from: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/report-sexually-transmitted-infections-canada-2013-14.html
- Reference 7
-
Fergus S, Zimmerman MA. Adolescent resilience: A framework for understanding healthy development in the face of risk. Ann Rev Pub Health. 2005:26;399-419.
Levesque JF, Harris M, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013:12(18). Available from: http://www.equityhealthj.com/content/12/1/18 - Reference 8
-
Merrill S. Introducing Syndemics: A Critical Systems Approach to Public and Community Health. Wiley: Jossey-Bass. 2009(pp. xiv). Available from: https://www.wiley.com/en-us/Introduction+to+Syndemics%3A+A+Critical+Systems+Approach+to+Public+and+Community+Health-p-9780470472033
- Reference 9
-
Levesque JF, Harris M, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013:12(18). Available from: http://www.equityhealthj.com/content/12/1/18
Footnotes
- Footnote 1
-
The World Health Organization defines this concept as the reduction in cases of N. gonorrhoeae and T. pallidum as well as the elimination of congenital syphilis and of pre-cervical cancer lesions through the high coverage of human papillomavirus vaccines.Endnote 1
- Footnote 2
-
The Government of Quebec plans to report to its population on measures it puts in place with regard to the pillars of the Pan-Canadian STBBI Framework for Action.