
Original quantitative research – Psychotic disorder and cannabis use: Canadian hospitalization trends, 2006–2015
Health Promotion and Chronic Disease Prevention in Canada
Bridget Maloney-Hall, MPHAuthor reference footnote 1; Sarah C. Wallingford, PhDAuthor reference footnote 2; Sarah Konefal, PhDAuthor reference footnote 1; Matthew M. Young, PhDAuthor reference footnote 1Author reference footnote 3
https://doi.org/10.24095/hpcdp.40.5/6.06
This article has been peer reviewed.
Correspondence: Matthew Young, 500–75 rue Albert Street, Ottawa, ON K1P 5E7; Tel: 613-235-4048 x 222; Fax: 613-235-8101; Email: myoung@ccsa.ca
Abstract
Introduction: Given the recent and impending changes to the legal status of nonmedical cannabis use in Canada, understanding the effects of cannabis use on the health care system is important for evaluating the impact of policy change. The aim of this study was to examine pre-legalization trends in hospitalizations for mental and behavioural disorders due to the use of cannabis, according to demographic factors and clinical conditions.
Methods: We assessed the total number of inpatient hospitalizations for psychiatric conditions with a primary diagnosis of a mental or behavioural disorder due to cannabis use (ICD-10-CA code F12) from the Hospital Mental Health Database for ten years spanning 2006 to 2015, inclusive. We included hospitalizations from all provinces and territories except Quebec. Rates (per 100 000 persons) and relative proportions of hospitalizations by clinical condition, age group, sex and year are reported.
Results: Between 2006 and 2015, the rate of cannabis-related hospitalizations in Canada doubled. Of special note, however, is that hospitalizations during this time period for those with the clinical condition code “mental and behavioural disorders due to use of cannabinoids, psychotic disorder” (F12.5) tripled, accounting for almost half (48%) of all cannabis-related hospitalizations in 2015.
Conclusion: Further research is required to investigate the reasons for the increase in hospitalizations for cannabis-related psychotic disorder. The introduction of high-potency cannabinoid products and synthetic cannabinoids into the illicit market are considered as possible factors.
Keywords: cannabis, psychotic disorders, hospitalization, Canada
Highlights
- Between 2006 and 2015, the rate of hospitalizations for cannabis-related mental or behavioural disorders in Canada rose from 2.11 to 5.18 per 100 000.
- Males consistently accounted for over two-thirds of all hospitalizations for cannabis-related mental or behavioural disorders.
- Young people aged 15 to 24 years represented the greatest proportion of hospitalizations (between 49% and 58%) of any age group.
- Over the entire study period, psychotic disorder was the most common clinical condition among hospitalizations for cannabis-related mental or behavioural disorders, and accounted for 48.0% of cannabis-related hospitalizations in 2015.
- Between 2006 and 2015, the rate of hospitalizations due to cannabis-related psychotic disorder tripled, from 0.80 to 2.49 per 100 000.
Introduction
Cannabis is a psychoactive substance widely used in Canada, with 14.8% of Canadians aged 15 years and older reporting past-year use in 2017,Footnote 1 which is comparable to the 2014 estimate of 13.2% for past-year use in the United States among Americans aged 12 years and older.Footnote 2 Past-year prevalence of use in Canada was higher among males (18.7%) than females (11.1%) and also among young people aged 15 to 24 (26.9%) compared to adults aged 25 and older (12.7%).Footnote 1
Although there is evidence for moderate therapeutic effectiveness of cannabis in the treatment of some health conditions (e.g. chronic pain, chemotherapy-induced nausea and vomiting, multiple sclerosis spasticity symptoms),Footnote 3Footnote 4Footnote 5Footnote 6Footnote 7 there is little evidence to suggest that cannabis can be beneficial for mental disorders and symptoms.Footnote 8 Moreover, cannabis use, particularly frequent use over periods of months or years, has been associated with increased risk for health harms, including psychosis,Footnote 9Footnote 10Footnote 11Footnote 12Footnote 13 negative respiratory symptoms,Footnote 12Footnote 14Footnote 15 motor vehicle collisionsFootnote 9Footnote 12Footnote 16Footnote 17Footnote 18 and adverse effects on adolescent brain development.Footnote 12Footnote 19Footnote 20
A recent study of the costs associated with substance use in Canada found that in 2014 over $208 million was spent in cannabis-related health care costs, including over $38 million for inpatient hospitalizations.Footnote 21 Moreover, cannabis-related health care costs have been increasing in Canada. The costs of all cannabis-attributable inpatient hospitalizations increased by 22% between 2007 and 2014,Footnote 22 with the cost of inpatient hospitalizations for mental and behavioural disorders due to cannabis use increasing by 52% between 2006 and 2011.Footnote 23 As of now, there is limited research exploring the specific contribution of different mental and behavioural disorders to these observed increases in cannabis-attributable hospitalizations. This study evaluated trends in hospitalization rates between 2006 and 2015 for mental and behavioural disorders attributable to cannabis by age and sex and examined the number and proportions of these hospitalizations according to the type of clinical condition.
Methods
Data sources
Data for this analysis were acquired from the Canadian Institute for Health Information (CIHI). Specifically, data on inpatient separations (herein referred to as hospitalizations) for those with a primary diagnosis of mental and behavioural disorders due to use of cannabinoids (herein referred to as cannabis) were extracted from the Hospital Mental Health Database (HMHDB) for the ten fiscal years spanning April 2006 to March 2016 (herein referred to as 2006 to 2015). The HMHDB is a comprehensive pan-Canadian administrative database capturing demographic and clinical information on patient hospitalizations for psychiatric conditions from both general acute care and specialized psychiatric hospitals. CIHI compiles data for the HMHDB from four sources: the Discharge Abstract Database (DAD), the Hospital Morbidity Database (HMDB), the Ontario Mental Health Reporting System (OMHRS) and the Hospital Mental Health Survey (HMHS).Footnote 24
Measures
Hospitalizations
We defined a hospitalization as a departure from an inpatient hospital, due to discharge or death, where the patient had a primary diagnosis of a mental or behavioural disorder due to use of cannabis. These specific diagnoses were identified using the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada (ICD-10-CA), and diagnoses are determined from a patient’s medical record. Given the nature of these data, it was possible for an individual to have more than one hospital stay recorded in a given year. We included hospitalizations from all provinces and territories except Quebec. At the time of this study, data from Quebec were not available. Hospitalizations recorded in OMHRS were coded using the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), rather than the ICD-10-CA coding system, and therefore were excluded from this analysis. In any given year, a large proportion (57.3%–74.0%) of cannabis-related hospitalizations in Ontario were excluded due to being recorded in the OMHRS and coded with the DSM-IV-TR. The remainder of hospitalizations were recorded in the DAD, HMBD or HMHS and used ICD-10-CA codes. On average, 63% of Ontario hospitalizations were excluded, meaning that a total of 1252 hospitalizations were included and 2088 hospitalizations were excluded for Ontario between 2006 and 2015.
Clinical conditions
According to ICD-10-CA, there are 10 clinical condition codes (F12.0–F12.9) used to describe the type of mental and behavioural disorder due to use of cannabis that constitutes a patient’s primary reason for hospitalization. These conditions include: acute intoxication (F12.0), harmful use (F12.1), dependence syndrome (F12.2), withdrawal state (F12.3), withdrawal state with delirium (F12.4), psychotic disorder (F12.5), amnesic syndrome (F12.6), residual and late-onset psychotic disorder (F12.7), other mental and behavioural disorders (F12.8), and unspecified mental and behavioural disorder (F12.9). Full descriptions of these conditions are available from the World Health Organization.Footnote 25 It is important to note that none of these codes includes any information abouttype (plant based, extract or synthetic) or quantity of cannabis used, the route of administration (inhaled or ingested) or the reason for use (medical or nonmedical).
Age group
Counts of cannabis-related hospitalizations were categorized according to the age groups 0 to 14 years, 15 to 24 years, 25 to 44 years, 45 to 65 years and 65+ years.
Sex
Counts of cannabis-related hospitalizations were grouped by sex (male and female). Hospitalizations for which the patient’s sex was not recorded as male or female were excluded.
Analytic strategy
To examine trends in cannabis-related hospitalizations in Canada over the ten fiscal years from 2006 to 2015, we analyzed the count, proportion and sex- and age-specific rates of cannabis-related hospitalizations by year and clinical condition. Where applicable, we expressed relative proportions by clinical condition in relation to the total volume of hospitalizations for mental and behavioural disorders due to use of cannabis. We calculated the overall crude rate for the Canadian population and sex- and age-specific rates using annual population estimates derived by Statistics Canada using the mid-calendar population estimate.Footnote 26
In accordance with CIHI’s privacy policy, at the time they provided the aggregate data requested for this analysis, some small cells were suppressed for confidentiality. This included cells with single digits (i.e. 1–9 were indicated by “§”) as well as cells with multiple digits (i.e. 10–19 were indicated by “1§”). For the purposes of this analysis, we replaced any suppressed digits with “1” in order to estimate hospitalizations for these cells (i.e. a cell indicated by “§” was replaced with “1”, and a cell indicated by “1§” was replaced with “11”).
Results
Between 2006 and 2015, the number and crude rate of hospitalizations associated with mental or behavioural disorders due to cannabis use in Canada rose from 525 (2.11 per 100 000) in 2006 to 1430 (5.18 per 100 000) in 2015 (Table 1; Figure 1).
Table 1. Number and proportion (%) of hospitalizations for cannabis-related mental or behavioural disorders by demographic characteristics, Canada (excluding Quebec), 2006–2015
| Category | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall | 525 | 615 | 661 | 618 | 779 | 911 | 952 | 1085 | 1243 | 1430 |
| Sex | ||||||||||
|
369 (70.3) | 455 (74.0) | 469 (71.0) | 464 (75.1) | 583 (74.8) | 708 (77.7) | 726 (76.3) | 810 (74.7) | 893 (71.8) | 1026 (71.7) |
|
156 (29.7) | 160 (26.0) | 192 (29.0) | 154 (24.9) | 196 (25.2) | 203 (22.3) | 226 (23.7) | 275 (25.3) | 350 (28.2) | 404 (28.3) |
| Age | ||||||||||
|
21Footnote a of Table 1 (4.0) | 20 (3.3) | 30 (4.5) | 19 (3.1) | 21 (2.7) | 28 (3.1) | 31Footnote a of Table 1 (3.3) | 22 (2.0) | 30 (2.4) | 41 (2.9) |
|
272 (51.8) | 302 (49.1) | 353 (53.4) | 341 (55.2) | 428 (54.9) | 486 (53.3) | 503 (52.8) | 627 (57.8) | 691 (55.6) | 746 (52.2) |
|
178 (33.9) | 229 (37.2) | 211Footnote a of Table 1 (31.9) | 215 (34.8) | 251Footnote a of Table 1 (32.2) | 304 (33.4) | 317 (33.3) | 351 (32.4) | 408 (32.8) | 494 (34.5) |
|
54 (10.3) | 61Footnote a of Table 1 (9.9) | 56 (8.5) | 43 (7.0) | 68 (8.7) | 86 (9.4) | 96 (10.1) | 78 (7.2) | 106 (8.5) | 136 (9.5) |
|
1Footnote a of Table 1 (0.2) | 1Footnote a of Table 1 (0.2) | 1Footnote a of Table 1 (0.2) | 0 (0.0) | 1Footnote a of Table 1 (0.1) | 7 (0.8) | 1Footnote a of Table 1 (0.1) | 7 (0.6) | 8 (0.6) | 13 (0.9) |
Figure 1. Rate of hospitalizations for cannabis-related mental or behavioural disorder (per 100 000) in Canada (excluding Quebec), 2006–2015

Text description: Figure 1
Figure 1. Rate of hospitalizations for cannabis-related mental or behavioural disorder (per 100 000) in Canada (excluding Quebec), 2006–2015
| Year | Rate per 100 000 |
|---|---|
| 2006 | 2.11 |
| 2007 | 2.44 |
| 2008 | 2.59 |
| 2009 | 2.40 |
| 2010 | 2.99 |
| 2011 | 3.46 |
| 2012 | 3.57 |
| 2013 | 4.02 |
| 2014 | 4.55 |
| 2015 | 5.18 |
Across all years examined, males consistently accounted for at least 70% of all cannabis-related hospitalizations and young people aged 15 to 24 years represented the greatest proportion of hospitalizations (between 49% and 58%) of any age group (Table 1).
Examination of sex- and age-specific rates for cannabis-related hospitalizations showed a 19-fold increase in hospitalization rates between 2006 and 2015 among those aged 15 to 24 years (Table 2). We also observed large increases in hospitalization rates among individuals aged 25 to 44 and individuals aged 45 to 64. Increases of 2.5-fold from 2006 to 2015 were reported for both males and females.
Table 2. Rates of hospitalizations for cannabis-related mental or behavioural disorders (per 100 000) by demographic characteristics, Canada (excluding Quebec), 2006–2015
| Category | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall | 2.11 | 2.44 | 2.59 | 2.40 | 2.99 | 3.46 | 3.57 | 4.02 | 4.55 | 5.18 |
| Sex | ||||||||||
|
2.98 | 3.64 | 3.71 | 3.63 | 4.51 | 5.43 | 5.49 | 6.05 | 6.59 | 7.50 |
|
1.24 | 1.26 | 1.49 | 1.18 | 1.49 | 1.53 | 1.68 | 2.02 | 2.54 | 2.90 |
| Age | ||||||||||
|
0.48Footnote a of Table 2 | 0.46 | 0.68 | 0.43 | 0.48 | 0.64 | 0.70Footnote a of Table 2 | 0.50 | 0.67 | 0.92 |
|
1.09 | 8.61 | 10.02 | 9.63 | 12.02 | 13.59 | 13.97 | 17.37 | 19.14 | 20.82 |
|
0.71 | 3.18 | 2.93Footnote a of Table 2 | 2.99 | 3.49Footnote a of Table 2 | 4.21 | 4.35 | 4.76 | 5.47 | 6.57 |
|
0.22 | 0.90Footnote a of Table 2 | 0.80 | 0.60 | 0.93 | 1.15 | 1.28 | 1.03 | 1.39 | 1.77 |
|
0.00Footnote a of Table 2 | 0.03Footnote a of Table 2 | 0.03Footnote a of Table 2 | 0.00 | 0.03Footnote a of Table 2 | 0.19 | 0.03Footnote a of Table 2 | 0.17 | 0.19 | 0.30 |
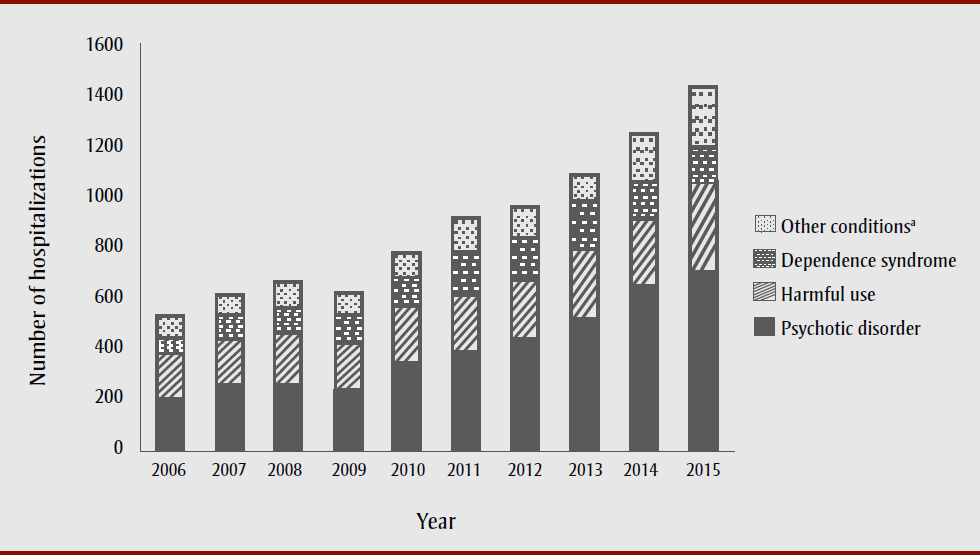
In an attempt to understand which clinical conditions might be associated with this increase, we assessed the distribution of clinical conditions for each year. In 2006, the two most common clinical conditions for cannabis-related hospitalizations—psychotic disorder and harmful use—accounted for similar proportions of hospitalizations, at 37.9% and 33.9%, respectively. However, by the end of the study period, the proportion of hospitalizations due to cannabis-related psychotic disorder was nearly double that of hospitalizations due to harmful use of cannabis, at 48.0% and 26.0%, respectively. Throughout the course of the study, cannabis-related psychotic disorder was the most common clinical condition seen in cannabis-related hospitalizations (Figure 2). Indeed, between 2006 and 2015, the rate of hospitalizations due to cannabis-related psychotic disorder tripled, from 0.80 to 2.49 per 100 000 (data not shown).
Figure 2. Number of hospitalizations for cannabis-related mental or behavioural disorders in Canada (excluding Quebec) by clinical condition, 2006–2015
Text description: Figure 2
Figure 2. Number of hospitalizations for cannabis-related mental or behavioural disorders in Canada (excluding Quebec) by clinical condition, 2006–2015
| Year | Number of Hospitalizations | |||
|---|---|---|---|---|
| Psychotic disorder | Harmful use | Dependence Syndrome | Other ConditionsFigure 2 footnote a | |
| 2006 | 199 (38.3%) | 178 (34.2%) | 70 (13.5%) | 73 (14.0%) |
| 2007 | 241 (39.4%) | 203 (33.2%) | 84 (13.7%) | 83 (13.6%) |
| 2008 | 249 (37.8%) | 211 (32.1%) | 101 (15.3%) | 97 (14.7%) |
| 2009 | 230 (37.5%) | 194 (31.6%) | 105 (17.1%) | 84 (13.7%) |
| 2010 | 332 (42.8%) | 232 (29.9%) | 119 (15.3%) | 93 (12.0%) |
| 2011 | 382 (42.1%) | 230 (25.3%) | 164 (18.1%) | 132 (14.5) |
| 2012 | 420 (42.2%) | 237 (24.9%) | 178 (18.7%) | 115 (12.1%) |
| 2013 | 508 (46.9%) | 284 (26.2%) | 183 (16.9%) | 109 (10.1%) |
| 2014 | 629 (50.6%) | 287 (23.1%) | 132 (10.6%) | 195 (15.7%) |
| 2015 | 687 (48.1%) | 372 (26.0%) | 124 (8.7%) | 246 (17.2%) |
Discussion
The overall rate of cannabis-related hospitalizations increased between 2006 and 2015, with the largest increase occurring in those hospitalizations with the clinical condition code “mental and behavioural disorders due to use of cannabinoids, psychotic disorder.” These results could be due to increased prevalence of cannabis use. However, as there is little evidence for increased prevalence of cannabis use across our period of analysis, particularly among youth and young adults, we suggest that a central explanation for our results is the increasing potency of cannabis and the introduction of synthetic cannabinoids into the illicit drug market. Further, changes in the way that hospitalization data is collected and coded, as well as changes in attitudes toward reporting cannabis use, may also contribute to the observed increases in psychiatric hospitalizations.
The link between cannabis use and psychosis and schizophrenia
The link between cannabis use and the risk for developing schizophrenia is an important consideration for understanding why the largest proportions of cannabis-related hospitalizations are due to psychotic disorders. A key symptom of schizophrenia is psychosis, and a first episode of psychosis can be an initial diagnostic feature of schizophrenia, especially among those with a family history of mental disorders. Although cannabis use is significantly higher among individuals with schizophrenia,Footnote 27Footnote 28 there is substantial evidence that cannabis use, especially frequent use over longer periods of time, increases the risk of developing both psychosis and schizophrenia.Footnote 29Footnote 30Footnote 31Footnote 32Footnote 33 The risk of psychosis also increases with the frequency of cannabis use in a dose-dependent mannerFootnote 30Footnote 31Footnote 34Footnote 35Footnote 36Footnote 37 and with increasing percentage of delta-9 tetrahydrocannabinol (THC) in the product consumed.Footnote 34Footnote 35Footnote 36 Early initiation of cannabis use, especially during adolescence, also elevates the risk for developing psychotic disorders, including schizophrenia.Footnote 38Footnote 39Footnote 40Footnote 41 Molecular genetic research demonstrates that another key factor influencing the degree of risk conferred by cannabis use for developing schizophrenia or psychosis is having a family history of these disorders.Footnote 37Footnote 42Footnote 43Footnote 44Footnote 45Footnote 46 Although it has been reported that some genetic risk factors underlie both the risk for developing schizophrenia and for initiating cannabis use,Footnote 47Footnote 48 cannabis use on its own is still an independent risk factor for psychosis and related mental disorders such as schizophrenia.
Increasing THC content in cannabis products available in the illicit market
Data from Statistics Canada show a relatively stable age of initiation among youth between 2004 and 2015,Footnote 49Footnote 50Footnote 51 and that the prevalence of cannabis use actually decreased among those under the age of 25.Footnote 52 During this same period, however, there is evidence of increased availability of high potency cannabis extractsFootnote 53 and the introduction of potent synthetic cannabinoidsFootnote 53Footnote 54Footnote 55Footnote 56 into the global illicit market.
Globally, the average proportion of THC, the main psychoactive component responsible for the “high” feeling associated with cannabis consumption, in herbal cannabis has risen over the last 50 to 60 years.Footnote 53Footnote 57 While in the 1960s the proportion of THC in herbal cannabis averaged around 3%, in the early 21st century, countries have seen average proportions of THC in the range of 12% to 20%.Footnote 53 In addition to the increase in proportion of THC in herbal cannabis, new high-THC products referred to as “extracts” (e.g. “shatter” or “butane honey oil”) have been found with THC concentrations of 80%Footnote 53 to 99%.Footnote 58
Given that the use of higher potency cannabis products is associated with an increased risk of adverse health outcomes,Footnote 25Footnote 36Footnote 53 it is possible that the increasing availability of high potency cannabis products, including herbal cannabis with higher THC potency as well as cannabis extracts, may be contributing to the increasing rate of cannabis-related hospitalizations in Canada, particularly those associated with psychotic disorder.
It will be prudent to evaluate these trends from 2016 onward to the era of legalized nonmedical cannabis, and to continue to monitor them, since cannabis extracts became legal in Canada in October 2019. In addition, investments in public education and harm reduction strategies are needed to prevent hospitalizations due to cannabis use. For example, this could include increasing the awareness and implementation of the lower-risk cannabis use guidelines, which mention choosing products with lower THC content, among other recommendations, to reduce the risk of adverse health effects from cannabis.Footnote 59 The data presented here also highlight the need for comprehensive and integrated mental health and addiction services, especially for youth and young adults (i.e. aged 15–24) in order to better address the overlap between cannabis use and mental and behavioural outcomes.
Synthetic cannabinoids
Synthetic cannabinoids are a large and diverse family of compounds that, like THC, bind to cannabinoid receptors in the body, but are typically more potent and toxic.Footnote 60 Documented adverse health effects of synthetic cannabinoids include cardiovascular problems (e.g. hypertension, chest pain, tachycardia) and psychiatric issues (e.g. psychosis, anxiety, withdrawal), among others.Footnote 60 The first identification of a synthetic cannabinoid in the illicit drug supply can be traced to 2008.Footnote 55 Though there is limited Canadian epidemiological data on the use of synthetic cannabinoids, we do know that they have been used in Canada since at least 2009.Footnote 54 The 2017 Ontario Student Drug Use and Health Survey indicated that 1.5% of students in Grades 7 to 12, encompassing the ages of 12 through 18, reported using synthetic cannabis in the past year, and that this estimate had remained stable since the survey first asked about synthetic cannabinoid use in 2013.Footnote 56 Between April 2018 and April 2019, synthetic cannabinoids were found in 0.2% of samples analyzed by Health Canada’s Drug Analysis Service.Footnote 61 Therefore, in addition to the availability and use of higher potency cannabis products, it is also possible that the rise in cannabis-related hospitalizations may be linked to the appearance of synthetic cannabinoids in the illicit drug marketplace.
Strengths and limitations
By furthering our understanding of the clinical conditions responsible for the observed increase in cannabis-related hospitalizations, we will be in a better position to provide prevention, treatment and harm reduction strategies for those who use cannabis. Given the period of study, this analysis further provides a snapshot of hospitalization trends before legalization of nonmedical cannabis in Canada, and can be a useful benchmark to compare with post-legalization follow-up analyses.
The dataset that we analyzed only included the total number of hospitalizations and not the total number of people who were hospitalized. Therefore, we are unable to comment on the proportions of hospitalizations that may be due to a person being hospitalized multiple times throughout a fiscal year, and which conditions are associated with multiple hospitalizations. This should be an important consideration for future studies, given that 12.1% of patients hospitalized for mental illness had at least three hospital stays in 2017/18.Footnote 62
The dataset we used for this study was also limited as to the scope of demographic factors analyzed that could be associated with cannabis-related hospitalizations for psychiatric conditions. In addition to age and sex, important factors to consider for future studies include socioeconomic status (income and education), geography (urban vs. rural), ethnicity and the use of other substances.
The ICD-10-CA coding system used by the databases we accessed contains a great deal of detail, but there are limitations. The classification codes for mental and behavioural disorders due to use of cannabinoids do not distinguish between those admitted to hospital for disorders associated with herbal cannabis versus synthetic cannabinoids, or whether the individual admitted was using a cannabis product for medical or nonmedical purposes. Therefore, the results cannot be linked with the prevalence of use of different types of cannabis products. In addition, we cannot account for differences in clinical practice settings that may influence the ICD-10 code applied to a particular diagnosis. For example, the perceptions of health care practitioners or their awareness of cannabis as a contributor to some psychological symptoms may have changed over time, perhaps due to increased public and political dialogue concerning cannabis legalization. The changing political landscape of cannabis throughout our period of study may also have influenced the likelihood that patients would disclose their cannabis use.
The results presented here are likely to be an underestimate of the true number of cannabis-related hospitalizations for several reasons. These data do not include inpatient hospitalizations for which a cannabis-related disorder was a secondary diagnosis. They also do not include hospitalizations for which a primary diagnosis code of “mental and behavioural disorders due to multiple drug use and use of other psychoactive substances” was given, of which some cases may be attributable to cannabis use. Further, Quebec and Ontario were not comprehensively included in the study. When investigating the clinical conditions associated with each hospital stay, only hospitalizations coded with the ICD-10-CA coding system were used, thus omitting a large proportion of cannabis-related hospitalizations in Ontario. As noted in the Methods section, approximately 63% of hospitalizations in Ontario were therefore excluded from this study’s analysis. Data from Quebec, a province that accounts for close to a quarter of the Canadian population, were not available for this analysis. Finally, we applied conservative estimation procedures for dealing with suppressed data cells, since these were assumed to have a value of 1, despite the actual value ranging between 0 and 9 due to secondary data suppression.
Conclusion
The increasing rate of hospitalizations due to cannabis-related psychotic disorder in Canada between 2006 and 2015 is a trend that warrants further investigation, in light of both what is known regarding the association between frequent cannabis use and psychosis and the recent legalization of nonmedical cannabis use in Canada. Further research is required to clarify the cause of these increased harms, particularly among those with the highest rate of cannabis-related hospitalizations (younger individuals and males), in order to better target public education efforts around lower-risk use and prevention of cannabis-related harms. Ongoing monitoring of cannabis use and related harms, including high potency cannabis products such as cannabis extracts and synthetic cannabinoids, will also be essential to understanding the impact of legislative change on these trends in the future.
Acknowledgements
The authors extend their thanks to Dr. Diana Ridgeway and Mr. Harry Kang for their assistance in the preparation of this manuscript. This work is made possible through a financial contribution from Health Canada.
Conflicts of interest
The authors have no conflicts of interest to declare.
Authors’ contributions and statement
All four authors, BMH, SCW, SK and MMY, contributed to each stage of developing the manuscript. This includes the research design, acquisition of data, analysis of data, drafting and revising of the paper, and approval of the final manuscript.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.