
Original mixed methods research – Experiences, impacts and service needs of injured and ill workers in the WSIB process: evidence from Thunder Bay and District (Ontario, Canada)

HPCDP Journal Home

Published by: The Public Health Agency of Canada
Date published: July 2022
ISSN: 2368-738X
Submit a manuscript
About HPCDP
Browse
Previous | Table of Contents | Next
Chelsea Noël, BSc, GradDipAuthor reference footnote 1; Deborah Scharf, PhD, CPsychAuthor reference footnote 1Author reference footnote 2; Joshua Hawkins, BA, GradDipAuthor reference footnote 1; Jessie Lund, MAAuthor reference footnote 1; Jewel Kozik, HBScAuthor reference footnote 3; Anna Péfoyo Koné, PhDAuthor reference footnote 2
https://doi.org/10.24095/hpcdp.42.7.02
This article has been peer reviewed.
Author references
Correspondence
Deborah Scharf, Braun Building, BB-1007E, 955 Oliver Road, Thunder Bay, ON P7B 5E1; Tel: 807-343-8773; Email: dscharf1@lakeheadu.ca
Suggested citation
Noël C, Scharf D, Hawkins J, Lund J, Kozik J, Péfoyo Koné A. Experiences, impacts and service needs of injured and ill workers in the WSIB process: evidence from Thunder Bay and District (Ontario, Canada). Health Promot Chronic Dis Prev Can. 2022;42(7):272-87. https://doi.org/10.24095/hpcdp.42.7.02
Abstract
Introduction: Individuals experience negative physical, social and psychological ramifications when they are hurt or become ill at work. Ontario’s Workplace Safety and Insurance Board (WSIB) is intended to mitigate these effects, yet the WSIB process can be difficult. Supports for injured workers can be fragmented and scarce, especially in underserved areas. We describe the experiences and mental health needs of injured and ill Northwestern Ontario workers in the WSIB process, in order to promote system improvements.
Methods: Community-recruited injured and ill workers (n= 40) from Thunder Bay and District completed an online survey about their mental health, social service and legal system needs while involved with WSIB. Additional Northwestern Ontario injured and ill workers (n = 16) and community service providers experienced with WSIB processes (n = 8) completed interviews addressing similar themes.
Results: Northwestern Ontario workers described the impacts of workplace injury and illness on their professional, family, financial and social functioning, and on their physical and mental health. Many also reported incremental negative impacts of the WSIB processes themselves, including regional issues such as “small town” privacy concerns and the cost burden of travel required by the WSIB, especially during COVID-19. Workers and service providers suggested streamlining and explicating WSIB processes, increasing WSIB continuity of care, and region-specific actions such as improving access to regional support services through arm’s-length navigators.
Conclusion: Northwestern Ontario workers experienced negative effects from workplace injuries and illness and the WSIB process itself. Stakeholders can use these findings to improve processes and outcomes for injured and ill workers, with special considerations for the North.
Keywords: occupational injuries, occupational stress, mental health, rural health services, workers’ compensation, WSIB
Highlights
- Individuals in Northwestern Ontario who were hurt or became ill at work experienced negative effects on their physical, financial, social and psychological well-being, including some related to or worsened by the WSIB process. This is consistent with research conducted elsewhere in the province.
- Injured and ill workers in Northwestern Ontario may face additional regional barriers to proper care and recovery, including limited employment opportunities, “small town” privacy concerns and the costs and burden of care-related travel, especially during public health crises such as the COVID-19 pandemic.
- Suggestions to improve the WSIB process provided by Northwestern Ontario injured workers and service providers included general system improvements (e.g. streamlining and explicating WSIB processes, increasing WSIB continuity of care, designating an arm’s-length system navigator), and several suggestions particular to the northern context.
Introduction
When individuals get hurt or become ill at work (henceforth “injured workers”), they encounter a cascade of negative effects on their physical, financial, social and psychological well-being.Footnote 1Footnote 2Footnote 3 Ontario’s Workplace Safety and Insurance Board (WSIB), formerly known as the Workers’ Compensation Board, is intended to help. First introduced in 1914, the Worker’s Compensation Board provided compensation to injured workers in the form of wage replacement and health care benefits, regardless of fault, in order to reduce adversarial relations between workers and employers when workplace injury or illness occurred.Footnote 4 The current WSIB, having undergone several substantial changes over time, is now an independent trust agency responsible for balancing interests of employers and injured workers.Footnote 5 The WSIB describes its function as collecting appropriate premiums from employers in order to provide timely and fair compensation to individuals who are hurt or become ill at work, while supporting their recovery and return to work.Footnote 5
Although most WSIB claims are adjudicated quickly and smoothly, and most injured workers return to work with minimal disruptions to life and career,Footnote 6 evidence suggests that approximately 20% of claims are prolonged, complicated and litigious, accounting for approximately 80% of total compensation claim costs.Footnote 3 Furthermore, when the WSIB denies a worker’s claim and the worker files an appeal, they may be without income and necessary health and social supports for years while the appeal is resolved. Such situations inevitably lead to catastrophic consequences to workers and their families.Footnote 1Footnote 7 Examples of such situations are frequently profiled in the media,Footnote 8Footnote 9 illustrating the vulnerability of injured workers and the power that the WSIB system has to support or deny workers in need.
Recourse pathways and resources for people wanting to appeal WSIB decisions are fragmented and scarce. In Ontario, specialized, Toronto-based, community legal clinics assist injured workers across the province. Smaller, satellite community legal clinics also exist in other locations, but many of those clinics, including the ones in Northwestern Ontario, are not fully staffed; frequently they do not employ a lawyer at all, and often do not have the resources to provide assistance in workers’ compensation matters. Moreover, while the Ministry of Labour’s Office of the Worker Adviser provides no-cost representation to non-unionized injured workers, their waiting list is years long, leaving people without the financial means to pay for legal assistance, and without recourse. Altogether, individuals who become engaged in the WSIB claims and appeals processes frequently experience a toll on their finances, families and mental health.Footnote 7
The risk of developing or exacerbating psychological illness during the WSIB claims and appeals process is high. Recent data suggest that up to half of individuals who get hurt or become ill at work develop depressive symptoms within a year of injury.Footnote 10Footnote 11 Such emergent mental health conditions further impede workers’ long-term recovery and potential to return to work.Footnote 12Footnote 13 Many workers also lose the ability to access mental health services and supports once they become injured or ill because they lose access to employer insurance and the income needed to pay for mental health services. In Ontario, waitlists for free, public mental health services are often six months or more.Footnote 14
In northern, rural or remote areas of Ontario, at least two additional challenges may further impede recovery and return to work. These include a general lengthening of the WSIB process, as workers frequently must travel to access specialists for assessments to justify receipt of WSIB benefits, and difficulties in accessing appropriate care once benefits are in place. For example, with just 11 WSIB-registered psychologists in Thunder Bay City and DistrictFootnote 15 (a region geographically larger than countries such as Germany and Spain), workers with benefits may have to wait months to begin receiving services and then travel several hours by car or plane to receive care when in-person services are required.
In order to improve the services and outcomes for injured workers in Northwestern Ontario, WSIB, policymakers and community stakeholders need research that describes workers’ needs throughout the WSIB claims and appeals processes, predictors of worker WSIB experiences and the available supports in the region. The WSIB, policymakers and community stakeholders particularly need research that describes the mental health and social service needs of injured workers engaged in the WSIB process in northern, rural and remote areas such as Thunder Bay City and District, in order to identify service gaps and quality issues, and to inform future system improvements in this high-needs, underserved region. Thus, our study describes Northwestern Ontario injured workers’ experiences with the WSIB process and its impacts, plus system factors affecting WSIB experience, and suggestions to improve it.
Methods
Study design and participants
This study included a convergent, parallel, mixed methods design,Footnote 16 including a quantitative online survey (n = 40 injured workers) and semistructured qualitative interviews with n = 16 injured workers and n = 8 service providers experienced with WSIB processes in Thunder Bay City and District (Ontario). Lakehead University’s Research Ethics Board approved the study procedures (reference no. 1467879).
Eligibility criteria
Eligible injured workers (1) were at least 18 years of age; (2) were able to read and write in English; (3) were residents of Thunder Bay City or District; (4) were previously injured at work or ill from work; and (5) had filed a WSIB claim or were involved with the WSIB compensation process (including appeals) within the past five years. Injured workers elected to participate in either the online survey or semistructured interview.
Eligible service providers (1) were at least 18 years of age; (2) had the ability to read and write in English; and (3) had provided services to at least eight injured and ill workers in Thunder Bay City and District in the past two years.
Recruitment
Our team recruited injured workers through social (e.g. Facebook, Kijiji, Reddit) and print (e.g. local newspapers, hardcopy flyers) media. We recruited service providers through (1) emails to listservs and service organizations; (2) professional networks; and (3) snowball sampling, with the intention of interviewing service providers from diverse service (legal, social and psychological) backgrounds.
Instruments
We designed and used three separate data collection tools for the study, including separate tools for workers and service providers. Our worker survey instrument was primarily designed to collect quantitative information, and both interview guides were designed to collect exclusively qualitative information.
Online survey and worker interview guide
We developed online survey and worker interview guides that included questions about (1) demographics; (2) workers’ injuries or illnesses; (3) workers’ experiences engaging in the WSIB claims (and separately) appeals processes; (4) workers’ use of any community or supplementary services during the claims and appeals processes (e.g. food bank, or legal or community mental health services); and (5) workers’ suggestions for improving the WSIB claims and appeals processes. Workers also reported their perceived impacts of the WSIB claims (and separately) appeals processes. In the online survey, workers responded to the question, “How stressful was the claims (or appeals) process?” on a 5-point Likert scale from “not at all” to “extremely” stressful.
Service provider interview guide
Service providers were asked about similar topics, but from their point of view. Service providers reported (1) personal demographics and professional experience with injured workers; (2) perceived impacts of WSIB claims and appeals process on workers; (3) experience supporting workers engaged in the appeals process; (4) workers’ use of supplementary services while in the WSIB claims or appeals processes; (5) challenges supporting workers in the WSIB claims and appeals processes; and (6) suggestions for improving the WSIB claims and appeals processes.
All data collection tools are available by request.
Data collection
We collected data between November 2020 and March 2021. We collected data from both sources (survey and interview) concurrently.
Online survey
Upon confirmation of eligibility and written informed consent, research assistants sent participants an email with a link to the online survey, hosted on the SurveyMonkey platform. The survey included 70 questions and took participants approximately 14 minutes to complete.
Qualitative interviews
Clinical psychology graduate students (JH, JL, CN), trained and under the supervision of a registered clinical psychologist (DS), interviewed injured and ill workers and service providers experienced with WSIB processes via Zoom or telephone (respondent’s choice). Because we collected data during the COVID-19 pandemic, we did not offer participants the option of in-person interviews. During each interview, interviewers reiterated the purpose of the study, collected verbal informed consent and posed questions to guide discussion. Interviewers encouraged participants to elaborate, specify and discuss their experiences. Interviews were audio recorded and transcribed.
Data analysis
We analyzed qualitative and quantitative data separately, using different but complementary approaches.
Quantitative analysis
Our team used descriptive statistics to characterize the sample, including workers’ injuries, needs, experiences and associated health and social service use. We also ran very preliminary, exploratory, univariate general linear models to suggest factors that might be associated with workers’ self-reported stress (on a 5-point Likert scale) separately during the claims and appeals processes. Due to our small sample size, we limited these analyses to a short list of demographic and injury-related factors derived from the literature and authors’ clinical experiences. These factors included participants’ age, sex, employment industry when injured (agriculture, manufacturing, transportation and warehousing; construction and mining; education, health care and social assistance; emergency services; hospitality, retail, arts, entertainment and recreation; and other industries), and permanence of disability (permanent, not sure, no permanent disability). All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Qualitative analysis
We (DS, CN, JH, JL) conducted a thematic content analysis,Footnote 17Footnote 18 first by reviewing transcripts and extracting relevant themes related to workers’ experiences and needs, and then by identifying convergent and divergent issues using a mixed analysis grid.Footnote 18 More specifically, we developed an initial coding framework for deductive analyses based on the preliminary themes used to organize the interview guide (experiences with and impacts of the WSIB process, system factors affecting WSIB experience, and suggestions to improve it). As there is a dearth of research related to injured worker experiences with workers’ compensation in rural, remote and northern communities in Ontario and in Canada overall, we kept themes in the initial coding framework minimal and broad, allowing for maximal generation of new themes and categories reflecting injured workers’ experiences.Footnote 19 Accordingly, we also conducted an inductive analysis to identify emergent themes and categories, which resulted in many new emergent themes (i.e. WSIB-specific risk factors vs. broader system risk factors affecting WSIB experience, varying suggestions to improve the process) and categories (e.g. various WSIB claim impacts) that we included in the final categorization.
To do this, we first familiarized ourselves with the data collected through the online surveys and qualitative interviews. Second, we summarized data into smaller fragments of information that were first descriptive (paraphrases), then interpretative (words representative of underlying concepts, called “codes,” selected by coders). We then grouped codes that reflected similar meaning under categories, and we grouped categories into themes within the coding framework.Footnote 18 We analyzed data continuously until saturation was reached (i.e. no new themes emerged). We finalized the coding framework, scheme and final categorization using co-coding and discussion, and we resolved disagreements through consensus.
Results
Participants
Injured worker characteristics are shown in Table 1. Injured workers were largely between 35 and 54 years of age, male, not legally married (i.e. single or common-law) and with no dependents. Participants largely identified as White. Nearly all participants were born in Canada, lived in Thunder Bay, Ontario, and spoke English as their first language. Gender and ethnicity were representative of the worker demographics of the region, but, in comparison, our sample was slightly older than other workers in the region.Footnote 20
| Characteristic | Survey (n = 40) | Interview (n = 16) |
|---|---|---|
| n (%) | n (%) | |
| Age (years) | ||
| 18–34 | 11 (27.5) | Footnote * |
| 35–54 | 20 (50.0) | 7 (43.8) |
| 55+ | 9 (22.5) | 5 (31.2) |
| Sex | ||
| Female | 17 (42.5) | 7 (43.8) |
| Male | 23 (57.5) | 9 (56.2) |
| Marital status | ||
| Legally married | 15 (37.5) | 8 (50.0) |
| Not legally married | 25 (62.5) | 8 (50.0) |
| Ethnicity | ||
| White | 34 (85.0) | 12 (75.0) |
| Other | 6 (15.0) | Footnote * |
| Number of dependents | ||
| 0 | 19 (47.5) | 8 (50.0) |
| 1 | 7 (17.5) | 5 (31.3) |
| 2 | 9 (22.5) | Footnote * |
| 3+ | 5 (12.5) | Footnote * |
| City of origin | ||
| Thunder Bay | 38 (95.0) | 15 (93.8) |
| Other | Footnote * | Footnote * |
|
||
Service providers (n = 8) were mostly female, with an average of M = 12.9 (SD = 14.25) years’ experience providing services to injured workers. Providers practised in the areas of mental health, legal and physical rehabilitation services and described their geographic practice areas as including Kenora, Thunder Bay, all of Northwestern Ontario, or all of Ontario including the North.
Workplace injuries, disability and need for accommodation
Injured workers described their workplace injuries, the presence of disabilities and their needs for accommodation through the online survey and semistructured interviews.
Survey
The majority (n = 28; 70%) of survey respondents’ injuries occurred in the past five years. Respondents’ injuries were largely physical (n = 32; 80%) as opposed to psychological or occupational disease. Respondents made claims while working in the following sectors: education, health care and social assistance (n = 8; 20%); agriculture, manufacturing, transportation and warehousing (n = 10; 25%); hospitality, retail, arts, entertainment and recreation (n = 8; 20%); construction and mining (n = 6; 15%); emergency services (n = 5; 12.5%) and “other” (redacted due to small cell size).
Half (n = 20; 50%) of survey respondents stated that they were working either full time (n = 15; 75%) or part time (n = 5; 25%) since filing a WSIB claim. Among respondents who stated that they were currently working (n = 20), 40% (n = 8) stated that they had accommodations in place including modified tasks, a modified workspace, reduced hours, delayed return to work and changes in their role. The majority (n = 25; 62.5%) of respondents stated that the workplace injury changed their life “a lot” or “completely.” Nearly half (n = 19; 47.5%) of all respondents reported sustaining a permanent disability from their workplace injury.
Interviews
The majority (n = 12; 75%) of interviewees’ injuries also occurred in the past five years. This means that a quarter of interviewees’ injuries occurred more than five years ago, yet they were still engaged in the WSIB process at the time of their interview. Their injuries were mostly physical (n = 12; 75%), with many fewer psychological and occupational diseases (n = 4; 25%). Injured worker interviewees also largely made claims while working in the education, health care and social assistance industries (n = 8; 50%). Other (n = 8; 50%) interviewees made claims while working in construction and mining, agriculture, manufacturing, transportation and warehousing and emergency services (% redacted due to small cell sizes). Fewer than half of all worker interviewees reported that they were working full time at the time of the interview (n = 7; 43.8%).
Experience and impacts of the WSIB claims and appeals processes
Injured workers and service providers described the experiences and impacts of the WSIB claims and appeals processes on injured workers through the online survey and semistructured interviews.
Survey
Although most (n = 32; 80.0%) respondents reported that their original claim was accepted, the majority of these still rated the claims process as “extremely” (n = 13; 32.5%) or “very” (n = 9; 22.5%) stressful. Similarly, among the nearly half of all respondents (n = 18; 45.0%) who reported appealing a WSIB claim, less than half of those appeals (n = 8; 44.4%) were accepted, and nearly one-quarter (n = 4; 22.2%) were still in progress. Nearly all respondents described the appeals process as “extremely” (n = 10; 55.6%) or “very” (n = 4; 22.2%) stressful. Respondents who filed claims only, or both claims and appeals, described the processes as having negative impacts on their psychological health, physical health, relationship with their family, relationship with their friends, hobbies, community involvement, financial security and career (Figure 1).
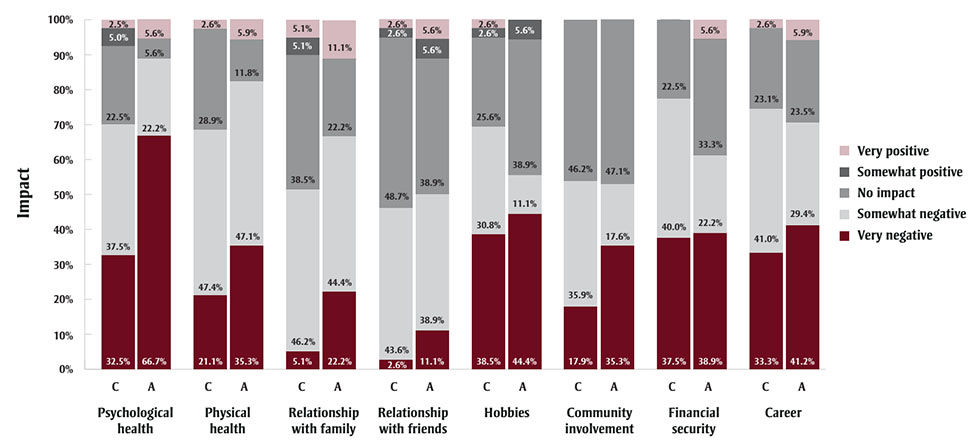
Figure 1 - Text description
| Process | Domain of impact | Very negative | Somewhat negative | No impact | Somewhat positive | Very positive |
|---|---|---|---|---|---|---|
| C | Psychological health | 32.5% | 37.5% | 22.5% | 5.0% | 2.5% |
| A | 66.7% | 22.2% | 5.6% | 0.0% | 5.6% | |
| C | Physical health | 21.1% | 47.4% | 28.9% | 0.0% | 2.6% |
| A | 35.3% | 47.1% | 11.8% | 0.0% | 5.9% | |
| C | Relationship with your family | 5.1% | 46.2% | 38.5% | 5.1% | 5.1% |
| A | 22.2% | 44.4% | 22.2% | 0.0% | 11.1% | |
| C | Relationship with your friends | 2.6% | 43.6% | 48.7% | 2.6% | 2.6% |
| A | 11.1% | 38.9% | 38.9% | 5.6% | 5.6% | |
| C | Hobbies | 38.5% | 30.8% | 25.6% | 2.6% | 2.6% |
| A | 44.4% | 11.1% | 38.9% | 5.6% | 0.0% | |
| C | Community involvement | 17.9% | 35.9% | 46.2% | 0.0% | 0.0% |
| A | 35.3% | 17.6% | 47.1% | 0.0% | 0.0% | |
| C | Financial security | 37.5% | 40.0% | 22.5% | 0.0% | 0.0% |
| A | 38.9% | 22.2% | 33.3% | 0.0% | 5.6% | |
| C | Career | 33.3% | 41.0% | 23.1% | 0.0% | 2.6% |
| A | 41.2% | 29.4% | 23.5% | 0.0% | 5.9% |
Abbreviations: A, frequencies related to
the appeals process; C, frequencies related to the claims process.
Note: Percentages (%) represent the frequency of
responses for n = 40 injured workers who reported on their
experiences filing a claim, and a subset of n = 18 injured workers
who appealed the decision of a claim.
With full recognition of our small sample size (n = 40 survey respondents), we conducted very preliminary univariate linear regression analyses designed to identify worker and injury characteristics potentially associated with elevated levels of claim- and appeal-related stress, largely as potential suggestions for future research. Our univariate predictors included age, gender, injury type, industry and disability permanence, and our outcome was self-reported claim-related stress, measured on a 5-point Likert scale. Workers’ mean self-reported claim-related stress was 3.4 (SD = 1.5), and their mean self-reported appeal-related stress was 4.1 (SD = 1.3). Only presence of a permanent disability was found to be associated with claim stress (RFootnote 2 = 0.17, F2,47 = 3.78, p = 0.03). Specifically, workers reporting a permanent disability (Β = 1.49, p = 0.01) experienced significantly more claim-related stress than workers with no permanent disability (reference group). None of the variables that we examined were significantly associated with appeal-related stress.
Interviews
We used Northwestern Ontario injured worker and service provider interviews to describe the ways in which the WSIB claims and appeals processes affected workers’ mental health. Worker and service provider responses fit within nine common themes: (1) family role instability and conflict (e.g. partners and children transitioning to wage-earning roles; loss of respect or authority of injured worker with reduced ability to provide for others); (2) financial anxiety and insecurity (e.g. worries about the onset, duration and extent of WSIB wage replacement); (3) frustration and anger (e.g. about WSIB paperwork requirements, difficulty accessing case representatives and having the validity of their claims constantly questioned); (4) helplessness and hopelessness (e.g. processes were slow, requests for support to promote return to work were delayed or denied); (5) job insecurity (e.g. unavailability of pre-injury job after recovery or appropriate accommodated or alternate work); (6) loss of professional or occupational identity (e.g. disappointment about inability to work in the field that they were trained for and where they had careers); (7) retraumatization (e.g. needing to recount traumatic details of the workplace injury to multiple WSIB workers and reassert the validity of the claim); (8) guilt and shame (e.g. about not being able to work and support families); and (9) social isolation (e.g. separation from coworkers, self-isolation from friends and loved ones associated with workplace injury–related depression). Illustrative quotations may be found in Table 2.
| Theme | Sample quotation |
|---|---|
| Family role instability and conflict | “WSIB has caused a lot of issues, like, I’m upset more, so it’s affecting my relationship with my wife.” – IW 9 “I’ve seen marriages end because of what’s happened to the individual that’s been injured. Their life just spirals out of control and so you can see how that impacts relationships, how it impacts marriages, like I said, people have lost their homes. I don’t have to spend a lot of time with the injured workers group to see the significant changes that have happened, even to the ones that don’t have a brain injury. I have [seen] other kinds of injuries, and how [workers have] been impacted by those work-related injuries, and how it impacts their lives for the rest of their lives.” – SP 5 |
| Financial anxiety/insecurity | “I’m a single mom, my kids live with me full time, I’m 100% responsible for them, and I’m getting calls about my vehicle being repossessed. And then I can’t make my mortgage payments. And, you know, all these things that add to already, like you’re already mentally not coping well.” – IW 4 “I try not to think about my own case too much because it just gets me pissed off. It hasn’t been good by any means, because [I] pretty much lost everything. I’m going from making 100 and something thousand dollars a year to I don’t even know now. It’s not a lot. I had to sell my house. Sell my camp. Like, I’m not poor, but I am definitely not well off, and I was.” – IW 3 “Often pride comes in, and they don’t want to access the social assistance benefits, which often they have to, they’re forced into, because otherwise they have no income. We see people selling off their assets, which are very important in our area. So boats, snow machines, trailers, all those things. Part of it as qualifiers for social assistance, is that they’re forced into selling these things. And part of it is that they’re, they’re accessing money so that they can live.” – SP 2 |
| Frustration/anger | “Every time you call WSIB, it ignites like, an anger inside of me.” – IW 13 “Having somebody call you and call you and call you, and then send you letters and call you some more and then ask for updates and then want to talk to your doctors, want to take notes, and it’s different people every time, is infuriating.” – IW 10 |
| Helplessness/ hopelessness | “You get into the process and if you don’t have any help, you are overwhelmed, it is just set up … to make people give up.” – IW 3 “If it’s an appeals process, then it’s sort of got an adversarial component to it, which I think increases that sense of feeling under threat, right, and then so that’s just exacerbating any feelings of hopelessness or helplessness.” – SP 1 |
| Job insecurity | “From the mental health side of it, [following my physical injury] even though I had a really hard time keeping up with their production, I was still required to do it, or [face] the threat of job loss. So that became a real issue, mentally … and that’s how the two are intertwined. From a physical to mental health.” – IW 11 |
| Loss of professional or occupational identity | “[My workplace] just sang the praises, like whenever they needed somebody, I worked with all the very difficult cases. I gave them 110% all the time. And then when I became an injured worker when I was injured there, well then I became a nothing.” – IW 5 “They’re not able to work towards their career goals. It is just human nature, right, to want to aspire to something and to further. And I actually feel like it’s a shame because that’s an effect of the trauma that’s actually unnecessary. Once they’re well enough, psychologically, they should be supported, to be able to have gainful, meaningful work without any kind of financial costs, if we’re really true to the spirit of WSIB.” – SP 4 |
| Retraumatization | “And then going through the process and retelling your story to everyone you meet with, which is also, like, very retriggering going over things and over things. And you get to the point where you’re telling them and trying to get your point across and make them not only understand, but believe you, because you’ve said it so many times and obviously, when you’re repeating it for the 10th time, you’re just, like, okay, so obviously the last couple people didn’t believe me.” – IW 4 |
| Shame/guilt | “All those feelings of shame that go with it—I’m, you know, I’m normally this strong, confident woman and I can’t do the things I normally would do. And it has such a compounding effect on your whole life.” – IW 4 “You feel guilty that you’re incapable of doing the one thing that you wanted to do.” – IW 10 |
| Social isolation | “It took a huge toll on my mental health. It took a long time for me to admit that. I’m a very strong, stubborn person. And so it was my husband first that realized that I wasn’t going out anymore. I’m very, very active person, you know, hiking, canoeing, hunting everything outside, I was staying in a lot more.” – IW 1 “And so of course, that affects them socially. Because then they don’t have these things to go and do. And they lose their friends and connections that were associated with it. They also have no money to go out and hang out with people. So they become isolated.” – SP 2 “They start to become socially isolated from their own friends and family because they physically can’t do things, you know, they can’t pick up a coffee mug. When you’re in chronic pain you’re just very down and just give up. Right?” – SP 4 |
Abbreviations: IW, injured/ill worker; SP, service provider; WSIB, Workplace Safety and Insurance Board. |
|
System factors impacting workers’ WSIB experiences
Injured workers and service providers also described system factors impacting workers’ experiences with the WSIB through the online survey and semistructured interviews.
Survey
Respondents selected (from a list) aspects of the WSIB process that went smoothly and those that were challenging, separately, during the claims (n = 40) and appeals (n = 18) processes (Figure 2).

Figure 2 - Text description
| Component | Claims process was challenging | Claims process went smoothly | Appeals process was challenging | Appeals process went smoothly |
|---|---|---|---|---|
| Going through process while still injured/ill | 45.0% | 17.5% | 72.2% | 0.0% |
| Finances while off work | 55.0% | 15.0% | 44.4% | 5.6% |
| Interactions with coworkers | 12.5% | 25.0% | 11.1% | 22.2% |
| Interactions with employers | 22.5% | 15.0% | 27.8% | 11.1% |
| Attending meetings/appointments | 30.0% | 12.5% | 33.3% | 22.2% |
| Scheduling meetings/appointments | 15.0% | 27.5% | 5.6% | 33.3% |
| Medical expert assessment/consultation | 47.5% | 37.5% | 38.9% | 27.8% |
| Communication with employers | 42.5% | 20.0% | 27.8% | 11.1% |
| Communication with WSIB | 72.5% | 20.0% | 77.8% | 0.0% |
| Paperwork | 55.0% | 7.5% | 50.0% | 5.6% |
Abbreviation: WSIB, Workplace Safety and
Insurance Board.
Note: Percentages (%) represent the frequency of
responses for n = 40 injured workers who reported on their
experiences filing a claim, and a subset of n = 18 injured workers
who appealed the decision of a claim.
Injured workers identified some aspects of the claims and appeals processes that went smoothly (n = 34; 85.0%), including medical expert assessment and consultation (n = 15 [37.5%] for claims and n = 5 [27.8%] for appeals, respectively), interactions with coworkers (claims: n = 10 [25.0%]; appeals data redacted due to small cell size) and scheduling meetings and appointments (n = 11 [27.5%] and n = 6 [33.3%], respectively).
All participating workers chose to identify challenges during the claims process. These included communication with WSIB (n = 29; 72.5%), paperwork (n = 22; 55.0%), finances while off of work (n = 22; 55.0%), medical expert assessment/consultation (n = 19; 47.5%) and going through the application process while still injured/ill (n = 18; 45.0%). Findings were similar for the appeals process. Respondents reported encountering challenges related to communication with WSIB (n = 14; 77.8%), paperwork (n = 9; 50.0%), medical expert assessment and consultation (n = 7; 38.9%) and going through the application process while still injured/ill (n = 13; 72.2%) during the appeals process. More information about the nature of these challenges came from worker interviews (see next section).
Workers were also asked if they had accessed non-WSIB community supports during the WSIB claims and appeals processes. Some (n = 16; 40.0%) workers reported accessing support services in the process of making claims or appeals, including psychological and legal services, chronic pain programs, employment services, injured worker groups, employee assistance programs, foodbanks, crisis lines, transportation services, income supplement services and the Office of the Worker Adviser (n’s and percentages redacted due to small cell sizes). Among workers (n = 16) who accessed support services, the majority (n = 14; 87.5%) described them as “very” or “extremely” helpful.
Interviews
Northwestern Ontario workers and service providers described system factors that positively and negatively impacted their WSIB claims and appeals experiences, including both WSIB-specific and broader system factors. Corresponding sample quotations for themes and categories are shown in Table 3.
| Theme | Category | Sample quotation |
|---|---|---|
Protective factors |
Access to adequate services (e.g. psychological) |
“I was lucky that my psychologist still continued to do just pro bono check-ins with me. I would say the [most helpful] thing has been, like, my nurse practitioner and my psychologist.” – IW 4 “I will give credit for the fact that they did have funding in place for the psychology component. I will be, I can’t, I can’t thank them enough for that.” – IW 12 |
Introduction of online portal |
“I really enjoyed that when I utilized their online service to submit a question. It allows you to input what time is the best time to call you at. I think that’s great, because I work three jobs. So sometimes it’s nice for me to be able to put in, don’t call me until after five, like, I’m at work, like, I can’t answer the phone. [Also], I think that having things like that in writing is also really beneficial. Because, like, coming from a union perspective … being able to submit that and have a copy of that, and then a copy of a response that if anything was to ever happen.” – IW 10 “Well, definitely the electronic portion of their, their claims submission now, as has been changed, you know, before, like I say, you could only mail your stuff, or fax it to them. So now, now they’ve established, you know, electronic reporting. And also, you know, now they have a secure email format. They never have, they never had that before. And even one of the first times I talked to that colleague, I said, you know, rather than me phoning you, or you phoning me, because we did sort of play phone tag there for a little bit. And back in May, I says, you know, would be nice if, you know, I could just send you an email and wouldn’t be this …. And so she says, oh, yeah, well, we’re working on that. And she says, we need to make, make it secure. And probably back in April, I asked her that. And then eventually, they did, you know, develop that system. So that was very, very good.” – IW 16 |
|
WSIB transparency |
“I did find the return-to-work specialist from WSIB. I mean, she was, I found her great. She was very helpful. Um, like, insightful, gave you information and things like that.” – IW 4 |
|
WSIB system-specific risk factors |
Care coordination and treatment planning |
“A lot of [service providers] don’t understand WSIB and a lot of them you don’t want to deal with WSIB because WSIB for the doctors in some cases [have] big broad goals.” – IW 7 “I had one worker tell me when I wasn’t ready to go back to work yet, because I haven’t even gone to see my specialist, he said that you’re going to be cut off if you just don’t get back to work right now. So I felt very bullied to go back to work when I wasn’t ready to, which made the situation worse.” – IW 1 “I haven’t talked to [a neurologist or my family doctor yet], but [the WSIB] already set a plan up. And so I’m like wait a sec. How can you be making all these decisions without talking to the medical field?” – IW 9 |
Communication |
“It’s always the same process. You call there, you wait in the queue, you talk to customer service, they transfer you to your case manager, she doesn’t answer, you leave a voicemail, she never calls back, then you have to call again the next day, the next day, the day after, and go through the whole process again. And then ask to speak with the manager and find out why your case manager is not calling you back in what in the timeframe they tell you that they’re supposed to.” – IW 13 “I would say most of it’s communication. I think most workers, even those with allowed claims really, really struggle to get a person on the phone, to be honest, um and I don’t want to denigrate or speak ill of the case managers because they’re union members too, they’re part of CUPE and they’re so overworked.” – SP 4 |
|
Paperwork |
“I don’t know how people can keep up with some of the stuff like the paper[work] comes, the mail. And a lot of time, it’s like having a third job and you’ll watch your binders get thicker and thicker over the year. And you [have] to keep up with it because if you don’t keep up with it, at the end of the day, you’re going to pay for it. You have to be proactive yourself to actually make the system work. If you don’t do your job, at the end of the day, you’re gonna get screwed.” – IW 7 “It’s up to you to prove to them that you need these services, and that you need these things to happen. And there was months where, like, I felt like it honestly, to a certain degree, it’s been like a full time job, sort of staying on top of this, making the phone calls, following up with things, making notes, like, I have, like, this notebook, and it’s, like, all tabs. And this is my, like my Bible.” – IW 4 “[If] the person has a brain injury, cognitive impairments, information processing difficulties, memory problems, they’ll get this piece of mail, or they may not understand what [the WSIB is] asking, and then the [injured worker doesn’t] think to get help to fill out this form, or it ends up in the junk drawer or falls behind the fridge and the Board [will] come after them for noncompliance because they didn’t [complete] some form, and they don’t stop to think about how hard it is for this injured worker, if they have issues with fatigue, or if they’ve got cognitive fugue or had a seizure, and now their memory is that much more compromised, and it takes them a couple of weeks to get back up to speed again, and something shows up during that period of time. And [if] they’re not complying then they get cut off [WSIB benefits].” – SP 5 |
|
Staff turnover and continuity of care |
“I’m gonna be honest with you, it was never the same person that I spoke to. In that particular one, it every time somebody called me it was somebody else, it was almost like they were overwhelmed, which I can understand. And they, I just, my case was passed off, I would say I talked to about six different people. And nobody actually knew, like, what my injury was. So every time somebody would call me, I’d have to redo the whole story with them, and then go about whatever they called me about in the first place. Which is frustrating because you, it puts you in a position where not necessarily that someone doesn’t care, because it’s not really necessarily their job to care, but they don’t know who I am. It’s their job to make sure that I get the supports that I need.” – IW 10 “The other thing is, is that what the WSIB will do is they will switch their case managers or their nurse consultants quite frequently. So if somebody’s been on their roster for, you know, a long time, and they want to move them, they start changing their either case manager and nurse consultant, every, say, I don’t, don’t quote me on this, but, like, every three months, or something, or every six, six months, and so to be somebody with a fresh pair of eyes, but also somebody who doesn’t have the context of having read through their whole file.” – SP 1 |
|
Transparency |
“The biggest thing was just knowing partially, like, what your rates are, but also what’s out there for WSIB to offer you. Because they’re not really forthcoming and saying, we can do this, this and this for you, they’re only going to give you that if you go to say a doctor, a specialist, who knows what they can offer who, you know, writes that note, and then pushes you into that program. But yeah, it’s hard to know how to navigate and what WSIB should and shouldn’t be doing. Because you’re just following kind of what that what WSIB is telling you." – IW 13 “You’re going in blind, potentially, like you don’t know, all of a sudden you got hurt and you can’t work and you don’t know what that looks like, you know what I mean? So that adds to the stress of everything else. And then now you have WSIB calling you every day. And you don’t understand what their purpose is. There is no information on that.” – IW 10 “The WSIB doesn’t educate its clinicians on their processes, which would help us to educate our clients because the clients are kind of in the dark ... which feeds into the sense of uncertainty and lack of safety, which again, inhibits their psychological progress, right?” – SP 1 |
|
Broader system: risk factors |
Access/location issues |
“It was incredibly frustrating, because there’s only so much that I can do when you live in a northern city that only has so many health care providers. So, if you have to go to the fracture clinic, if you have to go to a chiropractor, if you have to go to physical therapy, like, those things take time. They’re not just you called me yesterday, and now you’re calling today. Nothing has changed, like, in an 18-hour timespan.” – IW 10 “There’s a lot of times for these services that I’ve been receiving anyways, you need a referral. And so if you can’t get in to see your own doctor to request that referral, while you’re on your own, you know, I’ve been trying to read a lot and try to educate myself and try to, you know, learn about myself as to what I’m dealing with. And it’s been an experience in that sense all by itself.” – IW 16 “[When] I had to go and explain my pre-existing condition, and that my specialist was in Toronto, that’s when it became very complicated. Realizing that there would be a lot of travel expenses back and forth from Toronto, hotel stays, lots of time off work, and things like that. They, they became very rude, very quick.” – IW 1 “Yeah, like, it was very aggressive, like, very aggressive. And they made me go back to the emergency room four times to get more paperwork from the same doctor, because my family doctor wasn’t good enough.” – IW 10 “The big thing that I find that I didn’t hit enough is that how different it is in the North, and, meaning, like me, disconnected, Kenora north, not very north, from sort of the urban Toronto-centric access to services, that, you know, it’s always important to explain the difference and how, you know, services are different, the people are different, accessing. So WSIB is always different like that.” – SP 2 |
Access to medical experts for assessment/consultation/ service |
“It would be nice if the government had [medical experts], especially in Northern Ontario, you don’t really have much open over there. In Toronto and Ottawa, places like that, I’m sure you could find someone just walking outside your building, like, some, somebody that knows the rules. But Northern Ontario, a lot of people are on their own. It’s an older generation and younger generation. You know [service providers], don’t really want to deal with WSIB, I’m sure you have a couple labour lawyers that are involved in that stuff.” – IW 7 “Something happens, they’ll deny your claim because there’s no, the big word is continuity, with WSIB. They want to see the MRIs, they want to see the doctors appointments. They want to hear the transcripts from the doctors and most people won’t do that because they don’t have the time, especially if they have a family.” – IW 7 |
|
Employer and union relations |
“I ended up getting let go [from] my job, like, within two weeks of [calling the labour board to notify them about my unsafe workplace], or I suspect it was reprisal because I called the labour board and all this kind of stuff. So I more or less was like, on top of being injured … Just kind of didn’t help anything.” – IW 6 “Unfortunately, I wasn’t able to access anything legal, because my agency is unionized, so I did have a union rep helping me out at first but was told via private emails that the agency basically bullied her off my case, because they said that if she continues supporting me that she would be fired and so I didn’t, I don’t really have any help with them, either. Because they, they don’t have anyone representing me.” – IW 1 “What was worse was having my workplace come in to Workers’ Comp and say that I must have been faking it, or that I wasn’t worthy of a meaningful re-education, that they didn’t want to be liable for it. Having my workplace not back me up, that was bad.” – IW 8 |
|
Going through the process while still injured/ill |
“Every day when I do talk to someone, I have to make notes because I also, my memory is not what it used to be, so I don’t retain information the same and so I have to do that. And there was huge periods of time where mentally I wasn’t able to advocate for myself. And luckily, I have great family and friends supports that sort of helped pull me through and, like, my children of course. But I sort of, I look at it like if I hadn’t had those, you know, where would where would I be right now?” – IW 4 “I don’t have the mental capacity anymore to try and remember when things have to be in, how things get organized, this group I’m working with, [I’ve] got all kinds of people helping me out with organizing and stuff like that and my wife just doesn’t have the time because she’s driving me to doctors’ appointments.” – IW 3 |
|
Abbreviations: IW, injured/ill worker; SP, service provider; WSIB, Workplace Safety and Insurance Board. |
||
Protective (i.e. positive or experience-enhancing) factors identified by workers were: (1) access to adequate services (e.g. psychological); (2) the recent introduction of a WSIB online portal to coordinate and file claims and appeals; and (3) WSIB transparency (i.e. instances in which workers knew exactly what to expect from WSIB and what procedures to follow).
Risk factors (i.e. negative or factors that detract from the experience) specific to WSIB identified by workers included: (1) care coordination and treatment planning issues (e.g. accessing and aligning services between providers); (2) communication challenges (e.g. difficulty getting in touch with WSIB representatives); (3) paperwork (total amount, complex nature); (4) staff turnover and continuity of care (e.g. having to repeat basic injury/illness information to multiple new workers); and (5) transparency (e.g. uncertainty about process steps and requirements). Worker-identified broader system risk factors included: (6) location and ability to access medical experts for assessments, consultation or services; (7) employer and union relations (e.g. pressure from employers to return to work, or work in ways negatively impacting recovery, or tensions between unions and employers); and (8) having to go through the WSIB process while injured or ill (because it is complex, it requires multiple actions, taking up time that could have been spent in rest and recovery).
Suggestions for improvements
Workers and service providers made a number of suggestions for improving the WSIB system and how it functions overall and in the context of Northwestern Ontario.
Survey
Survey respondents’ suggestions for how they would improve the WSIB process included increasing access to supplementary services (n = 15; 35.0%) such as counselling or psychological services (n = 7; 17.5%). Individuals also listed legal aid, pain or rehabilitation specialists and disability compensation (n’s < 5) as ways to improve services for Northwestern Ontario injured workers.
Survey and interview
As survey respondents also proposed suggestions to improve the WSIB process in an open-ended fashion, we analyzed interview transcripts and answers to open-ended survey questions jointly. Injured worker and service provider suggestions for how to improve the WSIB processes were tightly aligned and included the following themes: (1) the addition of a systems or arm’s-length navigator to help workers understand and move effectively through WSIB processes; (2) greater compassion from WSIB workers; (3) continuity of care (e.g. more opportunities to speak with WSIB representatives familiar with workers’ cases); (4) increased access to and knowledge about support services, within and outside of WSIB-funded care; (5) more responsive communication from WSIB; (6) special considerations and succession planning for Northern providers; and (7) transparency (e.g. information about worker pathways and options, including available services). Corresponding sample quotations for these themes may be found in Table 4.
| Theme | Sample quotations |
|---|---|
| Addition of systems/arm’s-length navigator | “I think that there needs to be someone who is, and I don’t know how it would work, but someone who talked you through any process, like a staff services manager, knowledgeable on all aspects of [the WSIB claims and appeals process]. And you could [get help/guidance] with filling out forms, letting you know what forms you needed, walking you through those things and just check[ing] in on you. Um, it [would] make a huge difference.” – IW 4 “I would love some sort of like, I’m, I’m new, I don’t even know what it would be called, but almost like a place where they could go to, to discuss, like, consult with someone regarding navigating this system, right? So, somebody who would be syncing them up with the resources that you’re talking about who would be giving them realistic expectations around what, around what they could expect from the WSIB, what their rights are, like, educating them about that. Just somebody just sort of, like, give them, like, a roadmap of what this chapter is going to look like, of their life, like, almost.” – SP 1 |
| Compassion | “I just wish WSIB was a little bit more compassionate towards people. It’s a very stressful situation going through what people go through. I know every case is different, some are minor, some are not, some are life-threatening, some are not. Fortunately, mine wasn’t life-threatening, but did lead to lifelong problems and to be called a number instead of by my name, to me, it just feels like they push you aside, like it’s not that big of a deal.” – IW 1 “Also treating you with, you know, basic human respect and dignity.” – IW 16 “I think that like anything that’s going to help people to have to feel more seen and more heard and acknowledged, is going to be supportive for their mental health.” – SP 1 |
| Continuity of care | “Yeah, the continuity with the same person I’d say, with this, if you were seeking help, then you’d be talking to the same person all the time, I think those things same things is a good thing to have.” – IW 11 “If you have a case manager that you started with the very beginning, I’d like to see you remain with the case manager, because they pass you on to this case manager, and then the next one, the next one. But over time, they change it, it’s a, I don’t know why they do that. I don’t think they want you to have rapport with your case manager. I just think they want to keep it as business but when you’re comfortable talking with a case manager that you’re dealing with, it’s a lot easier to be open with them, and you’re not hiding things or you’re not afraid to say what you’re supposed to say or a lot more clear and more willing to give the information that they asked for. There’s no hidden agenda.” – IW 7 |
| Improved access to/knowledge about support services | “It just kills you. Some of these people really, really need help dealing with depression and they need to know how to find it.” – IW 3 “I feel like I probably could have done well with some sort of a stress management or anxiety management program.” – IW 10 “After their initial communication, they provided no information to me in regards to psychological or physiological services. I do believe that my organization extended that if I needed to use my Employee and Family Assistance Program, EFAP, that it was available to me, but I don’t believe, and in my notes I have no indication, that WSIB provided any type of supplementary care options.” – IW 12 |
| Increased/improved/responsive communication | “They definitely need to work on their communication skills. I understand 100% that they have big case loads, and that mine may not always be a priority. I’m very, very aware of that. But missing opportunities for medical appointments and to hopefully be in less pain, because they just haven’t called me back in three months is 100% unacceptable.” – IW 1 “Better communication.” – IW 13, 16 “I think they could streamline [the WSIB process] a little bit.” – IW 7 “Better communication between the case manager and the treating psychologist I think would be helpful.” – SP 1 |
| Special considerations and succession planning for Northern providers | “People will practise in WSIB until they die just because there’s not very many people and they become such an expert in it. And, and the detriment of losing that one person and all their knowledge, like, the entire province feels it.” – SP 1 “I’ve had referrals from outside of Thunder Bay for sure, yep, but I kind of stopped taking them for a little while just because they were a lot of work.” – SP 2 |
| Transparency | “I think right off the bat, they need to make it very clear that they are not working for me, they’re working for the agency. I didn’t know that, once again, because I’ve never had to deal with WSIB before. I thought they were insurance for me and to cover me and they were on my side, and then very, very quickly found out that it was not that way.” – IW 1 “WSIB likely would do themselves a massive service, if they made their initial point of contact with the consumer, aka the person who’s injured. If they explained to people upfront that this is a process that could take months and months of their time and their lives in a very difficult situation. For some reason, there’s this predisposition it seems on their part to assume that people have a clue of what happens in this bureaucratic internal thing that really presents itself as this kind of iron curtain. You have no idea what’s going on there. And they don’t explain anything to you. So, I think that likely, in the perfect world, my suggestion would be that they do some basic customer service and talk people through the initial stages.” – IW 12 “As an injured worker you don’t, you don’t know what’s required.” – IW 16 “I think clarity, clarity of process, consistency of process. Um, at least, what’s sort of the typical, there always then at least, you know when you’re deviating, right, and you can provide good rationale as to why you’re deviating because there’s at least a consistent process. Um, and I think clarity of role as well. So, when you’re asked of your opinion, from your little corner of expertise, that there’s some clarity of role that you’re, in fact, being a major influencer in the decision that happens and some kind of feedback loop, where if that doesn’t happen, that’s communicated and preferably not through the client, I, I kind of wonder if what you’re trying to do is empower the client and have the client be in charge.” – SP 3 |
Abbreviations: IW, injured/ill worker; SP, service provider; WSIB, Workplace Safety and Insurance Board. |
|
Discussion
Although workers’ compensation systems such as the WSIB are devised to reduce financial harms and promote recovery and return to work,Footnote 5 research has demonstrated that injured workers generally have poor physical health, mental health and occupational outcomes.Footnote 21Footnote 22Footnote 23Footnote 24Footnote 25Footnote 26 In our study, injured workers and service providers in Northwestern Ontario described the range of impacts from their workplace injuries, incremental impacts on injury, illness and recovery from the worker compensation system, and suggestions for improving the system intended to support them.
Consistent with previous research on workers elsewhere in the province, the Northwestern Ontario injured workers in this study described a wide range of negative impacts from their injuries and illness, including impacts on their psychological, physical, social,Footnote 21Footnote 22Footnote 23Footnote 24Footnote 25Footnote 26Footnote 27Footnote 28Footnote 29 recreational,Footnote 30 financialFootnote 30 and occupationalFootnote 31 well-being. In particular, this study identified a high rate of psychological distress among injured workers, with most survey respondents stating that their workplace injury changed their life “a lot” or “completely.”
A key finding from this work is that Northwestern Ontario injured workers clearly described incremental negative impacts from being involved in the workers’ compensation claims and appeals processes. More than half of the participants in this study rated the claims and appeals processes as extremely or very stressful. These findings are consistent with research conducted elsewhere in the province showing that injured workers involved in workers’ compensation systems report considerable levels of stress and are at greater risk of developing persistent mental health problems than those who were not injured at work, and the general population.Footnote 32Footnote 33 The injured workers and service providers highlighted several aspects of the process that could contribute to a negative claim or appeal experience, outlined below.
The injured workers in this study described specific mental health impacts of the WSIB process, including feelings of helplessness, hopelessness, shame, guilt, frustration and anger, as well as retraumatization, financial and job anxiety and insecurity, the loss of professional or occupational identity, social isolation and family role instability or conflict. These results substantiate previous research highlighting power differentials between claimants and the workers’ compensation system, and build upon previous injured workers’ accounts of de-legitimization, coercion and stigmatization perpetrated by compensation system actorsFootnote 4Footnote 34Footnote 35 occurring elsewhere in Canada. Moreover, the mental health impacts of the WSIB process described by participants lend support to previous injured worker studies describing feelings of frustration, helplessness and hopelessness resulting from “adversarial” and unjust workers’ compensation experiences,Footnote 3Footnote 34Footnote 35Footnote 36Footnote 37Footnote 38 and the consequent negative ramifications of these processes and experiences on career plans, hobbies and community involvement, finances and mental health of claimants.Footnote 30Footnote 31Footnote 36Footnote 38Footnote 39Footnote 40
We also found some very preliminary evidence that stress related to claims and appeals was different across groups. Specifically, we found that sustaining a permanent disability following workplace injury was a significant predictor of claim-related stress. This finding helps to substantiate previous research demonstrating that injured workers with permanent impairments have poorer outcomes than injured workers who fully recover and return to work, and the general population.Footnote 10 More research with larger samples is needed to confirm and identify other potential subgroups of individuals (e.g. lower preinjury income, English language learners) at risk for negative mental health impacts from the claims and appeals processes, in Northwestern Ontario and beyond. If replicated, special considerations (e.g. enhanced supports for managing stress, and different expectations for income replacement among workers unable to return to their workplaces in the same capacity) might benefit workers in the WSIB system.
Although our sample was restricted to workers and service providers in Northwestern Ontario, claimants and service providers described many challenging aspects of the claims process consistent with previous research conducted elsewhere in the province. These included care coordination and treatment planning issues,Footnote 38Footnote 41Footnote 42Footnote 43Footnote 44 communication challenges,Footnote 38Footnote 45 paperwork,Footnote 34Footnote 40 staff turnover and lack of continuity of careFootnote 35Footnote 38Footnote 46 and lack of transparency.Footnote 34Footnote 38Footnote 47 As expected, being involved in the appeals process negatively contributed to injured workers’ experience with the WSIB, and interviewees and survey respondents reported that, due to the adversarial nature of their appeals, already challenging aspects of the WSIB process were even more unsatisfactory during the appeals process. While these themes for workers in the WSIB system are not new, ours is the first study that we are aware of that shows that these issues persist in small, northern and rural communities throughout Northwestern Ontario.
Critical to the importance of our work overall, we also identified risk factors (i.e. negative, or those detracting from the experience) specific to WSIB claimants in Northwestern Ontario. For instance, we easily traced several region-specific issues to anticipated problems accessing services, including legal, social and health care services. In particular, well-known health services issues endemic in the North, such as insufficient numbers of providers to meet the population need, clearly affected the injured workers in our study. Importantly, problems related to low or no access to primary care services had cascading effects on workers, because primary care providers must assess the need for and initiate referrals to specialists, as well as plan and coordinate assessments and care. Limited access to specialist providers was also problematic, including long waitlists for local providers or the cost, logistics and time needed to travel for assessments or care while workers were ill and had family responsibilities. The COVID-19 pandemic also restricted travel for several of the workers in this study, further delaying access to assessments and care. Communication infrastructure issues were also common within this sample, including low or no access to reliable Internet or telephone service, which are likely less common in more populous parts of the province. These regional issues are consistent with research documenting disproportionate negative impacts of workplace injuries on injured workers in remote and rural communities and associated lack of access to care.Footnote 44Footnote 48Footnote 49Footnote 50Footnote 51
We also documented regional cultural impacts of workplace injury, including loss of equipment for local recreational pastimes. For example, workers described losing boats and snow machines (snowmobiles), which serve as transportation and connection to community, when their income was not adequately replaced. Policies that require individuals to sell all of their belongings in order to qualify for benefits are likely to have unintended, negative impacts on the overall recovery of people who become hurt or ill at work.
Finally, service providers in the North were very concerned about succession planning, noting that in small communities of practitioners, the whole service system suffers (and in some cases, can cease to function) when individuals, often serving as the sole providers to populations or regions, retire, move away or die. Attracting and training local providers to offer community and culturally informed services must be a priority for the WSIB to ensure adequate system function in the North.
Factors associated with the presence of psychological distress related to claims and appeals are modifiable,Footnote 52 as workplace response to injury and insurance claims and appeals processes can be altered.Footnote 53Footnote 54 Some aspects of the WSIB process that were described as protective can be maintained and enhanced for potentially underserved groups, such as access to adequate support services (mostly psychological or legal). Several workers also touted the recent introduction of a WSIB online portal to coordinate file claims and appeals; in consultation with workers and providers, WSIB may be able to further leverage technology to simplify and enhance small, rural, remote or northern community workers’ experiences.
Workers and service providers also suggested system improvements, such as
- creating arm’s-length navigators to help workers understand and move effectively through WSIB processes;
- enhancing WSIB employee compassion;
- increasing continuity of care (e.g. greater opportunity to speak with WSIB representatives familiar with one’s case);
- improving access to and knowledge about support services within and outside of WSIB-funded services;
- ensuring more responsive communication from WSIB;
- engaging in workforce development or succession planning, making special provisions for northern providers and special populations (e.g. enhanced provider training); and
- ncreasing transparency about WSIB’s role and the claims and appeals processes overall.
The main goal of all of these suggestions is to improve the well-being of injured workers.
Strengths and limitations
Although ours is the first study we are aware of describing the experiences, impacts and social service needs in small, northern and rural communities throughout Northwestern Ontario, our results should be considered within the limitations of the research design.
This study was cross-sectional, meaning that participants provided risk factor data specific to injury impact and to WSIB processes at the same time. Thus, some of our findings may have been subject to reverse causality effects, with workers experiencing negative impacts from their injuries inadvertently attributing some of their injury-related experiences to the WSIB system itself. Our design also did not give us access to information about workers’ preinjury (baseline) mental illness, which could have had an effect on workers’ descriptions of their injury impacts and risk factors while involved in the WSIB process.
We are also aware that our sample size is very small, although in line with other published, well-cited studies of the WSIB. Therefore, our findings may not represent the experience of all Northwestern Ontario workers and service providers, even though the total population of providers in the region is very small.Footnote 15 We are also aware that our assessment of risk factors is underpowered; future research with a larger sample (e.g. existing WSIB data) is needed to replicate and extend our analyses of workers’ claims- and appeals-related distress.
Our sample, besides its small size, was also limited to English speakers who were able to communicate with researchers over the telephone or computer. The experiences of new immigrants with limited English skills, very remote workers and completely indigent individuals were not fully captured in this research.
Finally, the quantitative survey measure used to assess injured workers’ experiences with the WSIB was developed for the study, and is not a validated measure of workers’ experiences. Future research is needed to validate our findings and assess their generalizability to larger samples of workers and service providers in Northwestern Ontario.
Conclusion
This mixed-methods study adds to the existing research on the plight of injured workers in Northwestern Ontario—a large and unique geographical region whose outcomes following workplace injury and illness are poorer than elsewhere in the province. It provides novel information about the experience of Northwestern Ontario injured workers, how they are multiplicatively impacted by their injuries and how the system intended to support them imparts negative impacts of its own. These workers and service providers familiar with the Ontario workers’ compensation system suggested improvements from their unique perspectives. The WSIB, policymakers, researchers and other stakeholders can use the findings in this research to improve supports for Northwestern Ontario injured workers to promote equity in their timely recovery, improved well-being and return to sustainable work.
Acknowledgements
This research was supported by a grant to DS and AK from the Injured Workers Community Legal Clinic in Toronto, Ontario.
Conflicts of interest
Declaration of interest: through her part-time private practice, Dr. Scharf provides psychological services to injured and ill workers whose care is paid for by the WSIB.
Authors’ contributions and statement
CN led the manuscript writing, contributed to data analysis and interpretation, figure preparation, and document preparation. APK designed the study, contributed to manuscript writing, data collection, analysis and interpretation. JH and JL contributed to the study design and data collection and interpretation. JK contributed to the study design, data interpretation and manuscript writing. DS led the study design and contributed to manuscript writing and data analysis and interpretation. All authors contributed to and have approved the final manuscript.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.