
Health Canada – 2011-12 – Departmental Performance Report
Table Of Content
- Minister’s Message
- Section I: Organizational Overview
- Section II: Analysis of Program Activities by Strategic Outcome(s)
- Strategic Outcome 1:
- Strategic Outcome 2:
- Program Activity 2.1: Health Products
- Performance Summary
- Program Activity 2.2: Food Safety and Nutrition
- Performance Summary
- Program Activity 2.3: Environmental Risks to Health
- Performance Summary
- Program Activity 2.4: Consumer Product Safety
- Performance Summary
- Program Activity 2.5: Substance Use and Abuse
- Performance Summary
- Program Activity 2.6: Radiation Protection
- Performance Summary
- Program Activity 2.7: Pesticide Safety
- Performance Summary
- Strategic Outcome 3:
- Internal Services
- Changes to Government Structure
- Section III: Supplementary Information
- Section IV: Other Items of Interest
Minister's Message

I am pleased to present Health Canada's 2011–2012 Departmental Performance Report, which summarizes Health Canada's work to keep Canadians healthy and safe, and to sustain our country's health programs and systems.
Legislative and regulatory modernization has continued to be a priority for Health Canada. Under the Canada Consumer Product Safety Act, we enhanced the protection of Canadians by developing regulations, policies, and standard operating procedures. We improved guidance to industry and responsiveness to consumer-reported incidents. Health Canada contributed to the Regulatory Cooperation Council, a bilateral initiative aimed at increasing regulatory transparency and cooperation between Canada and the United States. One part of the initiative, the Common Electronic Submission Gateway, will increase efficiency of drug product decision making, and improve access to medicines for patients in both countries. Going forward, the recommendations of the Red Tape Reduction Commission will help us to reduce the compliance burden of regulations without compromising on our commitment to the health and safety of Canadians.
Health Canada also worked with the Canadian Food Inspection Agency and other government partners to develop specific amendments to the Food and Drugs Act to support modernization of Canada's food safety system and more effective and efficient food safety regulation.
The final BC Tripartite Framework Agreement on First Nations Health Governance was signed on 13 October 2011, paving the way for the creation of a new First Nations Health Authority. It will assume responsibility for the design and delivery of health programs and services for First Nations in British Columbia. Health Canada also renewed First Nations and Inuit community-health programs, including those addressing maternal and child health, youth suicide, and diabetes.
Health Canada worked with the provinces, territories, and other health partners to address major sustainability issues related to our health system. In February 2011, our Government announced $39.5 million in funding, over six years, to support training for more than 100 family medicine residents, and to improve medical services in under-serviced communities, including rural and remote locations, across Canada. Eight jurisdictions have since signed contribution agreements under this initiative. Health Canada also developed the Northern Wellness approach to health funding that aims to improve health outcomes for individuals, families and communities while recognizing the unique realities of life in the North.
Health Canada continues to implement strategies that focus attention and resources on areas that will provide the greatest potential benefits to Canadians, for now and in the future.
The Honourable Leona Aglukkaq, P.C., M.P.
Minister of Health
Section I: Organizational Overview
Raison d'être
Health Canada is responsible for helping Canadians maintain and improve their health. It is committed to improving the lives of all Canadians and to making this country's population among the healthiest in the world, as measured by longevity, lifestyle and effective use of the public health care system.
Responsibilities
Health Canada has many roles and responsibilities that help Canadians maintain and improve their health. First, as a regulator, Health Canada is responsible for the regulatory regimes governing the safety of products including food, pharmaceuticals, medical devices, natural health products, consumer products, chemicals, radiation emitting devices, cosmetics and pesticides. It also regulates tobacco products and controlled substances, public health on aircraft, ships and other passenger conveyances, and helps manage the health risks posed by environmental factors such as air, water, radiation and contaminants.
Health Canada is also a service provider. For First Nations and Inuit, Health Canada supports: basic primary care services in remote and isolated communities and public health programs including communicable disease control (outside the Territories); home and community care; and, community-based health programs focusing on children and youth, mental health and addictions. Health Canada also provides a limited range of medically-necessary, health-related goods and services to eligible First Nations and Inuit that are not otherwise provided through other public programs or private insurance plans.
Health Canada is a catalyst for innovation, a funder, and an information provider in Canada's health system. It works closely with provincial and territorial governments to develop national approaches to health system issues, and promotes the pan-Canadian adoption of best practices. It administers the Canada Health Act, which embodies national principles for a universal and equitable, publicly-funded health care system. It provides policy support for the federal government's Canada Health Transfer to provinces and territories, and provides funding through grants and contributions to various organizations to help meet overall health system objectives. Health Canada draws on leading-edge science and policy research to generate and share knowledge and information to support decision-making by Canadians, the development and implementation of regulations and standards, and health innovation.
Strategic Outcomes and Program Activity Architecture (PAA)
Health Canada updated its Program Activity Architecture (PAA) and the supporting performance measurement framework, effective April 1, 2011. The new PAA improves the alignment of Health Canada programs along the department's three business lines: health system innovation, consumer protection and environmental health and First Nations and Inuit health. Together, with strengthened performance measurement indicators and streamlined financial coding structure, this will improve Health Canada's ability to measure and monitor results achieved for Canadians. Accordingly, all strategic outcomes and program activities are now focused more clearly on core departmental responsibilities. Some financial tables are complicated by the fact that actual spending figures for 2010-11 are based on the old PAA. A crosswalk between the old and new PAA can be found in the RPP for 2011-12. Where necessary, footnotes are provided with the affected tables for greater clarity.
Strategic Outcome 1
A Health System Responsive to the Needs of Canadians
- Program Activity 1.1 : Canadian Health System
- Program Activity 1.2 : Specialized Health Services
- Program Activity 1.3 : Official Language Minority Community Development
Strategic Outcome 2
Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating
- Program Activity 2.1 : Health Products
- Program Activity 2.2 : Food Safety and Nutrition
- Program Activity 2.3 : Environmental Risks to Health


- Program Activity 2.4 : Consumer Product Safety
- Program Activity 2.5 : Substance Use and Abuse
- Program Activity 2.6 : Radiation Protection
- Program Activity 2.7 : Pesticide Safety
Strategic Outcome 3
First Nations and Inuit communities and individuals receive health services and benefits that are responsive to their needs so as to improve their health status
- Program Activity 3.1 : First Nations and Inuit Primary Health Care
- Program Activity 3.2 : Supplementary Health Benefits for First Nations and Inuit
- Program Activity 3.3 : Health Infrastructure Support for First Nations and Inuit
Internal Services
![]()
The Health Canada Program Activity Architecture supports achievement of three of four themes in the Federal Sustainable Development Strategy:
Organizational Priorities
Priority I – Promote Health System Innovation
Type : Ongoing
Links to Strategic Outcome(s) : 1, 2 and 3
Why is this a priority? : The health care system in Canada is vital to addressing the health needs of Canadians wherever they live and whatever their financial circumstances. Given the importance of the health system to Canadians, Health Canada places a priority on working with partners to improve the effectiveness and efficiency of the health system.
2011-2012 Performance
Worked with provinces, territories, First Nations and Inuit communities, and other health care partners on advancing health system sustainability.
- Supported Canada Health Infoway to promote the development and use of eHealth technologies in Canada, such as Electronic Medical Records in physicians' offices and Electronic Health Records. As of March 31, 2012, 52.2% of Canadians have an Electronic Health Record available to their health care professionals.
- Renewed funding for national non-profit organizations, like the Canadian Partnership Against Cancer and the Canadian Institute for Health Information, and provided strategic project funding to health care partners to support innovation and the sharing of leading practices through the Health Care Policy Contribution Program.
- Continued support for the Mental Health Commission of Canada to foster change and innovation in the area of mental health, including the development of national strategy, knowledge exchange, reducing stigma and finding ways to help the homeless with mental health issues.
Collaborated with partners to improve access to physicians, nurses and other health care providers.
- The Health and Human Resource Strategy provided strategic funding to provinces and territories to support the training of physicians for areas of high need. In February 2011, the Minister announced $39.5M in funding over six years for more than 100 family medicine residents to receive training and provide medical services in rural and remote communities across Canada. Eight agreements have been signed with provinces and territories.
- The Internationally Educated Health Professionals Initiative (IEHPI) supported activities to assist the integration of internationally educated health care professionals into Canada's health workforce. To date, contribution agreements have been signed between Health Canada and all of the provinces and territories.
Supported health promotion and chronic disease prevention strategies (e.g., tobacco and childhood obesity) in collaboration with provincial and territorial partners.
- A compliance and enforcement plan for the Act to Amend the Tobacco Act was in place by the fall of 2011, addressing the key elements of minimum packaging, restrictions and advertising, prohibition of certain additives in cigarettes, little cigars and blunt wraps.
- The Government of Canada renewed the Federal Tobacco Control Strategy (FTCS) through Budget 2012.
- Facilitated provincial/territorial collaboration for improving the consistency of school food and beverage criteria and enhancing implementation efforts. Coordinated an expert panel on Supportive Environments for Learning: healthy eating and physical activity within Comprehensive School Health at the Chronic Disease Prevention Alliance of Canada fourth annual Pan-Canadian conference. This collaboration has contributed to policy priorities identified in the Curbing Childhood Obesity: FPT Framework for Action to Promote Healthy Weights.
Priority II - Modernize Health Protection Legislation and Programs
Type : Ongoing
Links to Strategic Outcome(s) : 2
Why is this a priority? : Rapid technological changes, the advent of products that blur traditional definitions and incorporate innovative components, challenge Health Canada's ability to carry out its health and safety mandate. To address this challenge, Health Canada continues to modernize its regulatory programs.
2011-2012 Performance
Advanced initiatives to enhance the protection of the health and safety of Canadians through the Canada Consumer Product Safety Act. (CCPSA)
- The new, modernized product safety legislation, the CCPSA, came into force on June 20, 2011.
- Health Canada developed new regulations, policies, guidance documents, standard operating procedures and processes for industry and consumer reported incidents.
Addressed environmental risks to the health of Canadians.
- Developed an air health indicator (AHI) for ozone and for fine particulate matter to monitor trends in mortality and morbidity resulting from exposure to air pollution.
- Provided guidance and expert advice to public health and emergency personnel in the development of Heat Alert and Response Systems (HARS) in their communities, as well as training for health professionals to reduce the vulnerability of their community to extreme heat.
- Expanded the Air Quality Health Index, which enables Canadians to make more informed decisions regarding their health by limiting exposure.
- Raised awareness of radon through the publication of the Cross-Canada Survey of Radon Concentrations in Homes.
- Successfully launched the second phase of the Chemicals Management Plan (first launched in 2006) whereby progress was made towards the 2015-16 goal of assessing, and where appropriate initiating the management of, some 1500 of 3000 remaining priority chemicals to be addressed by 2020.
Improved the capacity to do quality and timely reviews of human drugs and medical devices, including implementing modernized user fees.
- Worked on reducing the backlog of reviews for pharmaceuticals, medical devices and natural health products.
- Tested the use of foreign review information for Generic Drug Reviews; explored the use of foreign reviews/approvals of post-authorization changes; and eliminated the Notifiable Change review process for chemistry and manufacturing changes to human pharmaceuticals.
- The Updated User Fee Regulations containing updated user fees came into effect on April 1, 2011. Under the new user fees regulations, all fee categories and fee lines are subject to penalty if performance standards are not met. Cost recovery targets for 1st Decisions met 100% service standards in all program areas.
Priority III - Strengthen First Nations and Inuit Health Programming
Type : Ongoing
Links to Strategic Outcome(s) : 3
Why is this a priority? : While health outcomes for most Canadians are improving, First Nations and Inuit continue to experience serious health challenges. Health Canada plays an important role in supporting the delivery of, and access to, health programs and services for First Nations and Inuit. Health Canada works with partners on innovative approaches to strengthen access, improve integration of health services, and encourage greater control of health care delivery by First Nations and Inuit.
2011-2012 Performance
Worked on implementing renewed First Nations and Inuit community health programs including those addressing diabetes, youth suicide, and maternal and child health.
- Supported healthy pregnancy and early infancy services through Maternal Child Health (MCH) programming in 225 communities (a total of 125 projects).
- Supported early childhood development through Aboriginal Head Start On Reserve in 316 sites.
- Approximately 150 community based suicide prevention projects were implemented in First Nations and Inuit communities across Canada.
- Assisted in improving access to healthy foods, healthy eating, physical activity and achieving healthy body weights, through the Aboriginal Diabetes Initiative in 673 communities.
- Four regional food security plans were developed (BC, SK, QC and Atlantic) and two others are under development (MB, AB). Over 113 community-based food security projects are in place across the country.
Strengthened the provision of primary health care services to First Nations communities, ensuring that nurses have the clinical expertise and support they require, to provide needed primary health care.
- Implemented 40 pilot projects to promote new and innovative nursing service delivery approaches and to support advanced training, necessary for remote and isolated nursing practice across all regions. Efforts included: collaborative delivery teams; integration of technology, new and more flexible operating hours and improved nursing education; and, supported approximately 750 nurses to enhance, upgrade or maintain competencies.
- Provided preventive and basic oral health care services to 260 communities through the Children's Oral Health Initiative.
- Launched a national immunization social marketing campaign.
- Enhanced public health emergency preparedness and response with 98% of First Nation communities having a communicable disease emergency plan.
- Funded four community-based environmental health research projects and 26 regionally-based environmental health research projects through the Regional First Nations Environmental Contaminants Program.
The final “BC Tripartite Framework Agreement on First Nation Health Governance” was signed on October 13, 2011. The Saskatchewan First Nations Health and Wellness Plan was drafted in consultation with the Province and the Federation of Saskatchewan First Nations Health and Wellness Plan Chiefs in Assembly.
Supported effective delivery of Non-Insured Health Benefits to eligible First Nations and Inuit.
- Expanded the Prescription Monitoring Program to all regions, except Quebec. There was a 30% increase in client participation, as of September 2011.
- Changed the dental compensation model under the Non-Insured Health Benefits (NIHB) Program.
- Continued the development of a standardized price file for select medical supplies and equipment.
- Streamlined Dental Pre-Determination through the removal of endodontic pre-determination.
- Implemented a transition plan to integrate the new NIHB clients resulting from the McIvor case and the creation of the Qalipu Mi'kmaq Band in Newfoundland.
Continued to harmonize the management of contribution agreements with Aboriginal Affairs and Northern Development Canada and other partners.
While transitioning to new funding models, Health Canada permitted stakeholders to extend their existing agreements for a one year period.Priority IV - Align resources to priorities in a way that is flexible and forward-looking
Type : Ongoing
Links to Strategic Outcome(s) : 1, 2 and 3
Why is this a priority? : Given an extensive range of legislated responsibilities, an active policy and program agenda and the need for significant investments in the infrastructure to support core departmental operations and programming, Health Canada is committed to identifying efficiencies and reallocating resources to deliver the best results possible and provide value for money.
2011-2012 Performance
- Developed and implemented a Strategic Investment Planning Process for the department-wide prioritization of projects that best support Government of Canada objectives and reflect the areas of greatest risk for Health Canada.
- Updated the departmental financial and materiel management system to support the adoption of common and standardized processes and configurations promoted by the Office of the Comptroller General of Canada.
- Automated the Grants and Contributions Information Management System and modernized processes and tools to reduce administrative burden.
Priority V - Improve Service Delivery
Type : Ongoing
Links to Strategic Outcome(s) : 1, 2 and 3
Why is this a priority? : Health Canada is committed to focusing improvements to service delivery in support of core programs, and establishing and tracking the accountability mechanisms necessary for service improvement.
2011-2012 Performance
- Multi-year IT Application Reduction Initiative reduced duplicate /non-essential applications to decrease cost and complexity risks.
- Laboratory Infrastructure Renewal Plan implemented to support science priorities while reducing capital pressures.
- Departmental Security Plan and departmental Business Continuity Management Program developed.
Priority VI - Increase transparency and innovative communications and engagement with Canadians
Type : Ongoing
Links to Strategic Outcome(s) : 1, 2 and 3
Why is this a priority? : Health Canada is committed to engaging Canadians so that its policies, programs and services reflect citizen priorities and perspectives, and to using the internet and new technological tools to make information easily accessible.
2011-2012 Performance
- A more corporate and strategic approach to tracking, planning, executing and reporting of stakeholder engagement/and consultation activities based on a new Corporate Consultations Protocol.
- Web Presence Renewal Initiative launched; included the creation of a DG Steering Committee and a working group to review web governance.
- Departmental guidelines developed for the use of social media.
Risk Analysis
Health Canada, as part of its commitment to effective management and accountability, employs integrated risk management tools to recognize, understand, accommodate and capitalize on new challenges and opportunities. Health Canada's approach builds on the Treasury Board Secretariat's 2010 Framework for the Management of Risk, which in turn, is based on the International Organization for Standardization's Risk Management Standard (ISO 31000:200). The Standard includes a definition of risk as "the effect of uncertainty on outcomes."
Health Canada, as a public sector organization, faces risk every day. Risk is unavoidable and present in virtually every human situation. While most people think of the word "risk" as referring only to "hazards", as a management concept, risk is neutral and includes consideration of threats and opportunities. For instance, in its work related to food and nutrition, Health Canada is mindful of potential opportunities (e.g., access to a varied marketplace of healthy food) as well as the potential threats (illness related to poor food choices) and takes appropriate actions.
In a dynamic and complex environment, effective management of risk contributes to improved decision-making, better allocation of resources and, ultimately, better results for Canadians. Health Canada actively managed and responded to risks – both positive (opportunities) and negative (threats) – in 2011-2012. A selection of activities in Section IV, Other Items of Interest, demonstrate the range of risks Health Canada manages and the concrete interventions made to reduce impacts or probabilities of adverse risk, or to enhance the impacts or probabilities of positive risks.
Observations
It is important that there be targeted, relevant guidelines and tools for risk assessment and management to support the regulatory and other initiatives of Health Canada. As well, collaboration enhanced Health Canada's ability to respond to challenges. Close internal and external collaboration will remain essential to allow for appropriate policy and program responses. For detailed information on Health Canada's responses to risks please see Section IV.
New hazards are emerging on the horizon. Health Canada will continue to collaborate with law enforcement and public health experts to address issues such as emerging synthetic recreational drugs. Drug-resistant strains of communicable diseases such as tuberculosis will pose health challenges in Canada. Health Canada will continue to collaborate and communicate internally and externally to best respond to these challenges.
Next Steps
Going forward, Health Canada will continue the integration of risk management in operational and strategic planning. Continued implementation of the 2010 Treasury Board Secretariat's Framework for the Management of Risk will be undertaken and will serve to develop risk management capability throughout Health Canada. Health Canada will engage with internal as well as external stakeholders to allow for a comprehensive approach to risk management. This will require a range of outreach activities supporting a better understanding and uptake on the relationship between risk management, planning, resource allocation, and accountability. Health Canada's objective is to be systematic, proactive and adaptive as it responds to the strategic and operational uncertainties of the next few years.
Summary of Performance
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 3,345.7 | 3,927.4 | 3,786.3 |
*The decrease from forecast to planned spending is primarily associated with changes made to the Program Activity Architecture for 2011-2012.
Health Canada's financial resources had a direct impact on its ability to achieve its strategic outcomes and deliver on its program activities. The following sections highlight Health Canada's performance and demonstrate linkages between resources and results.
At the outset of the 2011-12 fiscal year, Health Canada's planned spending was $3,345.7 million. Through Main Estimates and Supplementary Estimates, Health Canada was allocated total authorities of $3,927.4 million. Actual spending for Health Canada was $3,786.3 million.
| Planned | Actual | Difference |
|---|---|---|
| 9,988 | 9,961 | 35 |
The human resources table above provides a summary of the total planned human resources and actual human resources for Health Canada for fiscal year 2011-12.
Strategic Outcome 1: A Health System Responsive to the Needs of Canadians
| Performance Indicators | Targets | Actual Results |
|---|---|---|
# of new or modified health system policies, proposals or practices to advance health system priorities by:
|
Increased # of policies, practices and proposals put forward to address health system priorities. |
|
| Examples of collaborative working arrangement that address health system priorities | Better and increased collaboration among Health Canada and health system stakeholders. |
|
| Program Activity | 2010-11 Actual Spending ($ millions) |
2011-2012 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | |||
| Canadian Health System | 377.5 | 301.0 | 302.8 | 400.4 | 371.3 | Healthy Canadians |
| Specialized Health Services | 23.6 | 23.6 | 25.5 | 22.3 | ||
| Official Language Minority Community Development | 39.3 | 39.3 | 39.4 | 39.0 | ||
| Canadian Assisted Human Reproduction | 3.4 | |||||
| International Health Affairs | 18.7 | |||||
| Workplace Health | 31.7 | |||||
| Total Spending for SO1 | 363.9 | 365.7 | 465.3 | 432.6 | ||
*Note: A new Program Activity Architecture (PAA) came into force April 1, 2011. In the Actual spending column for 2010-11 those rows representing new Program Activities that were not part of the PAA in that year are blank. Similarly, for 2011-12 figures, rows representing discontinued Program Activities are blank. For a crosswalk between the old and new PAA see the RPP for 2011-12.
Strategic Outcome 2: Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating
| Performance Indicators | Targets | Actual Results |
|---|---|---|
| % of target audience aware of the health risks associated with food, products, substances and environments, and of the benefits of healthy eating. Note: Should Public Opinion Research (POR) data be unavailable to support reporting on awareness, performance data on information outputs may be used as proxy performance measures. |
See performance indicator details for program activities: 2.1 Health Products 2.2 Food Safety and Nutrition 2.3 Environmental Risks to Health 2.4 Consumer Product Safety 2.5 Substance Use and Abuse 2.7 Pesticide Safety |
|
% and # of timely regulatory actions by:
|
See performance indicator details for program activities: 2.1 Health Products 2.2 Food Safety and Nutrition 2.3 Environmental Risks to Health 2.4 Consumer Product Safety 2.7 Pesticide Safety |
|
Level of exposure or prevalence by:
|
See performance indicator details for program activities: 2.3.4 Health Impacts of Chemicals 2.5 Substance Use and Abuse 2.6 Radiation Protection |
|
| Program Activity | 2010-11 Actual Spending ($ millions) | 2011-2012 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | |||
| Health Products | 170.6 | 168.3 | 168.3 | 177.3 | 177.2 | Healthy Canadians |
| Food Safety and Nutrition | 58.4 | 57.8 | 57.8 | 68.0 | 67.9 | |
| Sustainable Environmental Health | 134.9 | |||||
| Environmental Risks to Health | 48.1 | 48.1 | 119.4 | 105.1 | ||
| Consumer Product Safety | 27.9 | 28.0 | 28.0 | 32.7 | 27.7 | |
| Substance Use and Abuse | 124.0 | 139.1 | 139.1 | 142.2 | 123.0 | |
| Radiation Protection | 1.8 | 1.8 | 14.0 | 14.0 | ||
| Pesticide Safety | 46.3 | 34.1 | 34.1 | 48.1 | 46.8 | |
| Total Spending for SO2 | 477.2 | 477.2 | 601.7 | 561.7 | ||
*Note: A new Program Activity Architecture (PAA) came into force April 1, 2011. In the Actual spending column for 2010-11 those rows representing new Program Activities that were not part of the PAA in that year are blank. Similarly, for 2011-12 figures, rows representing discontinued Program Activities are blank. For a crosswalk between the old and new PAA see the RPP for 2011-12.
Strategic Outcome 3: First Nations and Inuit communities and individuals receive health services and benefits that are responsive to their needs so as to improve their health status
| Performance Indicators | Targets | Actual Results |
|---|---|---|
| Non-Insured Health Benefits (NIHB) Program utilization rate (percentage of eligible clients who accessed at least one NIHB benefit) | Maintain access levels according to medical necessity. | Access Levels maintained. Utilization rates remain stable over the past 2 years, Pharmacy (64%) and Medical Supplies and Equipment (6%), with the Dental utilization rate (36%) decreasing by 1% since 2010-11. |
| % of the on-reserve population who rate their own health status as excellent or very good | Maintain existing levels. | 44.1% of First Nations adults living on reserve rated their health status as either excellent or very good. (Regional Health Survey 2008-10). This represents an increase from 39.9% in 2002-03. |
| # of First Nations and Inuit engaged in the control, design, development and delivery of health programs and services based on their own identified needs | 5% increase over 5 years (The baseline of 383, established in 2011-12, is expected to increase by 5% by 2016-17.) |
First Nations and Inuit recipients of contribution agreements engaged in the control, design, development and delivery of health programs and services based on their own identified needs in 383 cases. |
| Program Activity | 2010-11 Actual Spending ($ millions) |
2011-2012 | Alignment to Government of Canada Outcomes | |||
|---|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | |||
| First Nations and Inuit Primary Health Care | 940.0 | 940.0 | 957.8 | 949.1 | Healthy Canadians | |
| Supplementary Health Benefits for First Nations and Inuit | 983.9 | 983.9 | 1,137.5 | 1,111.5 | ||
| Health Infrastructure Support for First Nations and Inuit | 256.8 | 256.8 | 353.4 | 351.6 | ||
| First Nations and Inuit Health Programming and Services | 2,402.1 | |||||
| Total Spending for SO3 | 2,180.7 | 2,180.7 | 2,448.7 | 2,412.2 | ||
*Note: A new Program Activity Architecture (PAA) came into force April 1, 2011. In the Actual spending column for 2010-11 those rows representing new Program Activities that were not part of the PAA in that year are blank. Similarly, for 2011-12 figures, rows representing discontinued Program Activities are blank. For a crosswalk between the old and new PAA see the RPP for 2011-12.
Internal Services
| 2011–12 Actual Spending ($ millions) | 2011-2012 | ||||
|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | ||
| Internal Services | 357.1 | 322.1 | 322.1 | 411.7 | 379.8 |
| Total Spending for Internal Services | 322.1 | 322.1 | 411.7 | 379.8 | |
Note: Variances between planned spending and actual spending are explained in more detail, where necessary, in Section II.
Contribution to the Federal Sustainable Development Strategy (FSDS)
The Federal Sustainable Development Strategy (FSDS) outlines the Government of Canada's commitment to improving the transparency of environmental decision-making by articulating its key strategic environmental goals and targets. Health Canada provides that consideration of these outcomes is an integral part of its decision-making processes. Health Canada contributes to the following FSDS themes as denoted by the visual identifier(s) and associated program activities below:
2.3 Environmental Risks to Health
2.6 Radiation Protection
3.1.2 First Nations and Public Health Protection
Internal Services
Health Canada has also strengthened its application of the Cabinet Directive on Environmental Assessment of Policy, Plan and Program Proposals by ensuring environmental effects were considered in decision-making processes. During the reporting period, one detailed strategic environmental assessment (SEA) was prepared on the Chemicals Management Plan (CMP). The assessment found that the CMP had positive environmental effects on goals and targets under Themes I – Addressing Climate Change and Air Quality, and Theme II – Maintaining Water Quality and Availability. Further information on the results of the SEA is available on the CMP website.
For more information on Health Canada's activities to support sustainable development and strategic environmental assessments, please visit the departmental website. For complete information on the FSDS, please visit the Environment Canada website.
Expenditure Profile
For the 2011-12 fiscal year, Health Canada spent $3,786.3 million to meet expected program activity results and contribute to the achievement of departmental strategic outcomes. The figure below illustrates Health Canada's spending trend from 2009-10 to 2011-12.
| 2011-2012 Departmental Spending Trend $ millions) | 2009-2010 | 2010-2011 | 2011-2012 |
|---|---|---|---|
| Main Estimates | 3,368.7 | 3,419.4 | 3,343.9 |
| Planned Spending | 3,587.0 | 3,448.5 | 3,345.7 |
| Total Authorities | 3,813.3 | 3,859.6 | 3,927.4 |
| Actual Spending | 3,748.9 | 3,752.6 | 3,786.3 |
| Canada's Economic Action Plan | 211.9 | 245.8 | 0.0 |
For the 2009-10 to 2011-12 periods, the total spending includes all Parliamentary appropriation sources: Main Estimates, Supplementary Estimates, and funding from various Treasury Board Votes.
For Canada's Economic Action Plan (CEAP) in 2010-11 the amount does not include the $500 million authorized in statutory funding for Canada Health Infoway and the corresponding $67.7 million in spending.
Departmental Spending Trend ($ millions)

The table below offers a comparison of the Main Estimates, planned spending, total authorities and actual spending for the most recently completed fiscal year, as well as the historical actual spending figures for the previous year.
| Program Activity | 2010-11 Actual Spending ($ millions) | 2011-2012 | |||
|---|---|---|---|---|---|
| Main Estimates | Planned Spending | Total Authorities | Actual Spending | ||
| Canadian Health System | 377.5 | 301.0 | 302.8 | 400.4 | 371.3 |
| Specialized Health Services | 23.6 | 23.6 | 25.5 | 22.3 | |
| Official Language Minority Community Development | 39.3 | 39.3 | 39.4 | 39.0 | |
| Canadian Assisted Human Reproduction | 3.4 | ||||
| International Health Affairs | 18.7 | ||||
| Workplace Health | 31.7 | ||||
| Health Products | 170.6 | 168.3 | 168.3 | 177.3 | 177.2 |
| Food Safety and Nutrition | 58.4 | 57.8 | 57.8 | 68.0 | 67.9 |
| Sustainable Environmental Health | 134.9 | ||||
| Environmental Risks to Health | 48.1 | 48.1 | 119.4 | 105.1 | |
| Consumer Product Safety | 27.9 | 28.0 | 28.0 | 32.7 | 27.7 |
| Substance Use and Abuse | 124.0 | 139.1 | 139.1 | 142.2 | 123.0 |
| Radiation Protection | 1.8 | 1.8 | 14.0 | 14.0 | |
| Pesticide Safety | 46.3 | 34.1 | 34.1 | 48.1 | 46.8 |
| First Nations and Inuit Primary Health Care | 940.0 | 940.0 | 957.8 | 949.1 | |
| Supplementary Health Benefits for First Nations | 983.9 | 983.9 | 1,137.5 | 1,111.5 | |
| Health Infrastructure Support for First Nations | 256.8 | 256.8 | 353.4 | 351.6 | |
| First Nations and Inuit Health Programming and Services | 2,402.1 | ||||
| Internal Services | 357.1 | 322.1 | 322.1 | 411.7 | 379.8 |
| Total Spending | 3,752.6 | 3,343.9 | 3,345.7 | 3,927.4 | 3,786.3 |
*Note: A new Program Activity Architecture (PAA) came into force April 1, 2011. In the Actual spending column for 2010-11 those rows representing new Program Activities that were not part of the PAA in that year are blank. Similarly, for 2011-12 figures, rows representing discontinued Program Activities are blank. For a crosswalk between the old and new PAA see the RPP for 2011-12.
**Note: Variances between planned spending and actual spending are explained in more detail, where necessary, in Section II.
At the outset of the 2011-12 fiscal year, Health Canada's planned spending was $3,345.7 million. Through Main Estimates and Supplementary Estimates, Health Canada was allocated total authorities of $3,927.4 million. Actual Health Canada spending was $3,786.3 million.
The $1.9 million increase from Main Estimates to planned spending is mainly due to funding for the Genomics Research and Development Initiative.
The $581.7 million increase from planned spending to total authorities is mainly due to incremental funding to protect Canadians' health and the environment through a renewed Chemicals Management Plan; for the renewal of the Clean Air Regulatory Agenda; for the assessment, management, and remediation of federal contaminated sites; to help Canadians adapt to the impacts of climate change under Canada's Clean Air Agenda; to support the creation of a new First Nations Health Authority which ultimately will be responsible to deliver health services to First Nations in British Columbia, as per the British Columbia Tripartite Framework Agreement in First Nations Health Governance; and for the Brain Canada Foundation to fund neuroscience research to advance knowledge of the treatment of brain disorders.
The $141.1 million difference between total authorities and actual spending is mainly the result of the timing of approvals of certain projects and initiatives: the Health Council, Non-Insured Health Benefits (NIHB) uptake of new Qalipu NIHB eligible recipients, and strategies to manage Health Canada's multi-year investment plan.
Estimates by Vote
For information on Health Canada's organizational Votes and/or statutory expenditures, please see the Public Accounts of Canada 2012 (Volume II). An electronic version of the Public Accounts 2012 is available on the Public Works and Government Services Canada's website.
Section II: Analysis of Program Activities by Strategic Outcome(s)
Strategic Outcome 1: A Health System Responsive to the Needs of Canadians
Canadians expect their governments to provide a health system that meets their needs and that delivers results effectively and efficiently. In addition to ensuring that it meets specific federal responsibilities, such as health services for federal employees and during international events held in Canada, Health Canada works with provincial and territorial governments as well as health organizations and other stakeholder groups to address the health objectives of Canadians. Research and policy analysis, support and funding to test innovations in health service delivery and monitoring of provincial and territorial application of the Canada Health Act all lead to continuing improvement in Canada's health system.
- Program Activity 1.1 : Canadian Health System
- Program Activity 1.2 : Specialized Health Services
- Program Activity 1.3 : Official Language Minority Community Development
Program Activity 1.1: Canadian Health System
The goal of this Program Activity is to provide strategic policy advice, research and analysis, and program support to provinces and territories, partners and stakeholders on health care system issues. Mindful of long-term equity, sustainability and affordability considerations, Health Canada collaborates and targets its efforts with provinces and territories, national and international organizations, health care providers, professional associations, other key stakeholders and Canadians in order to support improvements to the health care system, such as improved access, quality and integration of health care services. These targeted efforts are in place to better meet the health needs of Canadians, wherever they live or whatever their financial circumstances. Focusing on emerging health issues enables Health Canada to strategically position itself as a proactive organization, and targeted Grants and Contributions funding to support our health partners helps to reaffirm that Health Canada is an active player in tackling domestic and global health issues.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 302.8 | 400.4 | 371.3 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 321 | 188 | 133 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Acts as a catalyst to address current and emerging health issues and priorities. | Actions taken to respond to current and emergent issues by:
|
Increased adoption of new approaches, models and best practices in health care system. | Initiatives contributing to improved sustainability of the health care system included:
|
Performance Summary
Work under this program activity contributed to Health Canada's ongoing responsibility for policy, program, and research support for health care system improvements; oversight of provincial and territorial compliance with the Canada Health Act; collaboration with provinces, territories, and other partners to address the health and health care needs of all Canadians.
In particular, Health Canada continued to work with provincial, territorial and other partners on major health system sustainability issues, supporting projects to address Canada's health human resource needs under the umbrella of the Pan-Canadian Health Human Resource Strategy (HHRS), including funding for residency training positions in family medicine in underserviced communities. In February 2011, the Minister announced $39.5M in funding over six years to support more than 100 family medicine residents to receive training and provide medical services in rural and remote communities across Canada.
The Internationally Educated Health Professionals Initiative (IEHPI) continued to support activities to facilitate the integration of internationally educated health care professionals into Canada's health workforce. To date, contribution agreements have been signed between Health Canada and all of the provinces and territories. Agreements support work to achieve the objectives of both the IEHPI and the Pan-Canadian Framework for the Assessment and Recognition of Foreign Qualifications (FQR Framework), led through Human Resources and Skills Development Canada. The FQR Framework helps guide the implementation of foreign qualification recognition processes that are fair, consistent, transparent and timely.
Health Canada continued support for the Mental Health Commission of Canada to foster change and innovation in the area of mental health, including the development of a national strategy, knowledge exchange, reducing stigma, and finding ways to help the homeless with mental health issues.
Health Canada also implemented a funding agreement to develop new, more cost-effective and sustainable community-integrated palliative care models and services, to be delivered in a broader range of settings and by a wider variety of care providers.
Health Canada and the Public Health Agency of Canada developed an innovative contribution agreement with the Government of Nunavut that combines funding for several community based health promotion and disease prevention programs into one agreement. The new approach enables the Government of Nunavut to focus more on community wellness and less on administrative processes. Negotiations are ongoing with the other two territories.
Health Canada continued to work with international partners to demonstrate leadership on global health issues through membership and/or participation in the Pan-American Health Organization (PAHO), the World Health Organization (WHO), including the World Health Organization - Framework Convention on Tobacco Control (WHO-FCTC), the International Agency for Research on Cancer (IARC) and the Organization for Economic Co-Operation and Development (OECD). Canada's priorities were advanced on key issues including prevention and control of non-communicable diseases, illicit trade in tobacco products, counterfeit medicines, maternal infant and child nutrition, and HIV/AIDS. Health Canada continues to build strong bilateral relationships with key countries such as the U.S, China, Mexico and Brazil through partnerships such as the Global Health Security Initiative.
As of March 31, 2012, 52.2% of Canadians have an electronic health record available to their health care professionals. As well, progress has been made in implementing other eHealth technologies, such as electronic medical records in physicians' offices, and encouraging their use by clinicians.
Lessons Learned
Close collaboration with provinces, territories and other partners contributed to improvements in the health care system, including increased medical residency training positions in rural and remote communities; the development of tools for the assessment, bridge training and integration of internationally educated professionals into the Canadian health care workforce; and fostering community relationships to collectively monitor and address health system priorities.
Program Activity 1.2: Specialized Health Services
These specialized program activities provide delivery of occupational health services to public servants and work to ensure that Health Canada is prepared and able to continue services in the event of a national emergency. By working proactively to reduce the number of workdays lost to illness, Health Canada is promoting a productive public service, thereby delivering results to Canadians. This Program Activity also ensures that Health Canada works internally and with partners to ensure that Health Canada has preparedness plans that are ready for execution in the event of a national emergency. Ensuring that organizations have plans in place that take into account all facets of their legislated responsibilities helps Health Canada continue to deliver services to Canadians when most needed. This includes coordination with other members of the Health Portfolio and partners across the Government of Canada. As part of this work Health Canada arranges for the provision of health services to Internationally Protected Persons when they are visiting Canada for regular visits or in conjunction with international events such as summit meetings or international sporting events. Together, these specialized health services aim to ensure continuity of services and capacity in day to day operations as well as in extraordinary and unpredictable circumstances such as a national emergency or disease outbreaks such as H1N1.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 23.6 | 25.5 | 22.3 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 300 | 225 | 75 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Timely system response to public service employees with psycho-social health problems. | #, % of public service employee clients' psycho-social problems dealt with within service standards. | 70% (represents the current Industry standard). | 85% of psycho-social problems addressed within service standards despite an increase in volume (from 7% to 8.7%). |
| Coordinated, effective emergency response. | Congruity between planned and executed emergency response (includes plans for Internationally Protected Persons). | The Emergency Preparedness and Response is defined in the Health Portfolio Emergency Response Plan (HPERP), which was signed in January 2010. After an event, an After-Action Report is developed in consultation with all parties involved in responding to the emergency to assess the response and deficiencies/gaps. The gaps/deficiencies are addressed in regular updates to the HPERP. |
|
Performance Summary
While managing increases in volume, Health Canada provided timely psycho-social and occupational health support to employees across the public service.
Health Canada developed over 70 health contingency plans for Internationally Protected Persons and their family members while visiting Canada including the royal visit of the Duke and Duchess of Cambridge.
Preparedness exercises are designed to test how well emergency plans and procedures work during simulated emergency situations. Health Canada prepared and coordinated national exercises designed to identify security related gaps and mitigation measures. Seven plans were tested against the Emergency Management Act and assessed during and following activations. Furthermore, Health Canada and the Public Health Agency of Canada initiated an emergency preparedness risk identification and assessment.
Health Canada was also involved in responding to a critical incident (a radioactive threat presented by the defective nuclear reactors in Fukushima, Japan) requiring consultation and coordination with other government departments. As part of this incident, Health Canada worked with the Public Health Agency of Canada to develop an After-Action Report to assess the response. Identified areas for improvement were then addressed in an Annex to the Health Portfolio Emergency Response Plan (HPERP) in preparation for possible future events.
Lessons learned
The effectiveness of emergency plans and procedures were assessed through reviews and exercises. These identified performance deficiencies and opportunities to improve services and responses. Partners discussed the recommendations for improvement and developed and implemented strategies to improve response capability. In addition, lessons learned from the Fukushima incident were incorporated into a revised version of the Federal Nuclear Emergency Plan (FNEP), which Health Canada developed in collaboration with federal and provincial partners. The revised FNEP will be finalized in Fall 2012.
Program Activity 1.3: Official Language Minority Community Development
Official language minority community development involves the administration of Health Canada's responsibilities under Section 41 of the Official Languages Act, committing the federal government to enhancing the vitality of English-speaking and French-speaking minority communities, as well as fostering the full recognition and use of both English and French in Canadian Society and the provision of policy and program advice relating to the Act. Administration involves consulting with Canada's official language minority communities on a regular basis; supporting and enabling the delivery of programs and services; reporting to Parliament and Canadians on Health Canada's achievements under Section 41, and, in general, coordinating Health Canada's responses to the health needs of official language minority communities.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 39.3 | 39.4 | 39.4 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 12 | 9 | 3 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Increased number of health professionals available to provide health services in official language minority communities (OLMCs). | # of health professionals who successfully completed training programs (funded by Health Canada), by:
|
Francophones across Canada outside of Quebec: 1406 graduates over five years (281 annually). Anglophones in Quebec: Approximately 8000 health professionals completed second language training over five years (by March 31, 2013), an annual target of 1600. |
|
| Improved integration of OLMC health needs into the health system. | # of changes in legislative or public policies addressing the health needs of OLMCs (specify: type of change, purpose, OLMC need being addressed, location). | Presence of an integration plan for each area where there is a network and reports on the implementation and results achieved (by March 31, 2013). | In 2011-2012, only one or two minor changes were identified. This one-year observation is not sufficiently meaningful to assess status. |
Performance Summary
During 2011-12, there were 26 active contribution agreements as part of the Official Languages Health Contribution Program. Funding for recipients of the program totalled $38 million, and payments were made in a timely manner. Specific consultation activities included a national survey of French-speaking minority communities in eight provinces, to assess the health challenges they face, and a comprehensive consultation of Quebec's English-speaking communities regarding their health needs and priorities for the coming five years.
Health Canada funded 37 health networking organizations across all provinces and territories. These networks engaged community partnerships in improving health services, through such means as, informing provincial/territorial and regional health authorities of their needs, and implementing various projects to promote health and healthy lifestyles within their communities. There were 99 active projects in 2011-12. These health networks, through the joint commitments of partners, contributed to improving the organization of health services for English-speaking and French-speaking official language minority communities.
Lessons Learned
Health Canada organized a workshop on the state of health research for official language minority communities on August 31, 2011. The workshop looked at what should be done to understand the emerging and developing health needs of official language minority communities. The main message from this workshop was the importance of research activities to be collaborative; alliances formed between researchers and organizations can be more successful at improving health care than stand-alone research activities.
Strategic Outcome 2: Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating
This Strategic Outcome seeks to ensure that the food that Canadians eat and products they use are as safe as possible and that threats to health are addressed effectively. It helps increase Canadians' understanding of factors that influence everyone's health such as environmental conditions and nutrition. It helps to limit the use and abuse of tobacco and illicit drugs.
- Program Activity 2.1 : Health Products
- Program Activity 2.2 : Food Safety and Nutrition
- Program Activity 2.3 : Environmental Risks to Health
- Program Activity 2.4 : Consumer Product Safety
- Program Activity 2.5 : Substance Use and Abuse
- Program Activity 2.6 : Radiation Protection
- Program Activity 2.7 : Pesticide Safety
Program Activity 2.1: Health Products
This Program Activity is responsible for regulating a broad range of health products that affect the everyday lives of Canadians. Under the authority of the Food and Drugs Act and its Regulations, and the Department of Health Act, the Program Activity evaluates and monitors the safety, quality and efficacy of human and veterinary drugs, biologic and genetic therapies, radio-pharmaceuticals, medical devices, and natural health products so that Canadians have access to safe and effective health products. This Program Activity also verifies that, through compliance monitoring and enforcement activities, regulatory requirements for health products are met. In addition, the program provides timely, evidence-based and authoritative information to key stakeholders including, but not limited to, health care professionals such as physicians, pharmacists, natural health practitioners and members of the public to enable them to make informed decisions about the use of health products.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 168.3 | 177.3 | 177.2 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 2,292 | 1,896 | 396 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Increased awareness of the benefits and risks associated with the use of health products. | % of the target population aware of the benefits and risks associated with the use of health products. Examples include, but are not limited to:
|
Annual increases. | Public Opinion Research is not undertaken on an annual basis and was not conducted on Health Products in 2011-12. |
| Timely regulatory decisions for health products. | % of regulatory decisions made within service standards by type (Pre-market submissions): | Pharmaceutical drugs human – 90%; | Supplemental New Drug Submission (SNDS) (97%), Application for a Drug Identification Number - Disinfectant Product (DIND) (100%), Clinical Trial Application (CTA) (100&90%) and Clinical Trial Application Amendments (CTA-A) (100&94%) review decisions within performance standards. New Drug Submission (NDS) (89%) review decisions within performance standards. Drug Identification Number Applications (DINA) (67%). Abbreviated New Drug Submission (ANDS) (17%), Supplemental Abbreviated New Drug Submission (SANDS) (51%), and Notifiable Change (NC) (56%) review decisions. |
| Pharmaceutical drugs veterinary – 90%; | Regulatory decisions made within service standards - 89%. | ||
| Biologics and radiopharmaceuticals 90%; | Regulatory decisions made within the service standard for NDS, SNDS, and Drug Identification Number Biologics (DIN-B) applications -100%. | ||
| Medical devices – 90% | Investigational Testing (ITA) (92%) review performance. Class II (74%), III (80%) and IV (80%) review performance. |
||
| Natural health products – Product Licence Applications (PLAs): 90%, and Clinical Trial Applications (CTAs): 90%. | The Natural Health Products program surpassed submission review performance for Product License Applications and were on target for processing clinical trial applications. | ||
| Timely regulatory response for health product risks. | % of compliance/ surveillance activities reviewed within service standards by type:
|
96% of drugs establishment licenses and 91% of medical devices establishment licenses completed within service standards. | Inspections for pharmaceuticals, medical devices, and biologic companies met the planned number of 1165. |
Post-market safety assessments:
|
Completed - 90%. | post-market signal assessments (pharmaceuticals, medical devices, biologics, and natural health products) completed within service standards -93%. |
Performance Summary
Health Canada made considerable progress toward regulatory modernization, with the development of new policies and guidance documents. This included the development of new regulations, e.g.:
- Blood Regulations;
- Medical Devices Quality Management System Regulations; and,
- Class II Medical Devices Labelling Regulations.
Health Canada also developed new policies and guidance documents, e.g.:
- Bioequivalence Standards and Conduct of Bioequivalence Studies guidance document;
- Post-Notice of Compliance (NOC) Changes: Quality Document, and;
- Product Monograph Part III Plain Language guidance document.
Health Canada is currently improving its use of foreign regulatory information for health products, including foreign reviews, to be more efficient and systematic in its departmental marketing authorization review processes. Health Canada initiated the use of foreign reviews to accelerate the processing of generic drug submissions. The Program also explored the use of foreign reviews/approvals of post-authorization changes.
Updated User Fee Regulations came into force April 1, 2011. One hundred percent of first decisions met service standards in all cost recovery program areas. It is important to note that Health Canada is required to report submission review performance against current standards in place and by new standards under the new regulations. Specific to the new regulations, all fee categories and fee lines are subject to penalty if performance standards are not met. All applications are closely monitored and, where necessary, actions are taken to confirm that targets and/or penalty thresholds are not exceeded.
Lessons Learned
To improve the timeliness of regulatory decisions and so that priorities are met, the Medical Devices Program, implemented workflow efficiencies, updated processes to receive foreign reviews from other regulators, and enhanced internal systems.
Management of backlogs continued to be a challenge, primarily due to backlogs carried over from the previous year and an increase in the number of submissions received. Work to improve performance and reduce the backlog in generic drug submissions progressed through the addition of review staff, which increased the number of reviews being completed per month. The total backlog (all reviews and iterations) for Abbreviated New Drug Submissions and Supplemental Abbreviated New Drug Submissions in human pharmaceuticals is currently 57% of the workload. Over the last three months of the fiscal year, the program was averaging 31 completed reviews per month which is a significant increase in productivity. The Medical Devices Program did not meet the 90% on time target for Class II, III and IV applications also due to the previous year's backlog.
Program Activity 2.2: Food Safety and Nutrition
The Food Safety and Nutrition program activity establishes policies, regulations and standards related to the safety and nutritional quality of food. Food safety standards are enforced by the Canadian Food Inspection Agency and the Program Activity assesses the effectiveness of CFIA's activities related to food safety.The legislative framework for food is found in the Food and Drugs Act and Regulations, the Canadian Food Inspection Agency Act and the Department of Health Act. The Program Activity also promotes the nutritional health and well-being of Canadians by collaboratively defining, promoting, and implementing evidence-based nutrition policies and standards. As the focal point and authoritative source for nutrition and healthy eating policy and promotion, the Program Activity disseminates timely, evidence-based, and authoritative information to Canadians and stakeholders to enable them to make informed decisions and healthy choices.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 57.8 | 68.0 | 67.9 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 537 | 538 | 1 |
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Improved healthy eating by Canadians | % change in eating/ dietary practices of Canadians over time. | 20% increase from current value (42% of Canadians aged 18 and older reported that they consumed fruits and vegetables five or more times a day) by March 31, 2015. | The most current data from 2010 indicates that 42.6% of Canadians aged 18 and older reported that they consumed fruit and vegetables five or more times per day. |
| Responsiveness to external triggers related to nutritional and food safety risks through timely regulatory response and non-regulatory initiatives | % of Health Risk Assessments (HRAs) conducted at Canadian Food Inspections Agency's (CFIA) request addressed and communicated to stakeholders within Service Standards. | 100% of HRAs at CFIA's request within time standards by March 31, 2013. | 100% of HRAs requested by CFIA conducted within time standards. |
| Increased awareness of Canadians on the benefits and risks related to food safety, nutrition and healthy eating | % of the target population aware of benefits and risks related to food safety, nutrition and healthy eating over time. | For food safety awareness, as described in the ‘Survey of Canadians,' knowledge & behaviour related to Food Safety' research was last conducted in February 2010. For nutrition and healthy eating, this target is to be reached by March 31, 2013. |
A Nutrition Facts Education Campaign is presently ongoing which aims to increase consumers' knowledge and use of the % Daily Value (%DV) on packaged food labels. (Note: POR is not undertaken annually and was not conducted in 2011-12.) |
Performance Summary
The Food and Nutrition Program accomplished significant milestones on key files in 2011-12. The Nutrition Facts Education Campaign year two activities were launched. Health Canada worked with Canadian Food Inspection Agency, Privy Council Office and various government partners to develop targeted amendments to the Food and Drugs Act to support the modernization of Canada's food safety legislative framework. These amendments will provide more flexible tools that support risk-based approaches and alignment to the international framework. In addition to regulations, a number of guidelines were developed, and stakeholders continued to be engaged in food safety and nutrition matters.
The program activity also assesses the effectiveness of the Canadian Food Inspection Agency's (CFIA) activities related to food safety. During 2011-12, Health Canada completed assessment reports of CFIA activities related to food safety in Shell Eggs and Hatchery.
Health Canada updated its risk management approach for Caffeinated Energy Drinks and in October 2011, announced the transition of energy drinks to the food regulatory framework. Health Canada proposed a multifaceted approach that will use a range of complementary tools, regulatory and non-regulatory, that will help Canadians make informed decisions about these products, reducing the chances of over consumption of caffeine and other ingredients such as vitamins. New labelling requirements will also make it easier for parents to monitor the caffeine intake of their children and teens. This transition was the first step of a phased in approach aimed at providing appropriate risk-based regulatory oversight for products that are at the boundary between natural health products and food.
The Food Safety Program collaborated with the World Health Organization, the Food and Agriculture Organization of the United Nations, and the Government of Japan to host two Expert Consultations on Vibrio parahaemolyticus and Vibrio vulnificus in Seafoods and Salmonella in Bivalve Molluscs. The expert consultations supported continuing microbial risk assessments of pathogenic vibrios in seafood. This internationally led endeavour helped to advance Health Canada's own risk assessment and risk management approaches.
Lessons Learned
As a result of strong collaboration across government and with the agri-food and health sectors, the Government has met its commitments to reduce food safety risks, enhance surveillance and early detection of foodborne pathogens and illnesses, and improve emergency response, as reported in the Action On Weatherill Report Recommendations to Strengthen the Food Safety System: Final Report to Canadians. Part of the lessons-learned resulting from the 2008 Canadian deli-meat listeriosis outbreak was the development of a general guidance document for use primarily by federal level decision makers during foodborne outbreak investigations. This document provides information on factors to consider in determining the weight to assign when assessing evidence obtained from microbiological, epidemiological and food safety investigations.
Program Activity 2.3: Environmental Risks to Health
The environment continues to be a key determinant of health for all Canadians. This Program Activity aims to promote and protect the health of Canadians by identifying, assessing and managing health risks posed by environmental factors. The scope of activities includes: providing expert advice on the health impacts of climate change, air quality, drinking water quality and contaminated sites; research on and monitoring of chemicals and air quality; regulatory activities including risk assessment and management of chemical substances, products of biotechnology and products of other new and emerging technologies (including nanotechnology); and, working with the passenger conveyance industry to protect the health of the travelling public.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 48.1 | 119.4 | 105.1 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 544 | 761 | 217 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Threats to the health of Canadians posed by environmental risks are reduced | Trend data show improvements in air quality and health benefits. | Baseline for air quality and health benefit improvements to be set in 2013-14. Following that, air quality and health benefit improvements will be reported every three years, by percentage change over the period. | An air health indicator (AHI) was developed for ozone and for fine particulate matter to monitor trends in cardio-respiratory mortality due to exposure to each of these air pollutants in the Canadian population. Subsequent work focused on analyzing data to develop a morbidity-based AHI. The AHI also provides some of the input to inform the Air Quality Health Index and the Air Quality Benefits Assessment Tool. |
| Trend data demonstrate increased development and application of adaptation strategies to address health risks from climate change. | A minimum of five new communities adopt and implement a heat alert and response system to address the health risks from climate change over a five year period. |
|
|
| Level of exposure to substances of concern. | Program is currently working to establish new targets based on baseline established in 2010. | Canadian Health Measures Survey (CHMS) Cycle 1 data was released. Determination of Cycle 1 list of Substances of Concern completed and related exposure data analysis for baseline setting is ongoing. Anticipate setting of baselines for Substances of Concern by July 2012. |
Performance Summary
The Chemicals Management Plan, first launched in 2006, successfully initiated its second phase in 2011, whereby progress was made towards the 2015-16 goal of assessing, and where appropriate initiating the management of, some 1500 of 3000 remaining priority chemicals to be addressed by 2020.
Under the Clean Air Regulatory Agenda, research and assessment continued to provide the health basis and guidance for actions to reduce the health risks from indoor and outdoor air pollutants. Preparatory work was conducted with Environment Canada, the provinces and territories, and stakeholders, to lead to the adoption of a new national framework for managing air quality, including proposed new Canadian ambient air quality standards.
The Air Health Indicator (AHI), developed under Environment Canada's Canadian Environmental Sustainability Indicators (CESI) initiative, helps to monitor trends in mortality and morbidity resulting from exposure to air pollution. This indicator is designed to help identify which air pollutants are associated with health risks, to monitor changes in health risks over time and space, and to track the effectiveness of air quality management actions aimed at reducing adverse health effects in the Canadian population. The ozone AHI shows an upward trend in cardiopulmonary mortality attributable to ozone exposure. The fine particle (PM2.5) AHI shows no upward or downward trend in cardiopulmonary mortality. In July 2011, a summary of the AHI was posted to the CESI portion of Environment Canada's website, under Impacts of Air Pollution.
The Heat Resiliency Project continued to inform and advise public health and emergency management officials, public health professionals and Canadians on adaptation strategies to respond to extreme heat events. Accomplishments included the expansion of heat alert and response systems to at-risk regions across Canada; providing training for health professionals on the health impact of heat; and dissemination and outreach in support of the guidance documents that were released in 2011-12.
Four guidance documents were approved by the federal/provincial/territorial Committee on Health and the Environment and two tools developed to help identify threats to safety of drinking water and strategies to reduce these risks. In collaboration with the Public Health Agency of Canada (PHAC), the development of the Drinking Water Advisory Module continued. This is a real-time notification and information-sharing tool for public health and drinking water authorities that capture key information on drinking water advisories from Canadian jurisdictions. This unique application permits analyses and reporting on key trends and root causes of advisories across Canada and is currently being used or set up in a number of jurisdictions.
Lessons Learned
Air and water quality management requires participation of all levels of government, industry, and the general public. All partners are essential in bringing their unique expertise and perspective to the process. Close internal and external collaboration is essential to advance research in a timely manner. For instance, collaborative processes between federal, provincial and local governments involving a wide range of stakeholders have been the key to developing heat alert and response systems, a new national framework to manage air quality, and to implementing the Air Quality Health Index across the country.
Federal Sustainable Development Strategy (FSDS) Targets Led by Health Canada
| FSDS Goals | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Air Pollution: Minimize the threats to air quality so that the air Canadians breathe is clean and supports healthy ecosystems. | Levels of exposure to substances of concern by substance. *Canadian releases of selected controlled substances. |
Chemicals Management Reduce risks to Canadians and impacts on the environment posed by harmful substances as a result of decreased environmental concentrations and human exposure to such substances. |
|
| Health-based assessments of priority indoor air pollutants and associated management tools (# of indoor air and CMP priority indoor pollutant assessments, guidelines, building or product standards). | Help protect the health of Canadians by assessing indoor pollutants and developing guidelines and other tools to better manage indoor air quality. | Risk assessments were conducted and new Residential Indoor Air Quality Guidelines were developed for priority indoor pollutants toluene and fine particulate matter (PM), including recommendations on how to reduce exposure and protect health. The final Residential Indoor Air Quality Guideline for toluene was issued, and the proposed PM2.5 guideline was published for public comment in Canada Gazette, Part 1. Indoor air quality was also a primary focus of Health Canada's Hazardcheck outreach campaign. | |
| Water Quality: Protect and enhance the quality of water so that it is clean, safe and secure for all Canadians and supports healthy ecosystems. | Drinking Water Quality: Health-based water guidelines (# of water guidelines/guidance documents approved by F/P/T Committee by product type.) | Help protect the health of Canadians by developing health-based water guidelines. | Four guidelines/guidance documents have been approved by the F/P/T Committee on Health and Environment:
|
| *Percentage decrease of concentrations of selected substances— perfluorooctane sulfonate (PFOS) and polybrominated diphenyl ethers (PBDEs)—in water from baseline data. | Chemicals Management Reduce risks to Canadians and impacts on the environment posed by harmful substances as a result of decreased environmental concentrations and human exposure to such substances.* |
|
|
|
Table 1 footnotes
|
|||
FSDS Performance Summary
Health Canada responsibilities related to air, water, climate change and chemicals management contributed significantly to the Federal Sustainable Development Strategy (FSDS) in 2011-12. Under the Chemicals Management Plan, Health Canada assessed the health risks of new and existing chemicals and developed risk management strategies, where needed. Health Canada also responded to stakeholder inquiries and added to the awareness of Canadians about what they can do to reduce risks. Health Canada continued to work in partnership with provinces and territories to safeguard drinking water supplies in Canada by developing the Guidelines for Canadian Drinking Water Quality. Recognizing the link between air quality and health, Health Canada continued to support the Government's Clean Air Agenda (CAA). Health Canada, along with Environment Canada, worked with the provinces and territories and other key stakeholders to prepare a new national framework for managing air quality, including proposed new Canadian ambient air quality standards. Key elements of the framework are to be finalized in 2012.
The AQHI was expanded to more communities in 2011-12, making the AQHI available to 60% of all Canadians, and increased awareness of the index through marketing and targeted outreach to sensitive populations. Health Canada continued to provide Canadians with the information they need to achieve healthy indoor environments, through Residential Indoor Air Quality Guidelines, the Hazardcheck: Hazards in Your Home campaign, and the national Radon awareness program.
Program Activity 2.4: Consumer Product Safety
Health Canada is committed to promoting the health and safety of Canadians by working to improve the safety of consumer products in the Canadian marketplace. Under the Consumer Product Safety Program Activity, Health Canada works to identify, assess, manage and communicate to Canadians the health and safety risks associated with consumer products that adults and children commonly use for personal, family, household or garden purposes, or in recreation or sports. This is achieved through active prevention, targeted oversight and rapid response, all of which are supported by the Canada Consumer Product Safety Act.
Through active prevention, Health Canada worked with industry to help proactively identify and systematically assess safety risks posed by consumer products, develop standards and share best practices. Also, the Program Activity promotes awareness of new policy and regulatory activity, and provides guidance to industry on existing regulations through guidance documents, workshops and training. Through targeted oversight, the program keeps a close watch on products for which the risks are not yet fully understood or that pose the greatest potential risk to the public. Under rapid response, Health Canada can act quickly to protect the public when a problem occurs – including ensuring the removal of unsafe consumer products from store shelves.
Through this Program Activity, Health Canada confirms that cosmetic products used by Canadians on a daily basis are safe and meet the requirements set out in the Food and Drugs Act and its Cosmetic Regulations. Publishing the Cosmetic Ingredient Hotlist of Prohibited and Restricted Cosmetic Ingredients and requiring ingredients to be listed on outer product labels allows Canadians to make informed decisions when selecting and using cosmetics.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 28.0 | 32.7 | 27.7 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 246 | 212 | 34 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Increased consumer/industry awareness of health risks and regulatory requirements related to consumer products | % by target population aware of information related to consumer and product safety and related to exposure to consumer products by:
Note: Public Opinion Research (POR) was completed in 2011-12 to explore awareness, attitudes and knowledge as they relate to Consumer Products. |
On-going target to maintain industry awareness levels – to be measured using surveys distributed after speaking engagements with industry stakeholders. |
Industry
|
| Responsive regulatory system for consumer products | % of regulatory actions addressed within service standards (SS) and targets set (TS) by:
|
The Canada Consumer Product Safety Act (CCPSA), including the provision for mandatory incident reporting, did not come into force until June 20, 2011. The baseline will be established by early 2013. | Data collection for this area will begin in 2012-2013. |
| Improved industry compliance with product safety obligations | % and # of inspected registrants/firms/users that are compliant / non-compliant with standards/acts/regulations/ guidelines by:
|
100 % of cyclical enforcement projects completed within prescribed timelines. | Completed in 2011-12, the cycle targeting six regulated product categories with identified hazards and baseline data:
|
Performance Summary
In 2011-12, the Consumer Product Safety (CPS) Program's regulatory activities focused on putting in place the necessary mechanisms for the implementation of the Canada Consumer Product Safety Act (CCPSA), including initiating the development of regulations for administrative monetary penalties. The proposed Administrative Monetary Penalties (AMP) Regulations were published in the Canada Gazette, Part I in March 2012.
CPS successfully launched the consumer product incident reporting system to support the new mandatory incident reporting requirements for industry under the CCPSA. Incident reports are tracked outside of Health Canada for products in the international market and management and compliance responses are taken as needed. This includes simultaneous access and coordinated activity by regional inspectors, central policy makers and senior management/decision makers.
CPS developed an industry outreach plan to increase industry's awareness of the new CCPSA, particularly new requirements for mandatory incident reporting and record keeping. CPS successfully communicated key messages to thousands of industry stakeholders regarding the new modernized provisions of the CCPSA, increasing awareness of their obligations. Awareness surveys were conducted before and after the industry information sessions to assess the level of success.
When there is a concern with a product, consumers are informed quickly through recalls and advisories posted on the Health Canada website. This information is intended to allow consumers to make appropriate safe choices when using consumer products or cosmetics. During 2011-12, Health Canada used social media to inform Canadians of the 20 advisories and 249 recalls issued related to consumer products. These advisories and recalls were the result of various activities including: planned compliance and enforcement activities; mandatory incident reports from industry; voluntary incident reports from consumers; and information sharing with other jurisdictions such as the United States.
Lessons Learned
The rapid implementation schedule for the CCPSA led to adjustments in work plans throughout the Consumer Product Safety program to provide that Health Canada was well prepared for the coming into force date of June 20, 2011. This led to some work plans being revised as available resources focused on the CCPSA implementation.
Program Activity 2.5: Substance Use and Abuse
Through regulatory, programming and educational activities, Health Canada seeks to improve health outcomes by reducing and preventing tobacco consumption and combating alcohol and drug abuse. Through the Tobacco Act and its regulations, Health Canada regulates the manufacture, sale, labelling, and promotion of tobacco products. It also leads the Federal Tobacco Control Strategy – the goal of which is to further reduce the prevalence of smoking through regulatory, programming and educational activities. Through the Controlled Drugs and Substances Act (CDSA) and its regulations, Health Canada regulates controlled substances. As a partner department under the National Anti-Drugs Strategy, Health Canada supports prevention, health promotion, and treatment initiatives with the goal of reducing substance use and abuse and its associated harms. It also provides expert advice and drug analysis services to law enforcement agencies across the country.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 139.1 | 142.2 | 123.0 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 432 | 417 | 15 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Declining levels of substance use and substance abuse | Rates of substance use and abuse:
|
12% of Canadians 15 years and up; 9% youth (15-17). | Based on the most recent available data from the 2010 Canadian Tobacco Use Monitoring Survey (CTUMS), 17% of Canadians 15 years of age and up and 9% of Canadian youth (15-17) were current smokers. * CTUMS 2011 results will be released in September 2012. |
Levels of drug abuse in Canada
|
It has been determined that national targets are not applicable as policy and programs influencing the prevalence of illicit drug use primarily fall under the jurisdiction of Provinces and Territories. | Based on the Canadian Alcohol and Drug Use Monitoring Survey (CADUMS) 2011:
|
|
| Increased Compliance/Adherence to Tobacco Act and Regulations, and Controlled Drugs and Substances Act and Regulation | % of inspections that are compliant (C) / non-compliant (NC) with acts, regulations, or other control instruments by:
|
100% of inspections are compliant with the acts, regulations, or other control instruments by:
|
98% of Class A precursor licensed dealers that were inspected were found to be compliant. Since 2007-08, over 98% of the Class A Licensed Dealers had been inspected. |
Performance Summary
Health Canada continued to inform Canadians on the hazards and risks to health associated with alcohol, tobacco, controlled and illicit substances and precursors. There continues to be a decline in the levels of substance use and abuse in Canada.
The Government of Canada renewed the Federal Tobacco Control Strategy (FTCS) through Budget 2012. Smoking is at an all-time low in Canada, with smoking rates dropping to an historic low of seventeen percent. The number of Canadians who smoke on a daily basis is even lower at thirteen percent. The program introduced new graphic warning labels on cigarette packages and a pan-Canadian quit line phone number on and web portal on tobacco packages for people who want help quitting.
The program implemented a new compliance and enforcement plan for the Act to Amend the Tobacco Act addressing the key elements of minimum packaging restrictions and advertising prohibition of certain additives in cigarettes, little cigars and blunt wraps.
Under the leadership of Justice Canada, the National Anti-Drug Strategy (NADS) has made significant progress in achieving results in the implementation of best practices, enhancing knowledge exchange, and strengthening performance measurement and evaluation. Services projects supported new and enhanced treatment services for at-risk youth and for those living in Vancouver's Downtown Eastside.
The DrugsNot4Me/0droguepourmoi campaign continued to increase the awareness of the harms associated with illicit drug use, within youth ages 13-15, through a mix of traditional and social media initiatives. The Facebook page attracted over 87,000 fans and the DrugsNot4Me website obtained over one million visits. The "Pick Your Path" series of YouTube videos garnered astonishing uptake, with over 373,000 video views in just a few short weeks. Most youth (84%) recalled seeing campaign advertisements, and 20% of youth who saw the advertising took action as a result (e.g. visited the website, talked with friends/family, decided not to do drugs).
The program employed a risk-based model for controlled substances inspections, completing 187 inspections. In 2011-2012, only 2% of Class A precursor dealers inspected were non-compliant. For those, follow-up measures, including issuing monitoring letters, initiating correction actions and applying conditions to a licence were undertaken.
The Marihuana Medical Access Program (MMAP) improved responses to clients, and issuance of authorizations to possess, and licences to produce, marihuana for medical purposes, with the support of a physician.
Lessons Learned
In regards to the Marihuana Medical Access Program, Health Canada has benefitted from the input of stakeholder groups following extensive consultations throughout the year. Health Canada made significant improvements in restoring and improving upon service standards to program clients. This was achieved through improved and centralised operations, additional and well-trained staff, and an improved database.
Program Activity 2.6: Radiation Protection
Health Canada aims to reduce the health and safety risks associated with different types of radiation, both naturally occurring and from man-made sources, in living and working environments. Health Canada conducts research into the biological effects of environmental and occupational radiation, develops better methods for radiation dosimetry and its measurement, provides radiation safety inspections of federally regulated facilities containing radiation-emitting devices, develops regulations, guidelines, standards and safety codes pertaining to radiation-emitting devices, and provides radiation advice to other government departments, industry and the general public.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 1.8 | 14.0 | 14.0 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 82 | 152 | 70 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Increased public/stakeholder awareness of health risks related to radiation/radon | % and # of Canadians aware or knowledgeable of information and health risks related to radiation/radon by:
|
30% of Canadians. Note: Indicator being revised as public opinion research in this area is not currently planned. |
Radon brochure distribution increased by approximately 15% in 2011-12. Radon web activity (webpage hits and downloads) and public inquiries increased only marginally (5-10%) in 2011-12 compared to previous years. |
| Increased compliance/adherence to radiation emitting devices acts and regulations, and Canadian Nuclear Safety Commission acts and regulations | % of inspected registrants/firms/users that are compliant/non-compliant with acts, regulations, or other control instruments by:
|
At least 75% of inspected devices are compliant with the acts, regulations, or other control instruments by:
|
In 2011-12, completed:
|
| Declining Level of Illnesses and Injuries from 'Exposure to Radiation in the Environment | Incidence/rate of illness/risk related to exposure to radiation in the environment by:
|
Baseline to be established by March 31, 2013. | To be determined once baseline has been established. |
Performance Summary
The Canadian Radiological Monitoring Network (CRMN) operates 100 stations that monitor radioactivity in the air, water, and food. All stations were operational over 90% of the time, down only for brief periods for maintenance activities.
In support of the Federal Sustainable Development Strategy (FSDS) and the Clean Air Agenda (CAA), Health Canada tested radon levels in approximately 2000 high priority federal buildings in high-risk, radon-prone areas in 2011-12, and is currently on track towards meeting the target of testing 10,000 high priority buildings by the end of 2012-13. In support of the National Radon Awareness Campaign, radon brochure distribution increased by 15% and radon web activities and public inquiries increased between 5% -10% as compared to 2010-11. Health Canada also published the Cross-Canada Survey of Radon Concentrations in Homes, which includes the results of a two year study conducted by the Departmental National Radon Program.
Also in support of the Strategy, the Program delivered radon education and awareness products, including:
- A radon sniffer's fact sheet posted on the web and delivered via Physicians Hotline.
- Web posting the new radon flash presentation: “Radon what you need to know” and Canadian mitigation guide entitled, “Reducing Radon Levels in Existing Homes: A Canadian Guide for Professional Contractors”.
- A proactive regional radon media campaign.
- A national webinar on reducing radon in Canadian homes with over 230 participants.
Lessons Learned
Testing for radon is best done during the fall and winter heating season thus limiting the amount of time available to achieve the target. Meeting the target of 2,000 federal buildings tested for radon was dependent on the co-operation of other government departments. The importance of early engagement and coordination proved successful as the majority of the detectors have completed the three-month testing period.
Program Activity 2.7: Pesticide Safety
Health Canada, through the Pest Management Regulatory Agency, administers the Pest Control Products Act (PCPA) and its regulations. The primary objective of the PCPA is to prevent unacceptable risks to people and the environment from the use of pest control products. Health Canada regulates the entire life cycle of a pesticide, including: determination of value, health and environmental risk assessment, characterization and mitigation, registration of products, monitoring and enforcement activities, re-evaluation of registered pesticides on a 15-year cycle, and phase-out or cancellation of products. Pest control products are regulated in a manner to encourage the development and implementation of innovative, sustainable pest management strategies and to facilitate access to pest control products that pose lower risks. Health Canada also encourages public awareness in relation to pest control products by informing the public, facilitating access to relevant information and participating in the decision-making process. Health Canada plays a leading role in international efforts to integrate various regulatory systems around the world. International cooperation facilitates consistency and ensures that the best science available supports our decision making.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 34.1 | 48.1 | 46.8 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 499 | 474 | 25 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Prevention of unacceptable risk from pesticides | As a result of regulatory decisions:
|
Annually. |
|
| Timely regulatory decisions for pesticides | % of reviews conducted within service standards and targets set for:
|
|
|
| Mitigation of risks of/from non-compliance associated with pesticides | # and % of registrants/vendors/users, within a sector, found to be non-compliant that have returned to compliance (i.e., risks are mitigated) by:
|
|
|
Performance Summary
Through the Pesticide Safety program activity, Health Canada continued its ongoing responsibilities under the Pest Control Products Act through evaluation and re-evaluation of pesticide products as well as compliance, enforcement and risk reduction strategies. These approaches support an overall commitment to modernizing pesticide safety. Health Canada made a total of 2,560 regulatory decisions on various categories of pesticide submissions.
In September 2011, Health Canada hosted the First International Conference for Heads of Pesticide Regulatory Authorities in Ottawa, providing a forum to discuss global collaboration on pesticide regulation. Health Canada continued its leadership in the area of global joint reviews. This is the formal process whereby the review of the science data which supports the registration of a pesticide is split among a number of countries.
Collaboration with international partners also allowed Canada to remain in the forefront of pesticide regulatory science. For example, through the OECD Working Group on Pesticides, Health Canada co-led and contributed to a number of key issues. These included the development of an electronic standard for exchanging pesticide data and information, contributing to the science of pesticide residue chemistry in foods, key science issues related to pollinators, and the establishment of a global compliance network.
Furthermore, under the Canada - United States Regulatory Cooperation Council Initiative, Health Canada worked to facilitate equal access to pest control products and uses. Building on a long-standing history of cooperation in the area of pesticide regulation, further alignment could facilitate simultaneous access to effective production tools and technologies while protecting human health and the environment.
The implementation of the Food and Consumer Safety Action Plan succeeded in meeting all Year 4 commitments. Funding under the Plan enabled Pest Management Regulatory Agency to deliver compliance programs and projects during this reporting period. Significant active prevention and inspection activities were conducted for several sectors, including flea and tick spot-on products, pool and spa, rental properties, vendors, and seasonal worker programs.
New measures were introduced on approved pesticides as a result of the re-evaluation program, to reduce the risks to children and pets and non-target species. For example, rodenticides used by individual consumers must be placed in tamper-proof bait stations. Outreach materials were produced to alert consumers of the new mitigation measures.
Lessons Learned
Increased international collaboration with partners has contributed to finding efficiencies and standardized global approaches. Best practices are identified, with knowledge and experience transfer an important benefit.
Strategic Outcome 3: First Nations and Inuit communities and individuals receive health services and benefits that are responsive to their needs so as to improve their health status
This Strategic Outcome seeks to ensure that First Nations and Inuit living on reserve or in Inuit communities have access to health services as well as a limited range of medically necessary health-related goods and services not provided through private insurance plans, provincial/ territorial health or social programs or other publicly funded programs. It seeks to reduce the gap in health outcomes between First Nations and Inuit and the Canadian population in general.
- Program Activity 3.1 : First Nations and Inuit Primary Health Care
- Program Activity 3.2 : Supplementary Health Benefits for First Nations and Inuit
- Program Activity 3.3 : Health Infrastructure Support for First Nations and Inuit
Program Activity 3.1: First Nations and Inuit Primary Health Care
The Primary Health Care Activity funds a suite of programs, services and strategies provided primarily to First Nations and Inuit individuals, families and communities living on-reserve or in Inuit communities. It encompasses health promotion and disease prevention programs to improve health outcomes and reduce health risks, public health protection, including surveillance, to prevent and/or reduce human health risks associated with communicable diseases and exposure to environmental hazards, and primary care where individuals are provided diagnostic, curative, rehabilitative, supportive, palliative/end-of-life care and referral services.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 940.0 | 957.8 | 949.1 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 1,301 | 1,385 | 84 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Primary health care programs and services that are responsive to the needs of First Nations and Inuit individuals, families and communities. | Immunization coverage rates for two and seven year old children living on-reserve. | 95% of all provincially scheduled childhood immunizations by March 2016. | While 2011-12 data is not yet available, progress continued toward the March 31, 2016, target of 95% coverage for provincially supported vaccines among two and seven year olds living on-reserve. |
| % of on-reserve population receiving required primary care assessment/ diagnostic, treatment, rehabilitative, supportive and palliative care services. | Maintain service levels (Service level is 290/1000 population or 29%). | Service levels maintained. Clinical client care on-reserve services utilization ratio was 294.4/1000. In addition, 27,000 individuals were provided 2.6 million hours of home care services. | |
# and % of individuals, families and communities receiving required preventive, screening, treatment and support services for community-based health promotion/disease prevention programs by type of service:
|
Maintain service levels. (Baseline levels will be determined for service delivery measures for the 2012-13 reporting period.) |
Maintained service levels in mental wellness, healthy child development and healthy living programs. |
Performance Summary
Health Canada continued to focus on the implementation of health promotion and disease prevention programs to support individuals, families and communities in addressing health priorities related to healthy living, mental wellness and healthy child development.
In support of healthy living, funding for the Aboriginal Diabetes Initiative has enabled First Nations and Inuit communities to build on past successes in more than 673 First Nations and Inuit communities throughout Canada.
Contributing to mental wellness, Health Canada supported First Nations and Inuit communities to reduce risk factors, promote protective factors, and improve health outcomes:
- The National Aboriginal Youth Suicide Prevention Strategy funded projects in approximately 150 Aboriginal communities.
- The National Native Alcohol and Drug Abuse Program (NNADAP) and the National Youth Solvent Abuse Program (NYSAP) supported a network of 58 First Nations addiction treatment centres and more than 550 prevention programs in First Nations communities.
- With funding from the National Anti-Drug Strategy, Health Canada worked to improve the quality, accessibility and effectiveness of addictions services for First Nations and Inuit:
- The percentage of certified addiction treatment counselors increased to 77%, up from 68% in 2010-11, and 82% of treatment centres were accredited, up from 74% in 2010-11.
- Eight multi-disciplinary, mental wellness teams were supported in First Nations and Inuit communities across Canada. Mental wellness teams are community-based and provide clinical and cultural services.
- Honouring Our Strengths: A Renewed Framework to Address Substance Use Issues Among First Nations People in Canada was released in 2011, the result of a four-year, comprehensive review of NNADAP, undertaken in partnership with the Assembly of First Nations and the National Native Addictions Partnership Foundation. The framework supports a strengthened approach to First Nations addiction prevention and treatment services based on community needs, including enhanced services for women, youth, illicit drug users and people with co-occurring mental health problems.
Health Canada supported a number of programs and services aimed at contributing to the health and social development of Aboriginal preschool children and their families.
- The First Nations and Inuit component of the Canada Prenatal Nutrition Program served more than 600 communities and reached over 9,000 First Nations and Inuit women per year.
- The Maternal Child Health Program provided home visits by nurses and family visitors to 2,221 women and families with young children, in 125 projects within approximately 225 First Nations communities.
- The Fetal Alcohol Spectrum Disorder Program established 36 mentoring sites across Canada and reached more than 600 women. In addition, there are 17 community coordinators to help increase families' access to multi-disciplinary diagnostic teams and related services and support.
- The Aboriginal Head Start on Reserve served over 9,000 children in over 300 First Nations communities across Canada.
- There was continued success for a national immunization social marketing campaign for First Nations and Inuit parents and caregivers.
Health Canada completed the development of the Strategy Against Tuberculosis for First Nations On-Reserve. The strategy was developed for First Nations tuberculosis programming and may be used as a reference tool for anyone involved in tuberculosis prevention and control for First Nations and Inuit in Canada. It is based on current evidence, best practices and lessons learned. The study, provides an additional focus on populations at greatest risk for tuberculosis such as people infected with HIV/AIDS and on the need for stronger partnerships among Aboriginal, federal and provincial authorities. Furthermore, an increased emphasis on performance measurement and evaluation will help track progress and allow programs to adapt accordingly.
Capacity in First Nation communities to manage public health emergencies has been strengthened, as 98% of First Nation communities now have a communicable disease emergency plan in place. Over 87% of these communities have tested and validated components of their plan. Health Canada is continuing to work jointly with communities to test components of their communicable disease emergency plan.
Lessons Learned
Health Canada continued to take actions to respond to the findings and recommendations of recent Primary Health Care Activity evaluations including:
- Home and Community Care Program Summative Evaluation (2009),
- Children and Youth Programs Cluster Evaluation (2010),
- Final Evaluation Report of the Labrador Innu Comprehensive Healing Strategy (2010),
- Communicable Disease Control Cluster Evaluation Final Report (2010),
- Chronic Disease and Injury Prevention Cluster Evaluation Final Report (2011), and, Environmental Health and Environmental Research Cluster Evaluation Final Report (2011).
As a result, for example, the following actions were taken:
- Updated First Nations and Inuit home and community care program standards to address human resource challenges (staff recruitment, retention, training, development and compensation), and a “Quality Handbook” was developed for monitoring the quality and efficiency of home and community care services in First Nations and Inuit communities;
- Funded seven demonstration and 21 community-based projects on diabetes prevention in urban communities;
- Completed strategies to support community development and capacity building within First Nations and Inuit communities, and strategies for integrating these health promotion and social marketing activities;
- Prepared and shared tools with communities to identify, prioritize and address health needs and to improve the continuum of programs and supports, e.g.:
- A popular report on the 2010 evaluation on children and youth programs and services;
- A newsletter on children and youth programs and services;
- A popular report of a Fetal Alcohol Spectrum Disorder special study; and
- Three technical reports on the Maternal and Child Health Implementation Review, Fetal Alcohol Spectrum Disorder Mentoring Special Study, and the Fetal Alcohol Spectrum Disorder Community Coordinator Pilot Review.
Given the complex inter-jurisdictional nature of health care, it is challenging to collect timely, accurate and relevant on-reserve health data. To address this challenge, Health Canada worked to establish appropriate data collection tools and surveillance systems to accurately capture and report on communicable disease issues (e.g. vaccine preventable disease incidence and immunization coverage rates).
The collaborative process used to develop the Honouring Our Strengths addictions framework has been described as a highly successful approach for program renewal and policy development with First Nations partners. This process was designed and governed as a partnership between Health Canada and First Nations. First Nations communities, service providers and leadership were engaged at every stage of the process. Health Canada is documenting this process in partnership with First Nations to serve as an engagement model for future similar efforts.
Federal Sustainable Development Strategy (FSDS) Targets Led by Health Canada
| FSDS Goals | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Water Quality: Protect and enhance the quality of water so that it is clean, safe and secure for all Canadians and supports healthy ecosystems. | Footnote * Drinking Water Quality: Percentage of First Nation communities with acceptable water and wastewater facility risk ratings. | Footnote * Increase the percentage of First Nation communities with acceptable water and wastewater facility risk ratings by 2013. | Per the 2012 Annual Performance Inspection results (June 29, 2012), compared to data on the same systems from the National Assessment results (July 11, 2011)Footnote **: Water systems:
|
|
|||
FSDS Performance Summary
Health Canada undertook a number of actions in key areas to address the stated government priorities as outlined in the Federal Sustainable Development Strategy (FSDS). Access to safe drinking water is important to the public health of First Nations and Inuit communities. Health Canada has continued to enhance capacity to monitor drinking water as per the Guidelines for Canadian Drinking Water Quality in First Nations communities. Health Canada also continued to implement the health promotion campaign on mould in support of the National Strategy to Address Mould in First Nations Communities led by Aboriginal Affairs and Northern Development Canada in an effort to increase capacity geared toward the effective prevention and/or remediation of mould in First Nation homes and community facilities.
Health Canada's 2011-2012 Sustainable Development Strategy Performance Report provides additional information.
Program Activity 3.2: Supplementary Health Benefits for First Nations and Inuit
The Non-Insured Health Benefits (NIHB) Program provides a specified range of medically necessary health-related goods and services to over 896,000 eligible registered Indians (according to the Indian Act) and Inuit (as recognized by one of the Inuit Land Claim Organizations in Canada) where not otherwise covered under a separate agreement (e.g. a self-government agreement) with federal, provincial or territorial governments. The benefits under the NIHB Program include the following, where not otherwise provided to eligible clients through private or provincial/territorial programs: pharmacy benefits (prescription drugs and some over-the-counter medication), medical supplies and equipment, dental care, vision care, short term crisis intervention mental health counselling, and medical transportation benefits to access medically required health services not available on reserve or in the community of residence.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 983.9 | 1,137.5 | 1,111.5 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 521 | 408 | 113 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Access to non-insured health benefits appropriate to the unique health needs of First Nations people and Inuit | % of FN/I population who accessed NIHB by type of benefit:
|
Maintain access levels according to medical necessity. |
|
| Efficient management of access to non-insured health benefits | Administrative cost ratio (ratio of administration costs to benefit expenditures). | Reduce to 6.0% over five years. | The administrative cost ratio was reduced to less than 5.0%. |
Performance Summary
The Non-Insured Health Benefits program continued to fund the provision of a limited range of medically necessary supplementary health benefits not already provided through other public or private plans, for over 896,000 eligible First Nations and Inuit. In 2011-12, approximately 650,000 individual clients (73%) accessed at least one medically required benefit. Health Canada made a concerted effort to identify opportunities and implement efficiencies in administrative processes, to reduce costs as well as to reduce demands on service providers (e.g. business case for electronic claims processing for vision care benefits, pharmacy auto-approvals for three selected drugs, and streamlining of the dental pre-determination process for endodontic treatment).
Through the Children's Oral Health Initiative, 260 communities received preventive and basic oral health care services, provided by either oral health aides, dental therapists or dental hygienists. Health Canada successfully expanded the Children's Oral Health Initiative to 80% of eligible children aged 0-4 (target was 40%) and to 56% of eligible children aged 5-7.
In response to findings of the NIHB program evaluation (Non-Insured Health Benefits Program Cluster Evaluation, Final Report, November 2010), Health Canada explored ways to further streamline dental pre-determination and pharmacy pre-approval processes. Health Canada began restructuring dental pre-determination by removing endodontic pre-determination and changed the dental compensation model under the NIHB program. Health Canada also identified other opportunities to increase administrative efficiencies, to reduce costs and demands on providers, such as pharmacy auto-approvals and the development of a business case for electronic claims processing of vision care benefits.
In addition, Health Canada expanded the Prescription Monitoring Program to all regions, except Quebec; continued the development of a standardized price file for select medical supplies and equipment and implemented a transition plan to integrate the new NIHB clients resulting from the McIvor case and the creation of the Qalipu Mi'kmaq Band in Newfoundland.
Lessons Learned
A number of software issues were identified with the current medical transportation data storage system, which prevented adequate data capture to better support management decision-making. These issues are being addressed through changes to the system architecture and data submission processes and better coordination between headquarters and regions of initiatives, leading to software development.
Program Activity 3.3: Health Infrastructure Support for First Nations and Inuit
The Health Infrastructure Support activity underpins the long-term vision of an integrated health system with greater First Nations and Inuit control by enhancing their capacity to design, manage, deliver and evaluate quality health programs and services. It provides the foundation to support the delivery of programs and services in First Nations communities and for individuals, and promotes innovation and partnerships in health care delivery to meet the unique health needs of First Nations and Inuit. The funds are used for: planning and management for the delivery of quality health services, construction and maintenance of health facilities, research activities, encouraging Aboriginal people to pursue health careers, investments in technologies to modernize health services, and integrate and realign the governance of existing health services.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 256.8 | 353.4 | 351.6 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 243 | 651 | 408 |
|
||
| Program Activity Expected Results | Performance Indicators | Targets | Actual Results |
|---|---|---|---|
| Promote innovative integrated health governance relationships | % of provinces/territories with multi-jurisdictional agreements to jointly plan, deliver and/or fund integrated health services for aboriginal Canadians. | 100% by March 2015. | Health Services Integration Fund: 27 multi-jurisdictional projects to integrate health services for Aboriginal Canadians were implemented across 7 of 13 provinces and territories. |
| Improved First Nations and Inuit capacity to influence and/or control (design, deliver, and manage) health programs and services | # of communities involved in the planning process to influence and/or control (design, deliver, and manage) health programs and services. | 5% increase (two to three communities) in the number of communities involved by 2016. | Eleven First Nation communities took on greater involvement in the planning process to influence and/or control (design, deliver and manage) health programs and services. They began work on Multi-Year Work Plans and Health Plans to enable them to move into funding agreements with greater flexibility. |
Performance Summary
Moving toward the long-term vision for the integration of federal and provincial health services for Aboriginal people, the British Columbia (BC) Tripartite Framework Agreement on First Nation Health Governance was signed on October 13, 2011. This legally-binding Framework Agreement was signed by the federal and provincial Ministers of Health and the BC First Nations Health Society, with endorsement from the BC First Nations Health Council. The first of its kind, this Framework Agreement will create a new province-wide First Nations Health Authority to take over First Nations health programs, services, and staff in BC. In addition, the Saskatchewan First Nations Health and Wellness Plan was drafted in consultation with the Province and the Federation of Saskatchewan First Nations Health and Wellness Plan Chiefs in Assembly.
Announced in 2010, the Health Services Integration Fund (HSIF) is a five-year, $80 million initiative supporting collaborative planning and multi-year projects aimed at better meeting the health-care needs of First Nations, Inuit and Métis. Implementation will occur in five phases. Each phase builds on the previous phases and supports the necessary building blocks for collaborative planning, project implementation, and evaluation. In 2011-12, Health Canada focused on planning (Phases 1 and 2), which included forming Advisory Committees on health services integration with adequate representation of provincial and Aboriginal partners in health. By March 2012, each province and territory had formed advisory committees.
Health Canada continued to harmonize the management of contribution agreements with Aboriginal Affairs and Northern Development Canada and other partners. While transitioning to new funding models, Health Canada implemented a transition strategy, which included an option for stakeholders to extend their existing agreements for a one year period.
Lessons Learned
Health Canada worked with HSIF Advisory Committees to assist in the development of Integration Plans. Twelve of these committees (92%) have submitted Integration Plans to the HSIF Secretariat. Integration plans draw on lessons learned from the Aboriginal Health Transition Fund (Meta-Evaluation [Summative Evaluation] of the Aboriginal Health Transition Fund, Final Report, March 2012) and elsewhere, and define future priority areas in integrating health services within the province or territory.

Internal Services
Health Canada has a range of internal services. Some, such as financial, administrative, real property, security, human resources, information management and Information Technology, provide the basic infrastructure that enables Health Canada to function while complying with central agency policies and laws.
Other internal services in Health Canada address departmental and Health Portfolio needs such as general communications and policy activities, the management of relations with Parliamentarians, the Cabinet system and other government departments and levels of government. An additional set of internal service roles centre on critical departmental and government-wide responsibilities, such as obtaining the best value for Canadians through planning, accountability and tracking performance and results.
Those responsible for internal services within Health Canada continue to focus on their ongoing responsibilities while continuing to build on the use of department-wide approaches in such areas as learning, Information Technology and information management. Many directly help to oversee, deliver or support management priorities. In addition to those efforts, Health Canada addresses specific issues and opportunities that arise.
| Planned Spending | Total Authorities | Actual Spending |
|---|---|---|
| 322.1 | 411.7 | 379.8 |
|
||
| Planned | Actual | Difference |
|---|---|---|
| 2,658 | 2,636 | 22 |
|
||
Performance Summary
In 2011-2012, Health Canada focused on ongoing improvements to its delivery of internal services while building department-wide approaches to services delivery and investment planning. Health Canada developed and implemented a Strategic Investment Planning Process for prioritization of projects. Priority investments are highlighted in assets, acquired services and projects that reflect the areas of greatest risk for Health Canada and that best support Government of Canada objectives.
The development of a Community of Practice for Grants and Contributions Management, with active participation by Health Canada and PHAC, has resulted in modernized processes and tools including work towards a single-solution for grants and contributions, for Health Canada, the Public Health Agency of Canada, and Aboriginal Affairs and Northern Development Canada through shared service arrangements.
A Web Presence Renewal Initiative was launched and a Corporate Consultation Protocol was developed to improve stakeholder engagement / consultation activities.
Human Resources (HR) continued to improve its services by enhancing processes and tools.
A major Information Technology services achievement was the multi-year Application Reduction Initiative (ARI) to reduce duplicate or non-essential applications, decrease costs and complexity risks. ARI's target was to retire 687 applications by the end of 2012-13. ARI was completed a year ahead of schedule and retired a total of 787 applications by March 31, 2012.
Information management is gradually being transformed and modernized through the development of an implementation strategy for Enterprise Content Management Solution. This solution is aimed at better managing the life-cycle of information through simplifying storage, security, version control, process routing, and retention.
The Laboratory Infrastructure Renewal Plan Phase I was implemented to support current and future science priorities while reducing capital pressures over the long term. Health Canada was recognized as a leader in laboratory management across government by the ADM sub-committee of the Federal Laboratories Integrated Governance for the Banting Building and fume hood technologies developed won a National Real Property Institute of Canada award in the category of ‘Best Practices – Environmental Sustainability.' Its implementation improved the health and safety conditions in Health Canada's laboratories, increased laboratory productivity, and garnered more than $1M in cost avoidance.
The Departmental Security Plan was developed detailing decisions for managing security risks and outlines strategies, goals, objectives, priorities and timelines for improving departmental security. Health Canada is a finalist for the 2012 Disaster Recovery Institute Canada's Award of Excellence for outstanding achievement in Business Continuity Management. In addition, Health Canada has embarked upon, and is ahead of an accelerated schedule to conduct threat/risk assessments at all custodial laboratories.
FSDS Performance Summary
Health Canada is subject to the Federal Sustainable Development Act and is thus required to prepare a departmental strategy to comply with and contribute to the Federal Sustainable Development Strategy (FSDS). Health Canada meets this requirement through the Internal Services Program Activity. Regular functions under this program activity contribute to Theme IV, Shrinking the Environmental Footprint of Government, of the FSDS. Implementation strategies for Greening Government Operations (GGO) have been developed, and in 2011-12 progress has been made in the following areas:
- Developed and put into effect a Green Buildings Strategic Framework for the four green building targets;
- Increased the percentage of environmentally friendly information technology hardware purchases to 88% from baseline of 29% in 2009-2010;
- Implemented a Plan for Managing Surplus Electronic and Electrical Equipment;
- Adopted and implemented a Green Meeting Guide; and
- Established a baseline inventory of printing units and developed a Printing Unit Policy as part of the strategy to reduce the ratio of employees to printing units.
For additional details on Health Canada's Greening Government Operations activities, please consult GGO Supplementary Information Tables (Section IV).
Changes to Government Structure
Impacts on Financial and Human Resources Resulting from the Establishment of Shared Services Canada
| Planned Spending | Total AuthoritiesFootnote * | |
|---|---|---|
| Net transfer post Orders in Council (OIC)Footnote ** to Shared Services Canada (SSC) | 22.4 | 22.4 |
|
||
| Planned | Actual | |
|---|---|---|
| Deemed to SSC | 94 | 93 |
Section III: Supplementary Information
Financial Highlights
| % Change | 2011-12 | 2010-11 | |
|---|---|---|---|
| Total net liabilities | (3%) | 1,076,875 | 1,111,241 |
| Total net financial assets | (16%) | 249,000 | 294,875 |
| Departmental net debt | 1% | 827,875 | 816,366 |
| Total non-financial assets | (16%) | 149,388 | 178,308 |
| Departmental net financial position | 6% | (678,487) | (638,058) |
| % Change | 2011-12 | 2010-11 | |
|---|---|---|---|
| Total expenses | 4% | 3,920,279 | 3,754,710 |
| Total revenues | 32% | 98,156 | 74,467 |
| Net cost from continuing operations | 4% | 3,822,123 | 3,680,243 |
| Transferred operations | (42%) | 35,273 | 60,502 |
| Net cost of operations before government funding and transfers |
3% | 3,857,396 | 3,740,745 |
| Departmental net financial position | 6% | (678,487) | (638,058) |
Liabilities by Type
Liabilities by Type - Text Equivalent
- Pie chart showing percent of liabilities by type
- Accounts payable and accrued liabilities = 34 percent
- Vacation pay and compensatory leave = 4 percent
- Deferred revenue = 0 percent
- Employee future benefits = 13 percent
- Other liabilities = 49 percent
Total liabilities were $1,076.9M at the end of 2011-12, a decrease of $34.4M from the previous year. $89.2M of the decrease in liability is the result of payments and deemed interest payments to Canada Health Infoway Inc. originating from the 2007 and 2009 Budgets. There was also a decrease to employee future benefits of $33.5M due to the liquidation of severance pay and termination benefits and cessation of accumulation of benefit obligations as a result of changes in some collective agreements, as well as the transfer of a number of employees to Shared Services Canada. Accounts payable and accrued liabilities increased by $56.6M mainly due to the accrual of workforce adjustment costs. Other liabilities increased by $33.0M as a result of changes in the provision for contingent liabilities.
Assets by Type
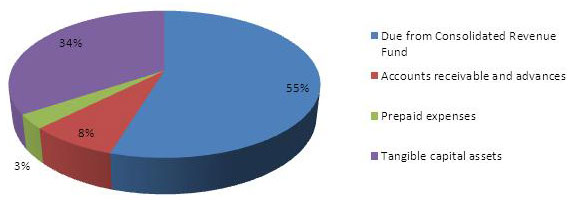
Assets by Type - Text Equivalent
- Pie chart showing percent of assets by type
- Due from Consolidated Revenue Fund = 55 percent
- Accounts receivable and advances = 8 percent
- Prepaid expenses = 3 percent
- Tangible capital assets = 34 percent
The total of financial and non-financial assets was $398.4M at the end of 2011-12 representing a decrease of $74.8M from the previous year. The majority of the change was due to a decrease in the Due from the Consolidated Revenue Fund account of $53.7M which is consistent with the decrease in liabilities. There was also a decrease in tangible capital assets of $22.1M which is primarily a result of the transfer of $20.5M of these assets to Shared Services Canada.
Expenses - Where Funds Go
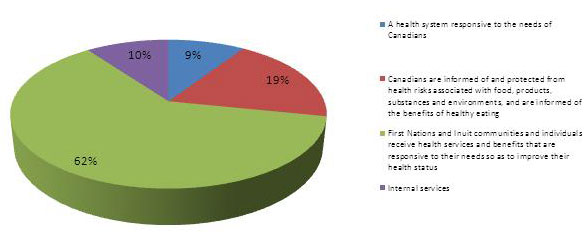
Expenses - Where Funds Go - Text Equivalent
- Pie chart showing percent of expenses by strategic outcome
- A health system responsive to the needs of Canadians = 9 percent
- Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating = 19 percent
- First Nations and Inuit communities and individuals receive health services and benefits that are responsive to their needs so as to improve their health status = 62 percent
- Internal services = 10 percent
Health Canada's total expenses were $3.9B in 2011-12, an increase of $165.6M from 2010-11. This was due mainly to an increase in salaries and employee benefits of $96.7M in large part resulting from the accrual of workforce adjustment costs of $65.1M, as announced in Canada's Economic Action Plan 2012. The other major contributing factor was an increase in the number Full Time Equivalents (FTEs) to support the implementation of the Cost Recovery Initiative for human drugs and medical devices regulatory programs, which was approved by Parliament in May of 2010. There was also an increase in travel for non-insured health patients of $24.5M which is a result of higher demand experienced during the year as compared with the prior year. Expenses in this program area are subject to unanticipated fluctuations as costs are demand driven. Also, other expenses have increased $30.4M, primarily as a result of changes in the provision for contingent liabilities.
Revenues - Where Funds Come From
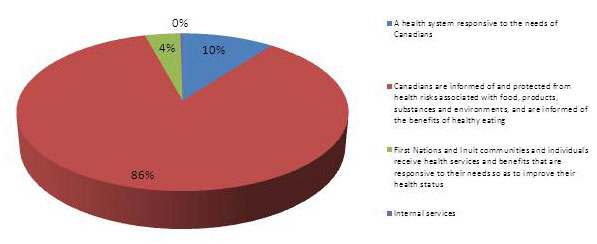
Revenues - Where Funds Come From - Text Equivalent
- Pie chart showing percent of revenues by strategic outcome
- A health system responsive to the needs of Canadians = 10 percent
- Canadians are informed of and protected from health risks associated with food, products, substances and environments, and are informed of the benefits of healthy eating = 86 percent
- First Nations and Inuit communities and individuals receive health services and benefits that are responsive to their needs so as to improve their health status = 4 percent
- Internal services = 0 percent
Health Canada receives most of its funding through annual Parliamentary appropriations. Health Canada uses the Consolidated Revenue Fund (CRF) which is administered by the Receiver General for Canada. All cash received is deposited to the CRF and all Cash disbursements are paid from the CRF. Health Canada does however generate revenue from program activities that support the above-noted Strategic Outcomes. Health Canada's total revenue was $98.2M in 2011-12, an increase of $23.7.0M over 2010-11. This increase is primarily a result of changes in fee regulations that became effective on April 1, 2011.
Financial Statements
Financial statements can be found on Health Canada's website.
Supplementary Information Tables
All electronic supplementary information tables can be found with the 2011-12 Departmental Performance Report, on the Health Canada website.
- Details on Transfer Payment Programs (TPPs)
- Up-Front Multi-Year Funding
- Greening Government Operations
- Horizontal Initiatives
- Upcoming Internal Audits and Evaluations over the next three fiscal years
- Sources of Respendable and Non-Respendable Revenue
- Summary of Capital Spending by Program Activity
- User Fees
Additional Weblinks
- Aboriginal Affairs and Northern Development Canada
- Aboriginal Diabetes Initiative
- Aboriginal Head Start On Reserve
- Aboriginal Health Transition Fund
- Act to Amend the Tobacco Act
- Air Quality
- Caffeinated Energy Drinks
- Canada Consumer Product Safety Act
- Canada Health Act
- Canada Health Infoway
- Canada Prenatal Nutrition Program
- Canadian Food Inspection Agency
- Canadian Food Inspection Agency Act
- Consumer Product Safety
- Controlled Drugs and Substances Act
- Cosmetic Regulations
- Cracking Down on Tobacco Marketing Aimed at Youth Act
- Curbing Childhood Obesity: A Federal, Provincial and Territorial Framework for Action to Promote Healthy Weights
- Department of Health Act
- Departmental Security Plan
- Drinking Water Advisory Module
- Drug Safety and Effectiveness Network
- Federal Sustainable Development Act
- Federal Sustainable Development Strategy
- Federal Tobacco Control Strategy
- Food and Consumer Safety Action Plan
- Food and Drugs Act
- Food and Drugs Act and Regulations
- Food Safety and Nutrition
- Marihuana Medical Access Program
- Maternal Child Health
- Medical Devices Program
- Medical Devices Quality Management System Regulations
- National Aboriginal Youth Suicide Prevention Strategy
- National Strategy to Address Mould in First Nations Communities
- Natural Health Products
- Non-Insured Health Benefits
- Nutrition and Healthy Eating
- Nutrition Facts Education Campaign
- Nutrition North Canada
- Official Languages Act
- Official Languages Health Contribution Program
- Organization for Economic Co-Operation and Development
- Radiation Dosimetry
- Regulatory Cooperation Council
- Shared Services Canada
- Social Media
- Strategy Against Tuberculosis for First Nations On-Reserve
- Sustainable Development Strategy Performance Report
- Tobacco Act
- Water Quality
- World Health Organization
- World Health Organization - Framework Convention on Tobacco Control
Section IV: Other Items of Interest
Organizational Contact Information
Marc Desjardins
Director General
Planning and Corporate Management Practices Directorate
Jeanne Mance Building - Floor: 12 - Room: B1243
200 Eglantine Driveway, Tunney's Pasture
Ottawa, Ontario K1A 0K9
Telephone: 613-948-6357
Closure of Assisted Reproduction Canada
In response to the 2010 ruling of the Supreme Court of Canada that significantly reduced the federal role in assisted human reproduction (AHR), the government of Canada announced that it would wind down Assisted Human Reproduction Canada. Health Canada has taken over responsibility for the remaining federal functions in AHR, such as compliance and enforcement, and outreach, effective October 1, 2012.
Risk Management Performance Summary
Health Canada actively managed and responded to risks – both positive and negative – in 2011-12. A selection of activities are presented below which serve to demonstrate the range of risks Health Canada manages and the concrete interventions made to reduce impacts or probabilities of adverse risk, or to enhance the impacts or probabilities of positive risks.
| Strategic Outcome | Risks Associated with Activities | Responses to Risks | Type* |
|---|---|---|---|
| Strategic Outcome 1 - A Health System Responsive to the Needs of Canadians | Managing uncertainty in meeting health needs in Canada created by shortage of human resources, including in remote & rural communities. | Implemented Pan-Canadian Health Human Resource Strategy in concert with provincial, territorial and other partners; provided contribution agreements to support the Internationally Educated Health Professionals Initiative. | O |
| Managing uncertainty and hazards associated with emergency situations. | Initiated a national exercise - gap analysis and appropriate responses; risk assessment of emergency response initiated. | O | |
| Hazards associated with radioactive threats from Fukushima, Japan. | Produced an After-Action Report on effectiveness of Canadian response; lessons learned added to the Health Portfolio Emergency Response Plan. | H/N | |
| Strategic Outcome 2 - Safety communicated on food, products, substances and environments, and healthy eating, in Canada | Managing uncertainty and opportunities associated with health products. | Undertook regulatory modernization to capture positive risks via accelerating/streamlining drug submissions; initiated the use of foreign regulatory information within review processes for health products. | N |
| Opportunities associated with human health drugs and medical devices. | Undertook regulatory modernization to update user fee regulations; use of performance information and monitoring. | O | |
| Opportunities associated with food safety enhancement. | Initiated food safety legislative framework renewal; supported implementation through development of tools, guidelines and stakeholder engagement. | O | |
| Managing uncertainty and hazards associated with food safety. | Simplified and modernized federal legislation and regulations that affect food safety; transitioned energy drinks to food regulatory framework. | N | |
| Hazards associated with indoor/outdoor air pollutants. | Developed new national air quality management framework for managing air quality in collaboration with Environment Canada; developed new Canadian ambient air quality standards; expanded the Air Quality Health Index (AQHI). | H/N | |
| Hazards associated with water safety. | Developed the Drinking Water Advisory Module in collaboration with the Public Health Agency of Canada (PHAC). | H | |
| Hazards associated with consumer product safety. | Launched the consumer product incident reporting system to support the new Canada Consumer Product Safety Act (CCPSA); applied an integrated industry outreach implementation plan. | H | |
| Hazards associated with chemicals. | Launched the second phase of the Chemicals Management Plan whereby further progress was made in assessing, and where appropriate initiating the risk management, of the 3000 remaining priority chemicals to be addressed by 2020. | H | |
| Hazards associated with tobacco and controlled and illicit substances use and abuse. | Renewed the Federal Tobacco Control Strategy as well as implemented a new compliance and enforcement plan for the Act to Amend the Tobacco Act; engage in public education/outreach initiatives; undertook controlled substances inspections. | H | |
| Managing uncertainty associated with the use of pesticides. | Health Canada continued to work with federal, provincial, and international partners to use the latest research and monitoring results to validate assumptions and reduce scientific uncertainty in its regulatory decisions. | N | |
| Strategic Outcome 3 - First Nations and Inuit communities and individuals receive health services and benefits that are responsive to their needs so as to improve their health status | Managing uncertainty associated with First Nations and Inuit (FNI) Primary Health Care. | Maintained contributions to programs, services, communities and initiatives; developed Strategy Against Tuberculosis for First Nations On-Reserve; supported capacity development for emergency response in First Nations communities. | N |
| Hazards associated with water safety in FNI communities. | Applied the Guidelines for Canadian Drinking Water Quality in FNI communities; collaborated with Aboriginal Affairs and Northern Development Canada (AANDC). | H | |
| Opportunities associated with support for FNI health care maintenance. | Streamlined pre-determination/pre-approval for oral health care; continued development of standardized price file for medical supplies and equipment. | O | |
| Opportunities associated with coordinating and integrating FN health programs and services. | Signed Tripartite health agreement with British Columbia First Nations and the Province of British Columbia; initiated implementation of the Health Services Integration Fund. | O | |
| Opportunities associated with support provided to FNI for health services and benefits. | Harmonized management of grants and contributions with AANDC and other partners. | O | |
| Internal Services | Managing uncertainty associated with project management. | Developed and implemented a Strategic Investment Planning Process for department-wide prioritization of projects. | N |
| Managing uncertainty associated with performance measurement. | Developed an Evaluation Framework Process. | N | |
| Opportunities associated with Grants and Contributions management. | Developed and implemented an automated grants and contributions information management system in collaboration with PHAC, and AANDC using complementary service arrangements; developed and mandated use of an Enterprise Risk Management tool. | O | |
| Managing uncertainty associated with the Budget Economic Action Plan 2012. | Human Resources shifted priorities and resources to develop and implement workforce adjustments. | N | |
| Managing uncertainty associated with information technology (IT) products and services. | Participated in Shared Services Canada innovations; reduced duplicate or non-essential applications. | N | |
| Managing uncertainty associated with information management (IM). | Enterprise Content Management Solution Implementation Strategy is being developed to enhance management of the life-cycle of information. | N | |
| Hazards/threats associated with safety and security, and business continuity. | Developed the Departmental Security Plan in line with current internal security risks and; strengthened the Business Continuity Management Program. | H | |
|
|||
Page details
- Date modified: