
2019 First Annual Report of the Disability Advisory Committee: Enabling access to disability tax measures
This report is dedicated to Wendall Nicholas, for his commitment and leadership as a member of the Disability Advisory Committee.
Table of contents
- Introduction
- Section 1 – Understanding disability tax measures
- Section 2 – Enabling DTC access through improved eligibility criteria
- Section 3 – Enabling DTC access through improved application procedures
- Health provider roles
- Health providers as gatekeepers
- When tax preparers/promoters and health providers disagree on eligibility
- When health providers may not have the information base necessary to completing Form T2201 on behalf of applicants
- When an applicant has more than one severe and prolonged impairment in an activity of daily living
- Expanding the list of health providers qualified to complete Form T2201
- Costs of completing Form T2201
- Clarity of Form T2201
- Layout of Form T2201
- Clarification letters
- Request a review / Appeal a decision
- Quality assurance framework
- Health provider roles
- Section 4 – Enabling access to DTC through improved communications
- Section 5 – Enhancing access to other disability benefits
- Section 6 – Recognizing the additional costs of disability
- Appendix 1 – List of Committee Members
- Appendix 2 – Recommendations
- Appendix 3 – Disability Advisory Committee Terms of Reference
- Appendix 4 – List of Organizations We Heard From
- Appendix 5 – Health Providers Survey
- Appendix 6 – Financial Advisors and Tax Preparers Survey
- Appendix 7 – Description of Federal Measures for Persons With Disabilities
- Appendix 8 – Disability Measures Linked to DTC Eligibility
- Appendix 9 – Form T2201
- Appendix 10 – DTC Data for Mental Functions
- Appendix 11 – RDSP Concerns
- Appendix 12 – Questions for DTC Refundability Conference Call
Introduction
Disability Advisory Committee
The Disability Advisory Committee was originally formed in March 2005 after the Technical Advisory Committee (TAC) on Tax Measures for Persons with Disabilities had completed its mandated work and released its report Disability Tax Fairness in 2004. The Committee subsequently was disbanded in 2006. Because of increased attention to the disability tax credit (DTC) and its administration, the Honourable Diane Lebouthillier, Minister of National Revenue, announced the reinstatement of the Committee in November 2017.
The Minister of National Revenue and the Canada Revenue Agency (CRA) are committed to ensuring that all Canadians receive the tax credits and benefits to which they are entitled. The Committee is a forum that enables CRA officials to come together with stakeholders to better incorporate the views of Canadians with disabilities into the Agency’s decision making and procedures.
Committee members are providing their insights on ways to improve access to various tax measures for Canadians with disabilities. Enhancing the accessibility of CRA services to persons with disabilities is an ongoing effort, which has been assisted by the Committee’s work.
Committee membership
The Committee is composed of nine voluntary members including persons with disabilities, health providers and professionals from a variety of fields, such as tax professionals and lawyers. See Appendix 1 for the list of Committee members who contributed to the report. The Committee is co-chaired by Dr. Karen R. Cohen, Chief Executive Officer, Canadian Psychological Association, and by Frank Vermaeten, Assistant Commissioner, Assessment, Benefit, and Service Branch, CRA. A 10th member of the Committee, Ms. Sherri Torjman, former co-chair of the TAC, serves as vice-chair. Ms. Torjman has been retained on contract by the CRA to support the Committee in co-ordinating its activities and fulfilling its reporting obligations.
Mr. Vermaeten, as co-chair of the Committee, functioned as the liaison between the Committee and the CRA. Under Mr. Vermaeten’s leadership, the CRA assisted the Committee in its work, providing secretariat services as well as research and communications support.Footnote 1
The Committee’s work is independent and impartial. During the first year of its mandate, the Committee identified research interests and led initiatives to study these areas in greater detail. The report that follows outlines the findings and recommendations, as developed and articulated by the Committee. See Appendix 2 for a full list of the recommendations.
Committee mandate
The mandate of the Committee is to provide advice to the minister of national revenue and the commissioner of the Agency on:
- the administration and interpretation of the laws and programs related to disability tax measures;
- ways in which the needs and expectations of the disability community can be better taken into consideration;
- increasing the awareness and take-up of measures for persons with disabilities;
- how to better inform persons with disabilities and various stakeholders about tax measures and important administrative changes; and
- current administrative practices and how to enhance the quality of services for persons with disabilities (see Appendix 3).
Committee work
Our committee met four times since its reinstatement. In addition, Committee members participated in one of four working groups set up to explore certain issues in depth. Working groups focused on stakeholder engagement, health provider concerns, tax preparer and financial advisor considerations, and policy/legislative questions. Unfortunately, the working group on Indigenous issues was curtailed by the untimely passing of Committee member Wendall Nicholas. We plan to address these issues in our future work.
The deliberations and recommendations of our committee were shaped by what we heard from individual Canadians, organizations representing persons with disabilities, health providers, tax preparers and policy experts. Early in our mandate, the Committee issued an open invitation to Canadians and organizations representing persons with disabilities to share with us the challenges they faced regarding the DTC and disability tax measures, more generally. We received responses from 53 private individuals and 34 organizations (see Appendix 4).
The Committee also conducted a survey of health providers with respect to DTC eligibility criteria and administrative procedures (see Appendix 5). An online questionnaire was sent to seven national organizations representing the health providers who can certify a DTC application (Form T2201, Disability Tax Credit Certificate) discussed below. We received 1,164 responses to the questionnaire, including several hundred additional comments.
A comparable survey was designed to seek the views of tax preparers and financial advisors (see Appendix 6). We look forward to incorporating their responses in future work. Similarly, a client experience survey will be developed in the coming months to gather information from current and former DTC recipients.
Finally, we reviewed relevant parliamentary reports as well as Disability Tax Fairness, produced in 2004 by the TAC on Tax Measures for Persons with Disabilities. Our committee also heard from a few academics who sent us studies on the DTC. We organized a conference call involving selected experts on the question of DTC refundability. Concurrently to the Committee’s work, several Committee members made a presentation to the Standing Senate Committee on Social Affairs, Science and Technology about the DTC and registered disability savings plans, and the co-chair was asked to present to a local group of health providers about the DTC and the Committee’s work.
Committee proposals
Our committee wants to acknowledge that Canadians are fortunate to have a DTC. This vital measure recognizes the potential impact of severe and prolonged disability upon individuals’ disposable income as well as their capacity to earn that income. At the same time, we heard about the many challenges embedded in the design and delivery of this tax measure, described below.
The DTC eligibility criteria, discussed in Section 2, comprise the first set of challenges. We document the wide-ranging concerns we heard from DTC applicants, current beneficiaries and hundreds of health providers. Our committee proposes both modest clarifications and significant changes to the existing eligibility criteria.
We turn our attention in Section 3 to DTC administrative practices. Regardless of whether the DTC eligibility criteria remain the same or change in response to our recommendations, DTC applications must be processed more fairly and effectively. Our committee makes several proposals for improved administrative practices. We also suggest the development of a quality assurance framework for ongoing monitoring and improvement of DTC eligibility procedures.
We focus in Section 4 on better communications around the DTC and disability tax measures, more generally. Most Canadians, and especially those with disabilities, are unaware of the range of benefits to which they may be entitled. We are particularly concerned about reaching Indigenous Canadians. We are also concerned that some individuals who have an impairment may need assistance to apply for the DTC and to access other tax provisions.
Our committee discussed at length the fact that the DTC has evolved beyond its original purpose. It is now more than just a measure that recognizes additional costs associated with severe and prolonged disability. It also acts as a screen for other crucial disability benefits. This expanded role has given rise to unique challenges that we consider in Section 5.
The final section of our report discusses various issues around disability-related costs. These involve not only the DTC but also the medical expenses tax credit for medical expenses and the disability supports deduction. It is essential to resolve these cost concerns, given the high rate of poverty among persons with severe disabilities.
Taken together, our recommendations seek to ensure that:
- DTC eligibility criteria are clearer, clinically relevant and empirically based;
- DTC administrative procedures are more transparent and fair;
- CRA materials and communications are more accessible and widely available;
- barriers embedded in the DTC gateway function are reduced or removed; and
- more attention is paid to the need for assistance for disability-related costs, bearing in mind the disproportionately high rate of poverty among persons with severe disabilities.
Our primary purpose in this first year of our work was to improve access to the DTC. However, where appropriate, we raised broader issues that we thought the CRA and/or the federal government, more generally, should address.
Finally, but perhaps most important, our work was guided by the principle of fairness. We hope that this principle also helps guide future CRA work.
Section 1 – Understanding disability tax measures
The Committee serves as an important forum to provide the CRA with feedback on the administration of tax measures for Canadians with disabilities (see Appendix 7). These include the:
- disability tax credit (DTC);
- medical expense tax credit;
- refundable medical expense supplement;
- disability supports deduction; and
- Canada caregiver credit.
There is also a set of disability tax measures and programs that require DTC eligibility (see Appendix 8). They include the child disability benefit and the registered disability savings plan (RDSP).
Disability tax credit (DTC)
While the mandate of the Committee includes this range of tax measures, our discussions focused primarily upon the DTC for the first year of our work. This tax measure plays two key roles.
First, the DTC helps recognize the additional costs that persons with severe disabilities may face. Second, it acts as a screen for a range of other disability-related programs and services. We discuss this gateway function later in the report.
The DTC provides tax relief to individuals with severe and prolonged impairments in function that restrict them in the basic activities of daily living or who are blind. It is also available to those who require therapy in order to sustain a vital function.
The credit is based on the assumption that these individuals likely incur a range of disability-related costs that they are not able to claim under the medical expense tax credit. The DTC also assumes that persons with severe and prolonged disabilities likely have their income-earning capacity negatively affected because of the extra time they must devote to their severely disabling condition. The purpose of this tax measure is to help persons with disabilities retain more from their work efforts.
DTC applicants must have a severe and prolonged impairment in physical and/or mental functions that impedes their ability to carry out the activities of daily living. An impairment is considered prolonged if it is expected to last or has lasted at least 12 months.
In order to qualify for the DTC, individuals must submit application Form T2201, Disability Tax Credit Certificate. A designated health provider must certify the type, extent and expected duration of impairment (see Appendix 9).
The DTC plays a significant role among disability measures. At last count in the 2016 to 2017 fiscal year, some 770,000 individuals claimed the DTC. The DTC expenditure increased steadily in real terms from 2011 to 2017.
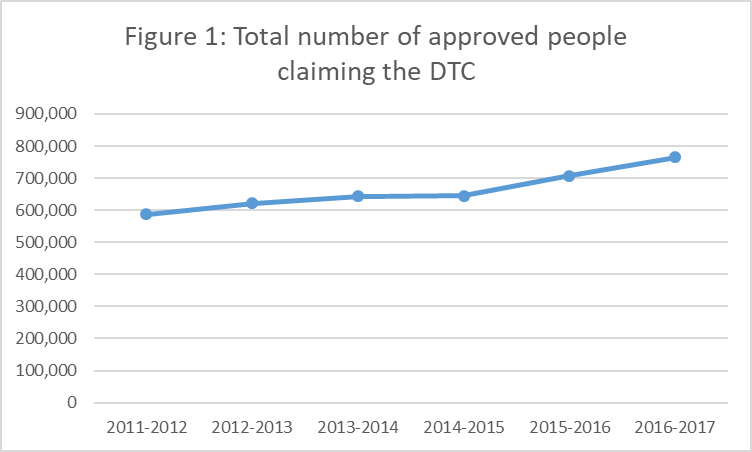
Text version
| Year | Total Number of approved people claiming Disability Tax Credit |
|---|---|
| 2011-2012 | 586,909 |
| 2012-2013 | 622,044 |
| 2013-2014 | 643,940 |
| 2014-2015 | 644,479 |
| 2015-2016 | 706,968 |
| 2016-2017 | 765,072 |
But while the caseload appears high and costs have been rising, significant numbers of applicants have also been refused the DTC. Figure 2 shows the number of applications, approvals and rejections from 2011 to 2017.
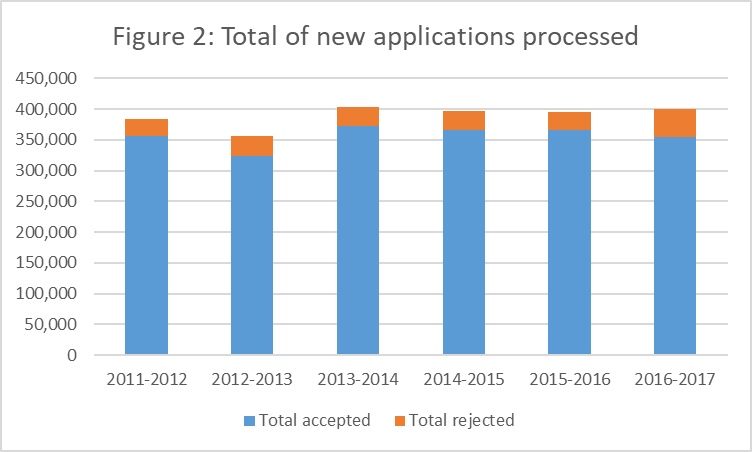
Text version
| Year | Total accepted | Total rejected |
|---|---|---|
| 2011-2012 | 355,900 | 27,329 |
| 2012-2013 | 324,368 | 32,023 |
| 2013-2014 | 373,143 | 30,400 |
| 2014-2015 | 365,991 | 30,462 |
| 2015-2016 | 365,274 | 30,235 |
| 2016-2017 | 354,798 | 45,157 |
The data are especially valuable in helping to identify where specific problems may lie. The relatively high rate of rejection of applications in mental functions category is particularly noteworthy. The data are consistent with the concerns raised in submissions to our committee and in the responses to the health provider survey.
It has long been recognized that the DTC eligibility criteria are complex and difficult for both persons with disabilities and health providers to understand. It is these eligibility criteria to which we now turn.
DTC eligibility criteria
There are different ways for which a person can be eligible for the DTC. The person must meet one of the following criteria:
- is blind;
- is markedly restricted in at least one of the basic activities of daily living;
- is significantly restricted in two or more of the basic activities of daily living (can include a vision impairment); or
- needs life-sustaining therapy.
In addition, the person's impairment must meet both of the following:
- is prolonged, which means the impairment has lasted, or is expected to last for a continuous period of at least 12 months; and
- is present all or substantially all the time (at least 90% of the time).
Section 2 – Enabling DTC access through improved eligibility criteria
Introduction
For years, persons with disabilities, members of Parliament, health providers and academics have expressed concern about the policy and administrative aspects of the disability tax credit (DTC). Its eligibility criteria are long and complex, making it difficult for most Canadians to understand this tax-delivered assistance and to determine whether they potentially could qualify for this measure. The complexities also present multiple challenges to health providers who are required to complete Form T2201.
Many of the concerns that were brought to the attention of the Committee and that we address in this report are not new. They have been raised over the years in numerous reports, including those produced by the House of Commons Sub-Committee on the Status of Persons with Disabilities, the Technical Advisory Committee on Tax Measures for Persons with Disabilities and, most recently, the Standing Senate Committee on Social Affairs, Science and Technology.
In addition to these reports, wide-ranging concerns were brought directly to our attention in the submissions we received from individual Canadians, organizations representing persons with disabilities and health providers who responded to the health provider survey that our committee conducted in June and July 2018.
The many eligibility complexities identified both recently and in years past can be grouped into five key themes:
- the definition of mental functions;
- the interpretation of marked restriction and the 90% guideline;
- parity in the treatment of physical and mental functions;
- life-sustaining therapy; and
- designated conditions.
Each of these issues is discussed below. Proposed improvements to various administrative procedures and CRA decision-making processes around DTC eligibility are considered in Section 3. We also note that a new challenge has arisen in recent years regarding the additional and vital role the DTC now plays as a gateway to other benefits. We discuss this emerging issue in Section 5.
Before we explore in greater depth each of the identified concerns, the Committee would like to acknowledge that we very much appreciate the challenges involved in the fair and consistent assessment of DTC eligibility. We know that this determination is no easy task.
We understand that in assessing eligibility for the DTC, the key criterion is not so much the presence of certain disabilities but rather the impact of these disabilities on the applicant’s day-to-day functioning. The person must be blind or be markedly restricted in at least one of the basic activities of daily living.
These basic activities of daily living are on the DTC application, Form T2201. They include vision, speaking, hearing, walking, eliminating, feeding, dressing and mental functions necessary for everyday life. The need for life-sustaining therapy as defined on Form T2201 also renders a person eligible for the DTC.
Because Form T2201 and the self-assessment questionnaire in Guide RC4064, Disability-Related Information, are the key sources of information to the public about the DTC, it is of utmost importance that these documents respect both the legislative intent of the Income Tax Act and its interpretation by the Tax Court of Canada.
We begin our discussion by focusing on the legislative intent of the DTC and the need for clarity in conveying this legislative intent. As noted, the effective administration of this intent and its clear communication by the CRA are considered in subsequent sections of this report.
Definition of mental functions
Perhaps no functional area in the DTC eligibility list has been fraught with more difficulty than mental functions. We are concerned both with how mental functions are defined in the federal Income Tax Act and how they are assessed on Form T2201.
As noted, the policy and administrative challenges with respect to the DTC treatment of mental functions are not new. They have been documented for close to 20 years.
The Sub-Committee on the Status of Persons with Disabilities held parliamentary meetings with representatives of health-related voluntary organizations as well as the Canada Revenue Agency and the Department of Finance Canada from November 2001 to February 2002. On March 21, 2002, the Sub-Committee tabled its report, Getting it Right for Canadians: The Disability Tax Credit, in the House of Commons.
When consultations with stakeholders failed to resolve major concerns with the administration of the DTC, the federal government created the Technical Advisory Committee (TAC) on Tax Measures for Persons with Disabilities in April 2003. While the TAC acknowledged the wide range of policy and administrative concerns linked to the DTC, it identified impairment in mental functions as the most difficult eligibility assessment challenge.
In the report, Disability Tax Fairness, published in December 2004, close to 15 years ago, the TAC made several recommendations to clarify the way in which mental functions were defined for the DTC proposing the following:
- changing "thinking, perceiving and remembering" in the Income Tax Act to mental functions necessary for everyday life in subparagraph 118.4(1)(c)(i) (recommendation 2.2); and
- providing for the cumulative effects of restrictions in more than one basic activity of daily living where the effects are equivalent to a marked restriction in a single basic activity of daily living in subparagraph 118.3(1)(a.1) and (a.3) (recommendation 2.4).
The TAC also recommended that the list of mental functions be expanded as it was deemed to be too narrowly defined:
"In our view mental functions are the range of processes that govern how people think, feel and behave. Based on our consultations and research, they include memory, problem solving, judgment, perception, learning, attention, concentration, verbal and non-verbal comprehension and expression, and the regulation of behaviour and emotions. These functions are necessary for activities of everyday life that are required for self-care, health and safety, social skills and simple transactions [TAC 2004: 122]."
The Income Tax Act subsequently was amended in 2005. Mental functions necessary for everyday life as set out in Form T2201 were changed to the following:
- adaptive functioning (for example, abilities related to self-care, health and safety, abilities to initiate and respond to social interactions, and common, simple transactions);
- memory (for example, the ability to remember simple instructions, basic personal information such as name and address, or material of importance and interest); and
- problem-solving, goal-setting, and judgment, taken together (for example, the ability to solve problems, set and keep goals, and make the appropriate decisions and judgments).
It is not clear how the federal government arrived at this interpretation of the TAC recommendations on the definition of mental functions. The changes that were introduced did not effectively capture the full intent of its proposals.
Data on the rate of DTC acceptance by function show that challenges in establishing eligibility for persons with disabilities related to mental functions continue to this day. The recent report of the Standing Senate Committee noted that:
"The approval rate for all new DTC applications processed ranged between 93% and 91% over the five-year period between 2011-2012 and 2015-2016. In 2016-2017, the approval rate for new applications declined to 89%.
Yet when the data were disaggregated by activity limitations, applications related to mental functions had consistently the lowest approval rates. Over the six-year period, applications related to mental functions had an approval rate ranging from 88% in 2011-2012 to a low of 81% in 2016-2017.
Applications related to the activities of dressing (often associated with pain and musculoskeletal disabilities) and feeding (a person requiring a feeding tube) consistently had the highest approval rates, ranging between 97% and 94% over the period. It is also noted that 2016 to 2017 appears to be an outlier year, with approval rates lower across all activity limitations, but most significantly for activities related to mental functioning [Senate 2018: 10]."
The data also reveal that while activities related to mental functioning have consistently lower approval rates, they represent the largest category of DTC claimants in five of the last six years (see Appendix 10).
In fact, the changes made to the Income Tax Act in 2005 ended up creating new problems that did not make the eligibility process any easier. For the purposes of establishing DTC eligibility, the assessment of persons with impairment in mental functions continues to be complex.
For one thing, the eligibility criteria for mental functions are conceptually confusing and are not clinically meaningful. We learned from the health provider survey that "while the effects of disability have to be unpacked in a way that the CRA understands, they are a bit foreign to a clinician geared more toward treatment." Another respondent told us: "I do not conduct diagnostic assessments with the purpose of filling out the CRA DTC form. This makes it difficult to comment on certain areas that CRA wants input on."
In fact, we note that the mental functions identified on Form T2201 are not all functions but represent, instead, a mix of functions and activities of daily living. Memory, problem solving, goal setting and judgment are all mental functions. Abilities related to self-care, and health and safety, by contrast, are activities.
We also question why three distinct mental functions must be present conjunctively. The Income Tax Act requires that problem solving, goal setting and judgment be "taken together," which means that a person must have a severe and prolonged impairment in all three mental functions to qualify for the DTC.
It makes no clinical sense to require that these three functions be present in combination in order to meet the eligibility criteria for the DTC. A person may have a severe and prolonged depression, for example, which compromises goal setting and judgment but not problem solving.
To add confusion, Form T2201 appears to contradict the conjunctive requirement. It acknowledges, through the following note included on the form, that problem solving, goal setting and judgment may be interpreted disjunctively: "A restriction in problem solving, goal setting or judgment that markedly restricts adaptive functioning, all or substantially all of the time, would qualify." At the very least, this contradiction must be resolved.
Our third concern: Requiring that problem solving, goal setting and judgment are present together applies a degree of rigour for mental functions that is not expected for the activities of daily living related to physical functions. It reflects a lack of parity between the treatment of impairment in physical and in mental conditions.
A person is deemed markedly restricted in walking, for example, if he or she cannot walk, regardless of cause. Factors related to memory, goal setting, judgment, problem solving, and learning can singly or in combination be responsible for a marked restriction in mental functions necessary for everyday life. Similarly, neurological factors, orthopedic factors and fatigue can singly or in combination be responsible for a marked restriction in walking.
However, if a health provider confirms that a person cannot walk, that individual is deemed eligible regardless of which, or how many factors, underlie the inability to walk. The same principle must, in all fairness, be applied to mental functions. If a person is markedly restricted in any of the mental functions necessary for everyday life, it should not matter which factor or combination of factors underlies the marked restriction.
The Canadian Mental Health Association (CMHA) noted this problem in its submission to the Committee. "The way that ‘impairment’ is conceptualized for applications based on ‘mental functions necessary for everyday life’ creates, in comparison to the other categories on the T2201, a higher threshold for the individuals with mental health-related difficulties to qualify." Moreover, the CMHA points out that "people with mental health-related disabilities are especially vulnerable in this situation due to this array of factors in combination with ill-defined and inappropriate eligibility criteria in relation to mental illness."
In order to ensure equity in the treatment of applicants with impairment in physical functions and those with impairment in mental functions, we recommend:
That in the determination of DTC eligibility, the Canada Revenue Agency ensure that the principle of parity guides its actions with respect to physical and mental functions including, but not limited to, the removal of multiple screens of eligibility for persons with impairment in mental functions.
The current iteration of mental functions must not only be consistent with the treatment of impairment in physical functions. The list also needs to be clinically meaningful. If Form T2201 requires that a physician, nurse practitioner or psychologist attest to the nature and impact of an applicant’s impairment, then the criteria must be those routinely assessed as impaired for mental health conditions.
We heard from many providers who stated unequivocally that Form T2201 is totally inadequate when it comes to impairment in mental functions.
"The form has a medical orientation that seems to be more directed towards physical than psychological or neuropsychological disabilities."
"The category of mental health concerns is completely missing from this application. Individuals with neurodevelopmental disorders can have significant mental health problems which impact on functioning and there is no way to elaborate on this (in fact, it isn't even an option as everything is physical medicine-based in this application). For example, individuals with autism spectrum disorder may be extremely impaired in daily functioning, not due to a hearing impairment, but to the attentional processes that are required to 'tune in' to the environment. Or this same individual may be so overwhelmed from a sensory point of view that he is unable to ‘hear’ what he is supposed to be hearing (due to the inability to filter out extraneous noises)."
We recognize the challenges involved in defining mental functions. In a frequently cited Tax Court of Canada case Radage v. The Queen, former chief justice Donald G.H. Bowman set out a long and thoughtful discussion on the definition of mental functions as they were defined at the time. He pointed out the daunting complexity of mental functions and the multiple difficulties involved in trying to arrive at precise definitions of these terms [Radage v. The Queen 16].
We also note that several cases brought to the Tax Court of Canada have challenged the current definition of mental functions and its interpretation by the CRA. Most notable is the decision in Buchanan v. The Queen that was upheld by the Federal Court of Appeal, in Canada (Attorney General) v. James W. Buchanan.
Connections is an Alberta-based organization that supports individuals with cognitive disabilities. In its submission to the Committee, Connections pointed out that "many professionals believe that the DTC only applies to physical disabilities." It further noted that health providers often inform individuals with developmental disabilities that they do not qualify and the doctors or psychiatrists refuse to fill out the form.
The Canadian Mental Health Association pointed out in its submission that individuals with impairment in mental functions find that health providers lack clarity and understanding of the DTC eligibility criteria and are thus hesitant to complete the DTC form. Moreover, "the understanding of disability implicit in the T2201 overlooks many of the ADLs (activities of daily living) and functions that are impacted by mental health-related disabilities, such as lack of initiative or motivation or changed/unusual behaviour."
Our committee carried out, as noted, a survey of health providers to hear their views on the DTC and the challenges involved in assessing impairment in physical and/or mental functions. Respondents made clear that the eligibility criteria for mental functions, in particular, are not those routinely assessed nor are they helpful in determining which conditions would actually qualify for the DTC.
The understanding that some conditions may be categorically ineligible appears to abound among applicants, consumer groups and health providers even though, as mentioned, no condition other than blindness is categorically eligible and no condition is ineligible. The challenge for health providers is in understanding how markedly restricted the individual with an impairment in mental functions must be in order to be deemed eligible for the DTC.
Moreover, the survey noted uncertainties around a range of conditions including autism, attention deficit and hyperactivity disorder, post-traumatic stress disorder and schizophrenia. We heard, for example:
"It has been my experience that some clients who are much less impaired have received the credit and those who are more impaired have not. I do not know what I should be writing to ensure that my clients, many of whom have lifelong disabilities such as autism spectrum disorders, qualify."
"Because I am responsible for autism spectrum assessments, I am asked to complete them for my clients. I believe the CRA has not developed a clear understanding of how impairing the presentation is, even for high functioning individuals."
It is vital to pay attention to this feedback from health providers for whom the definition and identification of mental functions are core components of their professional expertise. These are the professionals who both develop and employ the taxonomies and diagnostic classifications of mental disorders.
We strongly urge the federal government to revise the DTC criteria related to mental functions. While there is no single commonly accepted list, there are important internationally recognized standards that can help shape a new definition of mental functions.
Our recommended reformulation of mental functions necessary for everyday life approximates two such taxonomies. We have integrated and simplified these internationally developed clinical lists into a more simple and practicable form necessary for DTC purposes.
We have reformulated the definition of mental functions based on two types of data sources:
- the international classifications from the World Health Organization (WHO) and the U.S.-based National Institute of Mental Health; and
- the feedback from more than 1,000 health providers who responded to our survey of their experience with Form T2201.
The WHO classification includes the following list of mental functions: attention, memory, psychomotor, emotional, perceptual, thought, higher level cognition, mental functions of language, calculation, mental function of sequencing complex movements, experience of self and time functions, and specific mental functions. Each of these, in turn, is broken down into specific components.
The U.S.-based National Institute of Mental Health also sets out a detailed list of cognitive functions, which include attention, perception, declarative memory, language, cognitive control and working memory. Each is described and disaggregated into its constituent components, where appropriate.
We have reformulated the definition of mental functions with these international classifications as the empirical base. We have also taken into account the recommendations of, and feedback from, clients and health providers. Our goal is to ensure that a revised list of mental functions is clearer, more consistent with clinical practice and more easily applied. We recommend:
That the Canada Revenue Agency amend the list of mental functions on Form T2201 as follows:
- attention;
- concentration;
- memory;
- judgment;
- perception of reality;
- problem solving;
- goal setting;
- regulation of behaviour and emotions (for example, mood disturbance or behavioural disorder);
- verbal and non-verbal comprehension; and
- learning.
In addition to reformulating the definition of mental functions, other administrative clarifications are required. In respect of the principles of simplicity and user friendly proposed by the Multiple Sceloris Society of Canada, we note three areas that need immediate attention.
First, the text box on page 5 of Form T2201 asks qualifying providers to describe the effects of the applicant’s impairment. We learned from submissions to the Committee, as well as the health provider survey, that the current wording on the form creates confusion. More specifically, it is unclear whether health providers are being asked to assess the actual impairment or its effects on the applicant’s functional capacity. In order to ensure clarity of interpretation, we recommend:
That the Canada Revenue Agency replace on page 5 of Form T2201 the term "effects of the impairment" with the following:
"The effects of the individual’s impairment must restrict their activity (that is, walking, seeing, dressing, feeding, mental functions, eliminating, hearing, speaking or some combination thereof) all or substantially all of the time, even with therapy and the use of appropriate devices and medication."
Second, Form T2201 itself is confusing to health providers in that it appears to provide contradictory information. In order to rectify this problem, we recommend:
That the Canada Revenue Agency delete the reference to "social activities" on page 5 of Form T2201 due to the contradiction on page 3 of the form. Page 5 states that one is ineligible on the basis of social and recreational activity, while page 3 states that the inability to initiate and respond to social interactions makes one eligible, as does the inability to engage in common simple transactions.
Third, there is confusion about the question on page 5 of Form T2201 that asks health providers about the likelihood of improvement. It is not clear if the CRA is asking whether the underlying condition is likely to improve or whether the individual’s functional capacity is expected to improve. In order to clarify the intent of the question, we recommend:
That the Canada Revenue Agency change the question on page 5 of Form T2201 about the likelihood of improvement to ask health providers whether the individual’s illness or condition that is responsible for the impairment in function, such as walking or cognitive functions, is likely to improve, as in the following example:
"In thinking about the individual’s impairment, please consider whether the condition that causes the impairment (for example, blindness, paraplegia, schizophrenia or bipolar disorder) can be expected to last for a continuous period of at least 12 months."
The introduction of a clearer and clinically valid definition of mental functions is a vital start. But it is only a start. The other equally difficult roadblock comes in the form of the criteria employed by the CRA to assess the impact of the impairment on physical and/or mental functions.
Marked restriction and the 90% guideline
In order to qualify for the DTC, the presence of impairment is not sufficient. The effect of the impairment in physical and/or mental functions must be severe and prolonged.
As noted in the first section, DTC eligibility requires that an applicant meet one of the following criteria:
- is blind;
- is markedly restricted in at least one of the basic activities of daily living;
- is significantly restricted in two or more or the basic activities of daily living (can include a vision impairment); and
- needs life-sustaining therapy.
In addition, the person’s impairment must meet all of the following criteria:
- is prolonged, which means the impairment has lasted, or is expected to last for a continuous period of at least 12 months; and
- is present all or substantially all the time (at least 90% of the time).
Applicants are considered markedly restricted if they are unable or take an inordinate amount of time to do one or more of the basic activities of daily living, even with therapy (other than life-sustaining therapy) and the use of appropriate devices and medication. This restriction must be present all or substantially all the time, which has been interpreted by the CRA as at least 90% of the time.
The CRA defines inordinate amount of time as a clinical judgment made by a health provider who must attest to the fact that three times the average time is needed to complete the activity by a person of the same age who does not have the impairment. We heard that there is confusion in this area and that "it is difficult to differentiate between markedly and significant."
The most problematic area arises around the interpretation of the all or substantially all of the time requirement. It has been administratively interpreted by the CRA to mean that the restrictions in activity are present at least 90% of the time. When the individual’s ability to perform a designated activity is not restricted for at least 90% of the time, the CRA may determine that the applicant is not markedly restricted all or substantially all of the time.
Since the mid-1990s, the CRA has interpreted the all or substantially all of the time clause in the Income Tax Act as being at least 90% of the time. It has applied this guideline in various contexts, including businesses and charitable activities. The CRA argues that it uses this interpretation according to the well-established principle of uniformity of expression. In other words, the same term in the Income Tax Act has the same meaning throughout the Act unless a different meaning is clearly indicated.
In 2012, the CRA revised Form T2201 by introducing the parenthetical notation of the mathematical model to describe all or substantially all of the time as being at least 90% of the time. It is of interest that there was a significant uptick in refusals in DTC eligibility in 2012. We believe that this increase was due to the explicit reference to the 90% guideline on Form T2201.
We have serious difficulties from two perspectives in the use of the 90% guideline as it applies to the DTC. First, it has no basis in law. Second, its use has been challenged by relevant jurisprudence.
From a legal perspective, the 90% interpretation has no basis in actual law. The Income Tax Act does not establish a numeric or percentage calculation for the meaning of all or substantially all of the time.
From a judicial perspective, the use of the 90% guideline as applied to mental functions in the context of the DTC, in particular, has been challenged in several judgments prepared by the Tax Court of Canada.
The problem is that the 90% guideline has created an insurmountable barrier for many individuals living with severe and chronic impairment in mental functions as well as those with fluctuating or episodic conditions, such as multiple sclerosis. In Philip Steele v. the Queen (Docket: 2001-3700-IT-I), Judge Campbell Miller addressed the fact that a mathematical model is not an appropriate measure of disability for people living with mental disorders:
"I remain just a bit sceptical that the medical profession has advanced to the point that the complexities of the brain's receipt, storage and retrieval of data can be identified with such an accuracy that would allow a psychiatrist to proclaim that an individual is unable to remember 25%, 50% or 90% of the time."
The Honourable Donald G.H. Bowman, former chief justice of the Tax Court of Canada, has ruled against the CRA's interpretation of all or substantially all of the time as being at least 90%. In Watts v. The Queen and in several other cases, the judges noted that the 90% rule has no statutory basis.
In our interpretation of these court cases, the Committee believes that even if it had some basis in law, the rule itself is defective because it leaves unanswered the question 90% of what? While the 90% rule of thumb may be convenient to assessors and tax advisors, it is difficult to apply in practice.
The Disability Tax Fairness Campaign reviewed the court case of Bruno Maltais v. The Queen and indicated that Judge Alain Tardiff recognized that individuals living with psychotic illnesses did not exhibit the associated symptoms continuously. The judge stated that:
"When the problem involves a mental disability, the exercise is much more difficult and complicated, since the outward signs are not always visible or apparent. Moreover, a person who has such a disability may break down at any time without there being any indications or warning signs."
In a submission to the Committee, the Canadian Mental Health Association noted that because the experience of mental illness is frequently an episodic and variable one, the current DTC eligibility guidelines are inappropriate for mental illness. The CMHA proposes that the CRA "revise the language around ‘all or substantially all of the time’ as well as the 90% threshold as eligibility criteria."
In fact, the data for the fiscal year 2016 to 2017 demonstrate just how difficult it has become for people living with schizophrenia, bipolar disorder and other psychotic disorders to access the DTC, even those who have been receiving the tax credit for 10, 20 and even more years and their condition has remained unchanged. The unprecedented 53% increase in the number of rejections of applications from people who are markedly restricted in their mental functions all or substantially all of the time needs to be addressed [Lembi Buchanan].
We note, however, that persons with impairment in physical functions are equally vulnerable. The Chronic Pain Association of Canada pointed out to us that chronic pain can be invisible, even to clinicians. As a result, both acute and chronic pain are outright dismissed.
The National ME/FM Action Network, which represents the concerns of Canadians with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome, identified similar challenges. Its submission calls for a fundamental review of the current eligibility criteria and the addition of a new activity of daily living to deal with reduced functional capacity. Energy or pain impairments should be recognized among the eligibility criteria. The network notes explicitly that the "90% of time phrase is confusing."
The cases involving conditions in which symptoms present themselves intermittently have proven to be particularly challenging. While the symptoms may be intermittent, the condition is ever-present. It may impair the ability to carry out the basic activities of living at any time.
In its brief to the Committee, the Multiple Sceloris Society of Canada pointed out that the unpredictable, episodic and progressive nature of multiple sclerosis makes it challenging to maintain an adequate quality of life. Qualifying for income and disability programs is difficult for individuals with MS due to the episodic nature of the disease. Periods of good health are interrupted, often unpredictably, by periods of illness or disability that affect functional capacity.
The Multiple Sceloris Society recommends that the definition of disability used in determining eligibility for the DTC be changed to take into account all individuals with disabilities, including those with episodic disabilities. The Standing Senate Committee on Social Affairs, Science and Technology documented similar concerns about the eligibility barriers encountered by Canadians with fluctuating or episodic disabilities. It noted in its Breaking Down the Barriers report:
The committee also heard about the significant barriers that people living with episodic disabilities such as Multiple Sclerosis (MS) experience when trying to access the DTC. At present, a person’s disability must last for a continuous period of at least 12 months. This is problematic for people with chronic diseases that present episodic symptoms. For example, MS is a chronic, degenerative disease with no known cure. Symptoms can come and go unpredictably, being very severe and debilitating at some times and then abating for periods of time. The current criteria for the DTC do not capture the reality of those living with unpredictable, episodic experiences of disability, even though they face the same higher costs of living, economic challenges and income insecurity [Standing Senate Committee 2018: 11].
Committee member Lembi Buchanan presented to the House of Commons Standing Committee on Human Resources, Skills and Social Development and the Status of Persons with Disabilities that imposing the inflexible 90% guideline has created an insurmountable barrier for many individuals living with severe and prolonged impairments in mental functions and episodic disabilities. Many have reported that their doctors refuse to complete Form T2201, even though they may have qualified in previous years. The Chronic Pain Association of Canada raised a similar concern.
Respondents to the health provider survey also told us that:
"The 90% impairment is very hard to understand because a person with autism has the condition 100% of the time, but apparently it isn’t impairing enough in some cases but it is in others. It seems that a different form is needed for dealing with psychological issues - the way to report doesn’t fit with the medical aspects of the form."
"My clients often have developmental disorders that may fluctuate depending on the circumstances around them. It is difficult for me to determine whether their impairments will actually be present "90%" of the time, and the potential for them to be present is 100% of the time."
"90% of the time is difficult to ascertain and it is difficult to determine the extent of the effects of mental health disorders. The (T2201) form seems more suited for medical conditions and not mental health conditions."
Our committee believes strongly that the eligibility criteria regarding the assessment of severity of impairment in mental functions must be clarified. For one thing, Form T2201 asks health providers to identify when the individual’s restriction in mental function(s) became a marked restriction. It should made clear that this question does not necessarily refer to the year of the diagnosis, but to the time when the diagnosed condition produced severe and prolonged impairments in mental functions as defined by Form T2201.
The Committee spent considerable time discussing the problems related to the 90% guideline. Our deliberations led us to oppose the application of a fixed numeric standard for DTC eligibility. While a percentage guideline may readily apply to banking and other fixed assets, it is impossible to fairly and effectively employ a numeric benchmark in the determination of functional impairment. The application of a uniform blanket rule makes no sense when it comes to assessing complex human behaviour.
Based on our review of cases of appeal, as well as on a deeper understanding of how impairments impact functioning across functions, we propose that the CRA no longer interpret all or substantially all as 90% of the time and no longer interpret an inordinate amount of time as three times the amount of time it takes a person without the impairment. The reason for this recommendation is that, upon appeal, the courts have taken the position that there is no basis for these interpretations of terms in law.
More importantly, the threshold of 90% or three times the amount of time is too high a bar for persons who are indeed markedly restricted by their impairments. A restriction that is present 50% of the time may be marked. For example, if half the time one is unable to navigate directions or dress oneself, especially if those times are unpredictable, the impact on a person’s functioning is as severe as if the restriction were present 90% of the time. We recommend:
That the Canada Revenue Agency no longer interpret all or substantially all as 90% of the time and no longer interpret an inordinate amount of time as three times the amount of time it takes a person without the impairment;
That in the DTC assessment process, the Canada Revenue Agency employ the following definition to determine marked restriction in mental functions:
"The individual is considered markedly restricted in mental functions if, even with appropriate therapy, medication and devices (for example, memory and adaptive aids):
- all or substantially all the time, one of the following mental functions is impaired, meaning that there is an absence of a particular function or that the function takes an inordinate amount of time:
- attention;
- concentration;
- memory;
- judgment;
- perception of reality;
- problem solving;
- goal setting;
- regulation of behaviour and emotions (for example, mood disturbance or behavioural disorder);
- verbal and non-verbal comprehension; or
- learning; OR
- they have an impairment in two or more of the functions listed above none of which would be considered a marked restriction all or substantially all the time individually but which, when taken together, create a marked restriction in mental functions all or substantially all the time; OR
- they have one or more impairments in mental functions which are:
- intermittent; AND/OR
- unpredictable; AND
- when present, constitute a marked restriction all or substantially all the time."
Form T2201 asks health providers whether the applicant is markedly restricted in performing designated activities related to mental functions. We believe it would be helpful to provide examples that can act as guidelines for health providers in making this determination. Many of the comments from the health providers survey support this view. We heard:
"It would be better if there were more options/examples on the form and if we could use check-boxes rather than text description. Somewhere on the CRA website, it would be useful to have examples of patients who don’t meet the criteria as well as those that do to give more education to those of us who have to complete these forms."
Our committee agrees that examples are particularly important in the case of impairment in mental functions around which there have been so many challenges in establishing eligibility. We recommend:
That the Canada Revenue Agency remove specific references to activities in the T2201 section on mental functions and include examples of activities in the current Guide RC4064 to help health providers detail all the effects of the markedly restricted mental function(s), as in the following illustration:
"The individual is considered markedly restricted in mental functions if they have an impairment in one or more of the functions all or substantially all of the time or takes an inordinate amount of time to perform the functions, even with appropriate therapy, medication, and devices. The effects of the marked restriction in mental function(s) can include, but are not limited to, the following (this list is illustrative and not exhaustive):
- with impaired memory function, the individual cannot remember basic information or instructions such as address and phone number or recall material of importance and interest;
- with impaired perception, the individual cannot accurately interpret or react to their environment;
- with impaired learning or problem solving, the individual cannot follow directions to get from one place to another or cannot manage basic transactions like making change or getting money from a bank;
- with impaired comprehension, the individual cannot understand or follow simple requests;
- with impaired concentration, the individual cannot accomplish a range of activities necessary to living independently like paying bills or preparing meals;
- with impaired ability to regulate mood (for example, depression, anxiety) or behaviour, the individual cannot avoid the risk of harm to self and others or cannot initiate and respond to basic social interactions necessary to carrying out basic activities of everyday life; or
- with impaired judgment, the individual cannot live independently without support or supervision from others or take medication as prescribed."
As we note in the recommendation, these examples are illustrative only and are not meant to be exhaustive. The Multiple Sceloris Society of Canada brought to our attention the fact that "some individuals and/or qualified practitioners look at the examples on the form and don’t necessarily think outside of the examples indicated."
Several respondents to the health provider survey identified another serious weakness in the DTC eligibility process. The current Form T2201 does not readily apply to children because they typically require assistance with most of the activities of daily living. It was felt that examples would help health providers distinguish between a disability-related limitation and a developmentally related limitation due solely to age and maturation.
We concur that examples can act as invaluable guidelines to practitioners. We believe that the CRA should include some examples that are relevant to health providers completing Form T2201 on behalf of children. Because Form T2201 is geared toward adults, young children would need a lot of assistance from parents in the criteria currently listed. Several health providers commented on this concern:
"The questions are also difficult to apply to young children with diagnoses of developmental/intellectual disability. The activities of daily living are barely learned at a young age, and therefore cannot be depicted as impaired. But we know clinically that they WILL BE impaired in the future."
"The form was mostly created for adults. Many sections do not apply to pediatric patients, especially children who have never developed and will never develop the ability to take care of themselves. Having criteria more specific for children would make the form a lot more relevant."
"The criteria are difficult to apply to children. Normal children cannot do most activities listed, hard to use the form to explain the limitations of the children. Families read the forms and say their children with conditions like ADHD (attention deficit hyperactivity disorder) should meet the criteria under mental function, but in my opinion the child requires the same assistance as any child that age. I'd love to see a pediatric specific section for kids who require extra assistance for motor skills/extra supervision due to flight risk/self-harm."
"There are incidents when infants with genetic abnormalities require a lot of extra attention between specialist appointments and added therapies. The questions (on Form T2201) are irrelevant for an infant as they are dependent. Questions such as can they toilet themselves and feed themselves do not apply to an infant but there is a definite need with the extra time and expenses required to attend to the infant’s special needs."
"I would recommend that adults and children not be lumped together in terms of what constitutes impaired functioning as their day to day reality is definitely not the same – e.g., school vs work settings."
"It is ABSOLUTELY impossible to fill out this form for children with autism and other developmental disorders. Sounds like the people who designed this form forgot about these kids....!!!"
"This form is not well laid out for pediatricians, especially pediatricians seeing younger children with developmental disorders. I am a developmental pediatrician, specializing in developmental disorders and my focus is on developmental delays (genetic disorders, intellectual delays, global developmental delays) and autism, though I do see some children with neuromotor disorders, such as cerebral palsy. I often receive back the secondary forms for young children under 5 years with global developmental delays and very low DQ's (developmental quotients) - i.e., DQs<55 as well as on children with autism. The questions related to the independent functioning (dressing, eliminating, feeding) are not applicable because of their age, and the term ‘mental functions for everyday life’ is poorly worded for young children and for their parents to read."
In order to address the multiple challenges related to completing Form T2201 for children, the Committee recommends:
That the Canada Revenue Agency consider a child and an adult version of Form T2201, with eligibility criteria tailored as necessary.
We recognize, however, that it would take time to develop a new form for children and that legislative underpinnings would need to be introduced for this reform. In the meantime, we urge the CRA to expand the list of guidelines for health providers to include examples that apply to children. This action would at least respond to the concern we heard that "clearer guidelines for parents with children with disabilities are a must." The examples should include behaviours related to developmental disabilities and autism.
Parity between physical and mental functions
We have already expressed our concern about the fact that the current eligibility DTC requirements as presented on Form T2201 set the bar higher for mental functions than they do for physical functions. In an earlier recommendation in this section, we called for parity in the treatment of mental and physical functions. The lack of parity is compounded by the fact that some of the activities of daily living on Form T2201 are indeed activities (for example, dressing, feeding) and others are functions (for example, walking, seeing). The successful completion of an activity depends on any number of biological, social and psychological functions.
In order to respect the parity principle, we believe it is necessary to make associated changes in the statement of functions. We recommend:
That the Canada Revenue Agency revise the list of functions on Form T2201 to the following:
- vision;
- speaking;
- hearing;
- lower-extremity function (for example, walking);
- upper-extremity function (for example, arm and hand movement);
- eliminating;
- eating/feeding; and
- mental functions.
That the Canada Revenue Agency, in respect of the parity principle, create a list of examples of activities for each impaired function for inclusion in the current Guide RC4064 to help health providers detail all the effects of markedly restricted function(s), as in the following proposed guidelines (this list is illustrative and not exhaustive):
- with impaired lower-extremity function, the individual cannot walk;
- with impaired upper-extremity function, the individual cannot feed or dress themselves, or cannot attend to basic personal hygiene; or
- with impaired eating/feeding, the individual cannot swallow or eat food.
As in the case of mental functions, the examples here are illustrative only and can be expanded. In addition, the list should include examples that apply to children.
In fact, we heard that it would be important to engage professionals designated for each area of functioning to create the questions that need to be asked to determine level of impairment. Form T2201 was created many years ago for specific disabilities. While it has been expanded to include a range of disabilities, it has not been tailored to them. Further, in our view, there has been insufficient reliance on the health provider community in defining and administering the eligibility criteria and communicating these on Form T2201.
The health provider survey also brought to our attention the fact that the screening criteria for some physical functions are confusing or out of date. For example, we heard the following:
"The wording of the questions related to ‘speaking’ is poor. Questions are geared only towards speaking and don’t take into account language. Communication involves the actual speech act (i.e., ‘speaking’) but also includes the ability to use and understand language (i.e., to be able to put together and understand grammatical sentences)."
"When asking whether someone is ‘markedly restricted in speaking because they are unable to or takes an inordinate amount of time to speak,’ it does not take into account individuals with a severe expressive language delay. Someone with a moderate intellectual delay and an expressive/receptive language delay would not qualify based on the wording of this question, when they definitely should. Someone may be able to speak clearly but the content of what they say and what they are able to understand is severely delayed."
"At present, the form suggests that the person must be ‘unable to speak’ or ‘take an inordinate amount of time to speak’ in order to qualify. Does this mean we should only consider clients who lack the ability to speak or have a ‘reduced rate’ of speech? What about clients who have significant difficulty understanding language? Does the wording you use mean we shouldn’t consider clients that have overall difficulty with speech and language (e.g., clients who have significant issues with speech intelligibility, clients with significant issues with social communication skills, clients with severely disordered voice)? It might make more sense to use terminology that describes the severity of the overall speech-language disorder (e.g., ‘significantly or severely disordered/delayed speech or language skills’) if that is the intent of the form.
"It is not clear that a cumulative assessment can be used and that this can include vision. I also think that it should be clear that other aspects of vision (most importantly contrast sensitivity) can (should) be taken into account as well as visual acuity and visual fields, and that the impairment from all measures of vision (visual acuity, fields and contrast sensitivity) should be considered in an additive way. There should be a specific place to indicate this."
The Committee learned as well that the screening criteria for hearing are no longer current and need to be updated. We recommend:
That the Canada Revenue Agency review the current eligibility criteria for hearing, which are out of date.
In summary, we strongly support the need to modify the eligibility criteria for mental functions, in particular, and for physical functions in order to ensure both the clinical relevance and conceptual coherence of the DTC eligibility process. We want to prevent, however, the problem that arose in the past in which the recommendations of the TAC were changed significantly upon their adoption into the Income Tax Act. In order to avoid a similar problem in future, we recommend:
That the Canada Revenue Agency work in collaboration with the Department of Finance Canada to consult with relevant health providers and stakeholders before introducing any legislative changes to the Income Tax Act with respect to the definition of mental or physical functions.
Life-sustaining therapy
Currently, applicants are potentially eligible for the DTC if they require life-sustaining therapy. A medical doctor or nurse practitioner must certify that the following two conditions are met.
First, an individual must require this therapy in order to support a vital function. This condition applies even if the therapy has eased the symptoms. Second, the applicant must require this life-sustaining therapy at least three times a week and for an average of at least 14 hours per week.
There are rules that apply to the 14-hour requirement. It includes only the time related to the actual therapy. The requirement assumes that people must take time away from their normal everyday activities in order to receive it. The time may also be spent on administering the life-sustaining therapy to a child.
However, the 14-hour time requirement excludes the time involved in several key activities:
- actions related to dietary restrictions or regimes, like counting carbohydrates or exercising, even when these activities may affect or determine the daily dose of medication;
- travel time to receive therapy or medical appointments not related to the life-sustaining therapy; and
- recuperation after therapy.
Several concerns regarding the eligibility criteria for life-sustaining therapy were brought to our attention. Perhaps most important, there are serious questions about the empirical basis for the 14-hour minimum weekly time requirement, in particular.
Our understanding is that the 14-hour condition originally was based on the estimated number of hours involved in weekly dialysis, a clearly recognized life-sustaining therapy. Dialysis treatment typically takes place three times a week for a minimum of four hours per session.
But the three-times per week and 14-hour requirement that comprise the DTC eligibility criteria are not necessarily appropriate for other treatments, even those that would qualify as life-sustaining in their purpose and their effect.
Moreover, an individual may have to receive life-sustaining therapy three times a week, but not necessarily for 14 hours a week. Our committee agreed that even 10 hours a week was a significant amount of time to devote to this purpose. Instead of requiring an account of the number of times and hours per week involved in this therapy, we agreed that the person who requires life-sustaining therapy will, by definition, automatically spend an inordinate amount of time receiving that therapy.
We heard in submissions to the Committee that the combined time requirement in terms of both minimum number of hours and weekly sessions has had the effect of excluding many applicants who receive life-sustaining therapy. They typically must spend a significant amount of time engaged in administering and/or receiving the life-sustaining therapy but not necessarily in the precise numeric requirements set out in Form T2201.
We also heard from many health providers in response to our survey that they simply are not in a position to verify the precise number of hours that an individual was engaged in a particular life-sustaining therapy. The fact that a person requires such therapy effectively means that they are spending an inordinate amount of time engaged in this activity.
"I complete DTC for patients with diabetes. The 14-hour rule does not really apply to patients with diabetes. Although they are essentially completing or planning in advance for tasks, illness, food, physical activity, changes in schedule constantly when they have type 1 diabetes. Persons living with type 1 diabetes should have a separate section to fill out in place of the 14 hours rule."
"I could not be confident that what I thought was a clear description of a disabled child would be seen as such by CRA, based on supplementary questionnaires I have received in the past. Some requirements, for example, documentation of 14 hours/week for life-sustaining therapy in type 1 diabetes, seems unreasonable. Additionally, there is pressure from families whose children do not appear to meet criteria, to complete the form indicating that the child is disabled; I would like the families to be able to clearly interpret the requirements for themselves."
Cases involving diabetes have been particularly problematic. Diabetes Canada pointed out that "the eligibility criteria as currently interpreted do not reflect the realities of administering life-sustaining insulin therapy." Living with diabetes is a 24-hour a day job. There are no days off and no vacation. It is a life-long balance of diet, exercise, blood sugar testing and medications. Yet the DTC has been severely limited for persons living with diabetes who require intensive insulin therapy, which includes:
- insulin administration by injection or pump;
- testing blood or interstitial fluid (CGM);
- matching insulin to food;
- adjusting dose of insulin for activity/illness/stress; and
- treating low blood sugars (hypoglycemia).
In 2017, Diabetes Canada and the Juvenile Diabetes Research Foundation became aware of an increased number of rejected DTC applications by people living with diabetes. These rejections included individuals who had been DTC-eligible for many years, but were now being turned down when their DTC eligibility came up for renewal.
The Standing Senate Committee also expressed concerns about this issue in its recent report:
"It was explained that persons with the same disability share similar health burdens and financial challenges regardless of the time required. For example, someone managing Type 1 diabetes experiences the same activity restrictions and higher costs associated with administering insulin regardless of whether it takes 10 hours or 14 hours per week. It was also noted that these rules can often mean that young adults cease to qualify for the DTC when they turn 18 simply because their parent’s time is no longer included in the amount of time spent administering a therapy. In reality the only thing that has changed is that the person has turned 18 [Standing Senate Committee, 2018]."
In light of all the submissions, survey reports and personal letters from applicants, our committee feels that the CRA must move away from a rigid definition and interpretation of life-sustaining therapy that excludes many potential eligible Canadians from qualifying for the DTC. The undeniable fact is that any individual who requires life-sustaining therapy, by definition, must administer therapies on a daily/weekly basis or they will not survive.
Although therapies are measurable, this is not only time consuming for the health provider, it is also costly to the individual and a challenge for CRA officials who interpret Form T2201, often resulting in clarification letters and appeals. In the case of type 1 diabetes, many individuals administer their therapies independently but would not be alive if they neglected these activities. Our committee strongly believes that in order to qualify for the DTC, this particular category could be simplified by establishing the fact that since the person is alive, they must be adhering to the therapies essential for survival.
Our committee had extensive debates about the therapies that potentially would qualify as life sustaining. We agreed that these would not include, for example, a prescription drug regime for cancer patients or an implanted pacemaker for cardiac patients. Life-sustaining therapies involve the application of a procedure on a regular and frequent basis over an extended period for the duration of a person’s life. Only a handful of life-sustaining therapies meet these criteria. We recommend:
That the Canada Revenue Agency replace the current eligibility criteria for life-sustaining therapies as set out in Form T2201 with the following:
Individuals who require life-sustaining therapies (LSTs) are eligible for the DTC because of the time required to administer these therapies. These are therapies that are life-long and continuous, requiring close medical supervision. Without them, the individual could not survive or would face serious life-threatening challenges. Close medical supervision is defined as monitoring or visits, at least several times annually, with a health provider. These therapies include but are not necessarily limited to: intensive insulin therapy for type 1 diabetes; chest therapy for cystic fibrosis; renal dialysis for chronic and permanent renal failure; and medically prescribed formulas and foods for phenylketonuria (PKU).
Designated conditions
In trying to ease eligibility through improved eligibility criteria, we discussed whether it would be helpful to include a statement of condition or diagnosis on Form T2201. While the decision would not be made the basis of diagnosis, at least an indication of diagnosis might be helpful to CRA assessors making eligibility determinations.
We acknowledge the pitfalls associated with this approach. A designated list in any area of public policy invariably raises questions of fairness about the groups, items or conditions that have been left out. A lobbying process typically begins to open up the list in order to make it more comprehensive and complete.
At the same time, however, we recognize that the inclusion of diagnosis, though not the primary determining factor, may ease DTC eligibility for many Canadians. While it would not be the primary consideration in any eligibility determination, it could help provide additional context to the assessment process. This substantiating information may reduce the time involved in decisions and the associated administrative costs.
There is precedent for the inclusion of diagnosis on the eligibility forms of selected programs. For example, the Government of Ontario includes in its eligibility for long-term social assistance, the Ontario Disability Support Program (ODSP), a set of prescribed classes.
Prescribed classes refer to specific categories of people who do not have to go through the disability adjudication process in order to qualify for ODSP income support. However, individuals in the prescribed classes must still apply and meet all other ODSP eligibility requirements. (It should be noted that the Government of Ontario recently announced a review of its ODSP eligibility criteria. The intent is to align these criteria more closely with federal guidelines.)
For the purposes of the ODSP, members of prescribed classes include persons who:
- receive Canada Pension Plan / Quebec Pension Plan disability benefits;
- are already determined eligible for services, supports and funding under the Services and Supports to Promote the Social Inclusion of Persons with Developmental Disabilities Act, 2008;
- reside in a home under the Homes for Special Care Act; or
- reside in a facility that was a former provincial psychiatric hospital.
Long-term social assistance in Alberta employs a similar approach known as straightforward medical adjudication. Under the Assured Income for the Severely Handicapped (AISH) program, straightforward medical adjudication is employed to streamline the application process when the applicant’s medical situation may not require extensive analysis. Examples include:
- palliative or terminal prognosis;
- awaiting organ transplant;
- tetraplegia; and
- severe brain injury.
In these cases, the application is prioritized for immediate review. Applicants are considered medically eligible for the program as soon as AISH receives documentation validating their medical situation. This information can be provided by the applicant or their physician as a letter or other documentation submitted in lieu of the AISH Application Part B – Medical Report. A full list of conditions potentially eligible for straightforward medical adjudication can be found in the AISH Adjudication Guide.
The Canada Pension Plan disability (CPPD) benefits give priority to those with a terminal illness so that benefits can start as soon as possible if the application is approved. Moreover, the application form for CPPD benefits requires the following information:
- medical condition;
- ICD-9-CM code (a subset of the International Statistical Classification of Diseases and Related Health Problems);
- impairment;
- functional limitation; and
- prognosis.
While functional limitation is the key criterion, other factors related to medical condition and associated impairment are considered in the assessment.
Several organizations raised this issue in their submissions to the Committee. Parkinson Canada, for example, recommended that a person with a proven lifelong mental or physical impairment should not be required to reapply for the DTC.
The National NE/FM Action Network proposed automatic DTC eligibility for anyone who has been approved for a CPPD benefit or a provincial disability plan. These cases have already been supported as having severe and prolonged disabilities. This issue is discussed more fully in Section 6 on the gateway function of the DTC.
"Patients on CPPD or provincial disability programs also have to complete the form, and may be denied. Frail elderly patients are sometimes denied. Perhaps it would be more efficient to allow CPPD and provincial disability clients the tax credit automatically. Perhaps once a person reaches 90 years of age or is admitted to a nursing home (which requires its own list of forms), there could be an automatic tax credit. This might save doctors from paperwork, which distracts time from patient care, and save administrators excess forms for limited tax revenue differences."
Several health providers concurred with this view:
"Applications of individuals who have an intellectual disability and autism are often rejected. If you are eligible for ODSP, you should be eligible for the tax credit."
"I think that there should be a list of conditions which automatically qualify. Here are some examples which would save a lot of grief for doctors: insulin dependent diabetics, dementia, any degenerative neurological disease (Parkinson’s, ALS), any stroke, spinal stenosis, retirement home or nursing home residents (who obviously had to move there for health reasons), just to name a few. I would strike a committee of medical doctors and nurse practitioners to craft a list. It is simply way too subjective in its current form."
As noted, we are aware of the pitfalls associated with expedited DTC eligibility based on diagnosis. Such recognition would open the door to continual pressure from organizations to have their specific condition included on the list.
We also acknowledge the challenges implicit in the current assessment process. A certain diagnosis does not necessarily mean serious impairment in function. In many cases, it is neither appropriate nor factually correct to equate the two. But there may well be some conditions, such as paraplegia or dementia, whose effects are more evident and predictably stable.
We note that the Standing Senate Committee recommended in its Breaking Down the Barriers report that the minister of finance revise the DTC rules to better recognize the lifelong nature of certain physical and mental disabilities and eliminate the need for these people to reapply for the credit. We support the intent of this proposal and recommend:
That the Canada Revenue Agency:
- consider whether some conditions, such as a complete paraplegia or tetraplegia, schizophrenia or a permanent cognitive disorder with a MOCA below 16, should automatically qualify for the DTC in the way that blindness does. (MOCA is a mental status examination of cognitive functions used commonly to assess impairment that results from conditions such as dementia, head injury or stroke.); and
- examine the eligibility criteria employed in other federal and provincial/territorial programs, such as the Ontario Disability Support Program and the programs for Canada Pension Plan disability benefits and, veterans disability pensions, to identify the conditions/diagnoses that establish automatic eligibility for those programs; and
That the Canada Revenue Agency examine the new eligibility form being used for Canada Pension Plan disability benefits to identify areas in which there might be synergies regarding eligibility for the DTC, such as including the presenting condition or diagnosis as supplementary information to identifying functional limitations.
Section 3 – Enabling DTC access through improved application procedures
For years, Canadians with disabilities and health providers have raised concerns about the challenges related to DTC eligibility. The challenges derive from both how the eligibility criteria for the DTC are defined in the Income Tax Act and how they are expressed on the application Form T2201.
This first component of the problem was discussed in the preceding section on enabling DTC access through improved eligibility criteria. Some of the reforms that our committee proposed in that section would require legislative amendment.
The other equally important part of the access coin stems from the procedures that the CRA employs to make decisions about DTC eligibility. This section focuses on the administrative side of the eligibility equation. Most of the administrative changes discussed below can be introduced immediately through improved practices within the CRA.
In addition to specific recommendations, we propose the introduction of a quality assurance framework that sets out procedures that, ideally, would guide decision making around DTC eligibility. They would also incorporate a method for monitoring progress on an ongoing basis toward the more effective and efficient delivery of the credit. The idea is to ensure continual monitoring and improvement of service quality.
While we are concerned with operational effectiveness and efficiency, we also believe that the DTC must fairly meet the needs of all the people it intends to serve. The submissions we received from organizations representing persons with disabilities and the results from the health provider survey made clear that the principle of fairness needs to shape decision making. We hope that a quality assurance framework will ensure a process that is more effective and efficient for government but also for the Canadians who rely on it.
As discussed in the previous section, Canadians who apply for the DTC must submit Form T2201, which is to be completed by a physician, nurse practitioner or, for specific functions, other designated health providers. Sometimes several professionals are involved in the completion of a form, either because an assessment of a person’s functional activity requires input of several providers or because different providers are involved on a case over time.
These designated health providers are the front-line partners in the application process. If they are unclear about the purpose of the credit, the eligibility criteria or the application Form T2201, the efficiency and effectiveness of the DTC and its administration are compromised for everyone. We received hundreds of comments from health providers about the eligibility process. They relate to the following areas and are discussed more fully below:
- health provider roles;
- clarity of Form T2201;
- layout of Form T2201;
- clarification letters; and
- appeals.
Health provider roles
Health providers as gatekeepers
Health providers brought to our attention the fact that they effectively have become gatekeepers to the DTC, a role that they feel is not theirs to take on and one that can compromise the provider/patient relationship. The following comments illustrate the discomfort health providers feel in taking this gatekeeper role:
"There is not enough guidance on eligibility. Clients get directed to us from MPs (members of Parliament) offices and believe they qualify (based on their interaction there). Then we are left to police this service. That is NOT MY JOB!"
"My role as a physician should be to advocate for my patient, not for the government's tax credit program."
"The whole idea that the physician plays the role of gatekeeper for monies affects the patient-doctor relationship. Despite what I think was a clear explanation of disability, it felt like almost all the forms I filled in needed the secondary assessment."
"As a practitioner I don't want to be the gatekeeper for whether or not people get benefits. But I also don’t want to be filling out unnecessary paperwork for people who will not qualify. I would like to see more information given to clinicians to help guide us."
"The standards for eligibility vary widely among professionals. Everyone has a story of Uncle Fred or their neighbour whose "helpful" doctor uses a lower standard than I do. And even the most sincere and honest people feel insulted or hurt that I am "denying" that they have a problem. I’m not denying their problem, I am making a judgement that their problem does not meet the spirit of the criteria this credit is meant for. I consider myself an affable doctor and an advocate for my patients. But these forms put me into conflict with my patients, or conflict with my conscience..... and that is not something I appreciate."
The health provider experiences illustrated above lead us to encourage the CRA to explore other options for gathering some of the information it requires regarding impairment in physical and/or mental functions. We recommend:
That the Canada Revenue Agency test or pilot various approaches that would remove the gatekeeper role from health providers. One such approach would be for community tax clinics to take on a screening or advisory function. Another would be to establish a CRA call centre explicitly for this function.
When tax preparers/promoters and health providers disagree on eligibility
Several health providers noted that they are often placed in a difficult position by tax preparers/promoters or financial advisors who encourage individuals to apply for the DTC. It may well be that some tax preparers/promoters are insufficiently aware of the eligibility requirements.
It is also possible that some tax preparers/promoters may feel that applying is worth the risk of rejection, perhaps underestimating the burden posed on health providers and the CRA when people apply who are clearly ineligible and the emotional burden on people whose expectations are dashed when their applications are rejected. Health providers, tax advisors, and other individuals appear to commonly share in a lack of clarity about disability-related tax measures in general, and the DTC in particular.
When asked to complete an application for individuals, especially ones whose advisors have recommended application, health providers often feel pressure to exaggerate the impact of an impairment in function or, alternatively, refuse to complete Form T2201 altogether. Either option is not desirable, as several health providers pointed out in their survey responses:
"Sometimes I am finding a lot of patients are sent in by their accountants who have told them they qualify for the credit when it's clear that they do not qualify; this sometimes causes annoyance on the basis of the patient when I explain this. I would appreciate CRA providing clear and simple information for patients (and accountants) which would reduce unnecessary office visits and likely reduce CRA's need to audit."
"At present, thanks to private companies touting for business, everyone thinks they are eligible! It is a huge source of disagreement with patients. I frankly hate it."
"The definitions are difficult to interpret and hard for patients to understand. Most patients who bring the forms do not qualify per the definitions and are upset about that because their accountant assured them that they would."
"You also have a lot of accountants who give out the form (T2201) so the patient expects that we will fill it out. I think there should be some form of preliminary triage before the client comes to us to have it filled out."
"I would like to see more information given to clinicians to help guide us. But I also think that perhaps a process should be in place where not just anyone can access the forms. Maybe patients should have to go through a screening process to determine if it is even worthwhile to have it filled out. I get so many requests patients just print the forms off the Internet and expect that it will be completed."
"Most patients who bring in forms at the urging of their tax preparer do not qualify and it takes ages to explain to them why not. These forms take up ever increasing work time, at the cost of other work that could be done, like patient care/seeing patients/taking on orphan patients."
"I end up in unpleasant disagreements with patients. They come with forms from their accountant or therapist or — worst of all — the companies that charge people to provide a form, then advise them not to take no for an answer."
"It is not clear for many to understand why they do not qualify. There are people helping citizens to complete the forms at a cost to the citizens and these people are not health care professionals. Perhaps since CRA is offering this, CRA needs to hire providers to assess citizens and with the citizen complete the forms for tax paying citizens for the credit and then request specific reports from the citizen’s health provider."
To address the depth and breadth of DTC understanding among tax preparers, the Committee undertook a tax preparers survey, which we hope will inform a next set of recommendations related to this key stakeholder group.
When health providers may not have the information base necessary to completing Form T2201 on behalf of applicants
The Committee heard from many health providers who indicated that they often felt insufficiently qualified to respond to the questions on Form T2201.
"Parents, teachers and other support workers know exactly what is going on with these patients. As the consulting physician, I do NOT make home visits, nor provide day-to-day care, nor have any other way to "give specific examples of the patient's severely disabling condition." I CAN affirm that I believe the parent/teacher/support worker's information, yet when I do so the family's application is denied (because "your physician did not adequately describe the patient's disability"...)."
"We have to estimate when a disability began when we may or may not have possession of this information."
"Part 2 of the form (T2201) is difficult to complete because it asks very personal specific questions that I might not have the current information for and I feel could be better answered by the family directly rather than a physician."
When an applicant has more than one severe and prolonged impairment in an activity of daily living
Health providers also told us about the complications that can arise when an individual has more than one impairment requiring multiple providers to fill in Form T2201. There appears to be a lack of clarity as to when and how multiple providers might be needed to complete the form. For example, we heard the following:
"Certain professionals are required to fill out specific areas only, meaning the client/family needs to go to multiple practitioners to receive accurate information, as typically the family's/client’s GP is the least frequent professional encountered by the client."
"As occupational therapists, we can only complete parts and then the doctors have to complete other parts, which makes things difficult for clients. In addition, there is nowhere on the form to indicate if you fill out parts and the doctor fills out parts, so you end up signing in weird places and hoping it doesn’t work against your client somehow."
"Even after you have tried to explain on the form, there is usually another form to fill. It also seems the forms filled by specialists get approved as if a patient is more worthy if they are followed by a specialist, which is not always possible in a small community."
"The various components (of Form T2201) don’t have a separate section for signature. If the client had that section completed by another provider, the list in the form/these cases can be almost endless - an optometrist or audiologist, or speech/language person. It is very reasonable, indeed sensible, to have more than one type of provider filling out the section that pertains best to their expertise. So why does the form lack a signature line for that input/section?!"
"It is unclear to families how many professionals they need to complete the form as I can only fill in one section."
Expanding the list of health providers qualified to complete Form T2201
Finally, we received submissions from a number of organizations representing various health providers who asked that the list of designated assessors for Form T2201 be expanded to include their members.
The Canadian Chiropractic Association made the case for including chiropractors in the list of health providers who can assess for impairment in walking and upper-body mobility. Its submission was supported by the Arthritis Society, which encouraged "the Government of Canada to fix a serious oversight in the Income Tax Act by including chiropractors as qualified assessors to determine eligibility for the disability tax credit."
We also heard from Ostomy Canada, which pointed out that an increasing number of individuals living with an ostomy are being refused the DTC. It noted that the majority of medical practitioners listed as DTC authorizers have little experience with the individual living with an ostomy. Ostomy Canada recommended that nurses specializing in wound, ostomy and continence be added as health providers to certify impairment in bowel or bladder function.
In addition, the Canadian Association of Social Workers reached out to Committee Co-Chair, Dr. Karen Cohen, asking that registered social workers be considered for inclusion on the list of qualified health providers able to complete Form T2201 in the area of mental functions.
In our view, one significant concern has to do with client access. We asked ourselves whether Canadians are experiencing a serious problem when it comes to accessing health providers who can complete Form T2201.
We are keenly aware of the fact that there are critical access problems in the North, other remote parts of the country, and in rural areas. This concern was brought to the attention of the TAC on Tax Measures for Persons with Disabilities and there is no question that the problem remains to this day. We heard, for instance, from a health provider who told us:
"In New Brunswick, it is extremely difficult to access formalized psychoeducational assessments thus these applicants get screened out."
The problem of enabling access to the DTC was addressed partly through the inclusion in 2017 of nurse practitioners on the list of health providers who could assess functional impairment for all of the basic activities of daily living on Form T2201. While we believe that access problems still exist, we would like to have more information about the depth and breadth of these challenges prior to drafting any formal recommendations in this area.
We want to understand the precise nature of the access problem and to explore the most appropriate remedies. We plan to gather information about this and other issues by asking current and former DTC recipients about any challenges they may have faced in getting a health provider to complete Form T2201 on their behalf. The Committee is developing a client experience survey that will mirror the health provider survey we administered in June and July 2018.
We will ask specifically about any problems regarding access to health providers who can certify for the DTC. We want to collect information on which function or with which professional, in particular, access problems were encountered. We recommend:
That the client experience survey on the DTC and other disability tax measures to be carried out by the Canada Revenue Agency include a question as to whether the applicant or recipient had any difficulty accessing a health provider for the purposes of completing Form T2201 and, if so, for which activity. Clients should also be invited to provide any additional comments on this question. Special attention should be paid in this survey to the needs and concerns of Indigenous Canadians.
Of course, the Committee recognizes that we will be surveying the views of Canadians who have successfully applied for the DTC. We would also be interested in hearing the access challenges faced by individuals who were refused the DTC.
Once we have a better idea about the access problem, it will be easier to determine whether there is a need to expand the list of health providers on Form T2201 related to access.
We recognize that there are other variables related to the review of the eligibility of health providers to sign Form T2201. A set of identified principles or criteria would have to be developed to help guide expansion of this list. Our committee proposes that the CRA do some preliminary work on this question. We recommend:
That the Canada Revenue Agency develop a process for expanding the list of health providers with the appropriate expertise who can assess eligibility for the DTC.
Costs of completing Form T2201
Completing Form T2201 for applicants, especially when clarification letters are involved, imposes a significant burden of time on health providers, time which is largely unremunerated. As an example,
"It can be time consuming to do a clinical file review to answer all questions about age of onset, impact on daily life activities, and projected outcomes for children with speech difficulties, especially when you only see a child in one clinical setting."
Because many health providers are not compensated adequately or at all by the health care system for the time they spend completing Form T2201 or providing follow-up clarification when requested, many providers charge a fee to the applicant. This fee can be prohibitive, especially for individuals living on low income. We discuss this issue in Section 6 on the costs of disability.
Clarity of Form T2201
One message that we heard clearly and consistently from organizations representing persons with disabilities and health providers had to do with confusion related to Form T2201. Our committee recognizes the challenges involved in creating a form that will satisfy everyone, given the lack of clarity in the underlying legislation. The complex and confusing criteria, as well as the associated explanations on the current form, make it difficult for Canadians with disabilities to determine whether they are eligible for the credit. It is simply too hard to ascertain from a basic review of the eligibility criteria and the application form.
If Form T2201 is confounding for the average person who must self-assess, then it is doubly challenging for the health provider who is expected to complete it on the applicant’s behalf. When completing the form, they are not assessing or diagnosing the individual’s health condition but rather assessing the functional effects of that condition, effects which they often cannot directly observe (for example, health providers do not see the individuals daily or in their daily lives to confirm how much time they spent on some activities or if they are unable to do others).
Some health providers even expressed confusion about the purpose of the DTC.
"The overall purpose of the credit is unclear as are the specific categories – e.g., the degree of impairment required to qualify and the purpose of the money to offset unusual care costs. Lots of people have some problems but the degree of severity for the tax credit is very unclear and it can be hard to understand if it is an appropriate request."
In terms of specific problems, the responses to the health provider survey were overwhelmingly consistent. There was widespread consensus that the DTC eligibility criteria appear to be subjective and the operational definition of what comprises a disability is unclear at best. Here is what we heard:
"The criteria that are required to indicate whether or not someone is eligible are VERY vague. As a result, there is a great deal of confusion among practitioners and families, about who qualifies, particularly what markedly restricted means and what skills should be markedly restricted. I have had many families ask me to complete the DTC when their children do not qualify. However, they know someone who managed to find a practitioner who would complete it for a disability that does not result in marked restriction (for example, some learning disabilities, children with ADHD [attention deficit hyperactivity disorder] who still function relatively independently)."
"It is very ambiguous especially from a patient’s point of view. It should be clear, it is not based on diagnosis, and extremely strict guidelines need to be stated."
Other health providers told us:
"The definitions of disability are very hard to interpret. It is difficult to assess what 90% of the time means. It is so broad that I cannot answer without feeling I am underestimating my clients’ disabilities or conversely, that I am exaggerating the symptoms. It is also unclear what amount of reports would be beneficial to include without providing too much information (in the spirit of protecting clients’ confidential information). Finally, I’m not comfortable with not knowing the qualifications of the persons reviewing the files and the psychological information provided."
"The wording of the items is neither clear nor easy to interpret, especially when we are asked to describe level of impairment and what is considered significant."
Still other respondents noted the following about Form T2201:
"It does not give the practitioner enough guidance about what the difficulties really are. For example, anyone with a back or knee issue will say they are restricted from walking. But what does restricted mean? If they are able to work, attend to activities of daily living then do they really qualify? And the way I interpret the mental functions necessary for everyday life is basically the patient would have to be in a group home to qualify (or at least need someone to attend to their personal care). But other practitioners interpret it differently. The cumulative effects part doesn't make any sense. I am trying to figure out the amount of detail required to support a patient’s application."
"The criteria are vague and yet difficult to understand. For example, it seems that difficulties in daily living activities are favoured over behavioural, communication, social or academic difficulties. Formal evaluations are not valued with standardized tests."
While we can provide a more extensive listing of responses, they are all variations on a theme: confusion and lack of clarity regarding definitions of disability for the purposes of the DTC. There was also uncertainty with respect to the supporting documentation necessary to make the case. "I am trying to figure out the amount of detail required to support an individual’s application."
While confusion about mental functions in particular ranked high on the list, concerns regarding other conditions were noted as well. Form T2201 provides little guidance around specific conditions.
"The definition of a marked restriction in speaking is unclear, especially when it pertains to speech disorders that are variable like stuttering."
"How does dressing being affected by arthritis? Is it taking an inordinate amount of time compared to someone their age?"
There was uncertainty as well about reporting on the impact of a given condition and the activities of daily living.
"The form will say that functioning in school is part of the definition, but then we will be told that a client’s form was declined because school functioning was mentioned."
Health providers often second-guess whether their answers are written in a way the Agency will accept.
"Without clearly knowing the criteria for qualification or why certain questions are asked, it’s hard to know how the clinical descriptions will be interpreted by the CRA."
"The criteria are not clearly laid out and seem to change with how they are supposed to be interpreted."
"I typically complete these for individuals with autism for whom I have made a diagnosis. The criteria seem to be set up for medical disabilities and don’t clearly fit the disabilities experienced by this population. Also, autism is present early on (generally from birth), yet I would not have records on hand to document this (as asked for) other than parent report so I don't know how I am supposed to answer this question."
Other evidence of the lack of clarity is the perceived inconsistency in the application of definitions of eligibility. Health providers who complete forms for many individuals, as well as organizations representing persons with disabilities, expressed their concern about apparent inequities in the treatment of individuals with similar conditions.
A psychologist who specializes in autism, for example, will see many children with autism and can witness first hand any inconsistency in how applications are adjudicated. A number of health providers raised questions about CRA decisions that appeared inexplicable based on applicants’ assessed ability to function.
"There seems to be variation in who gets the tax credit based upon the particular words or wording used and this is not clear to the person completing the form. I have had several people approved and others not approved and it remains absolutely unclear to me how their disabilities and effect are not equivalent day to day."
"Qualified families are refused or challenged but less serious cases are accepted. Many families are encouraged to have the forms filled out by various practitioners or tutors but really probably don’t meet the criteria."
"For the mental health section, please ask us to complete a scale or two. Let us know what the score needs to be to qualify and we can proceed. You do this with visual acuity and walking. Why not mental health? Unless you want to maintain your discriminatory practice."
"I have had cases that I had advised the parents to not expect being accepted (as I did not deem their child’s symptoms to be severe enough to warrant applying for disability status) who were approved, and I have had families with children with severe chronic and lifelong disabilities (e.g., severe intellectual disability, severe autism spectrum disorder, severe ADHD [attention deficit hyperactivity disorder] and several complex medical conditions) who were refused, despite having several medical specialists having also completed their own application forms which accompanied my form."
"One of my major issues is a lack of consistency from CRA regarding which applications are approved and which are not and a seemingly shifting bar for who gets approved. I work on an autism spectrum disorder (ASD) diagnostic team so the majority of applications I fill out are for this. I have begun asking my clients to let me know if they get approved or not so I can get a sense of whether I am putting in sufficient detail and the level of severity necessary for it to be approved by CRA. I can honestly say that it seems like it depends on whose desk it lands on as to whether it gets approved. In the distant past, it seemed like all ASD applications were approved but now there seems to have been a bit of a crackdown on ASD in that many more applications are getting rejected (or I am at least asked to provide more information). There was also one case where a mother applied several times and was not approved (with a CLEARLY impaired child). On the other hand, I have sent in applications which I thought may or may not be approved and they were approved with no request for more information."
The Committee recognizes that inequities invariably will arise in the treatment of individuals with similar conditions. Eligibility for the DTC is determined not according to diagnosis or condition but rather on the basis of impairment in physical and/or mental functions. It is understandable that individuals with a similar condition may be affected differently and subsequently assessed in very different ways.
However, there were far too many cases brought to our attention in which persons with moderate functional capacities appeared to qualify for the DTC with relative ease while those who were far more severely impaired in their functional capacity were refused eligibility. Regardless of the eligibility criteria, these must be consistently applied. When they are not, it may signal that CRA administrators experience the same lack of clarity as do Canadians, health providers and other stakeholders in the DTC eligibility criteria.
Our proposed changes to the eligibility criteria and administrative procedures ideally will address the apparent inequities in the current decision-making process. We also hope that the suggested implementation of a quality assurance framework will improve the overall process to establish eligibility to make it fairer and more equitable.
Layout of Form T2201
In addition to the clarity of terms on Form T2201, we heard concerns about its layout. The following illustrate the nature of the comments we received:
"The instructions are NOT clear and questions are NOT clear. The application is VERY lengthy!"
"I would like more written information on the form (for the patient) regarding what renders a patient disabled."
"The fillable form has little space to write. The definitions and examples make it challenging to complete."
"Each section should have its own comments section. Also, I’d appreciate a more thorough handbook for completing the form."
"There is too much subjectivity in the narrative format and the form should be completely overhauled to ensure that there is standardization across different people and providers - remove what appears to amount to potential for narrative bias or inequity as that is not a true representation of disability."
Some health providers felt that the form did not allow sufficient space for the inclusion of detailed information. Others proposed the inclusion of standardized boxes that could be answered with tick marks.
"There is insufficient space to justify limitations and deficits. Often, if we limit ourselves to the space offered, the request is refused. The criteria are not very clear for disability in cases of behavioural disorders, ADHD, anxiety and other psychological and neuropsychological disorders."
"I wish it was tick box style so we could describe better how it is affecting their life."
"We need clearer instructions on inclusion and exclusion criteria. These should be given to patients seeking DTC first and foremost! Check boxes would make it easier to complete as well for providers."
"The questionnaire that is often sent in response to the initial application could be more easily completed in PDF form instead of a form that must be completed manually."
Several health providers and organizations representing persons with disabilities noted that there is nowhere to turn for help if they require assistance or clarification with respect to any aspects of the form. We discuss this issue in Section 4 on improved CRA communications.
Lack of clarity around the initial form gives rise to additional problems down the road. For example: The CRA claims that there is insufficient information on the form to make a decision and sends out clarification letters to request substantiating evidence. The wide-ranging issues identified in relation to clarification letters are discussed below.
Clarification letters
One of the most frequent concerns raised by health providers and organizations representing persons with disabilities had to do with the CRA request for clarification of the information submitted on Form T2201. In fact, we heard clearly and frequently about an apparent increase in recent years in the frequency with which clarification letters are sent. The Committee noted that it would be helpful to have data on the number of clarification letters, along with the type of function for which additional information is being requested.
The CRA sends clarification letters to health providers in order to request additional information regarding the initial Form T2201 completed on behalf of the applicant. From the health providers’ perspective, receipt of a clarification letter can be summed up simply as the bane of their professional practice.
The multiple concerns cited around the clarification letters can be grouped into six key themes:
- purpose of the clarification letter;
- substance of the clarification letter;
- challenge to professional competence;
- losing eligibility;
- time and cost involved in completing the request; and
- lack of transparency.
Purpose of the clarification letter
With respect to the first concern, many health providers questioned the purpose of the clarification letter as well as the CRA’s intent in sending it. Respondents were asked to provide additional information after they had already submitted substantial documentation in the initial application.
There was also a sense on the part of many organizations and health providers that individuals with certain conditions are targeted by the CRA in that they are consistently asked for substantiating information for individuals with those conditions.
The organization Centre intégré du réseau en neuro-développement de l’enfant (CIRENE), a special project of health providers in Quebec who specialize in the early screening and diagnosis of neurodevelopmental disorders in children, stated in its submission that its professional members correctly complete Form T2201. Yet they still receive clarification questionnaires asking them for information they have already provided on the form.
Many health providers also had concerns about the need for these letters. We include here a sample of comments we received:
"All information is provided as directed and is VERY detailed. However more often than not, a follow-up request for information is made. The information provided on the follow-up request is EXACTLY THE SAME as the prior report. Very frustrating for both the practitioner and the client. Furthermore, the criteria seem to be fluid and change from year to year. Approval of the DTC is not consistent from year to year, even for the same conditions that will not change."
"It is terribly redundant. The second form that is sent requesting further clarification in 100% of cases is very frustrating as I end up re-writing essentially the SAME information again a second time. It seems to me that this form should be filled out by CRA employees rather than medical professionals who are already overburdened."
"The initial form is never accepted as completed, but with same information entered on a supplemental form it is approved. No changes or additional information added. That should not happen."
"No matter what I write and check off on a T2201, I get a second form asking more questions."
"Even though information and examples of the impact of a disability on mental functions are provided, additional information is often requested in the form of a questionnaire that requires the provision of the same information already provided."
"It does not capture the scope or diversity of psychological impairments... my patients are uniformly turned down, return to me, and then I must charge them to complete an assessment and write a detailed report summarizing the results of psychometric testing."
"For autism spectrum disorder, there is almost 100% chance there will be a secondary form to complete. Children with type 1 diabetes were being refused for a time with no warning or explanation."
"I find the criteria to be too narrow and not at all realistic. I have patients who are severely impacted and do not qualify. There seems to be always an initial refusal and the need to appeal and go through the process again."
"It is difficult to describe cognitive impairments in the questions related to ‘daily life.’ I always attach an extended description to make the connections for the assessor, but since I get asked for additional clarification every single time, apparently the question and criteria aren’t clear or the assessors aren’t qualified to understand the answers. Very frustrating."
"I work with individuals with autism. They are routinely refused by the CRA, as the impact of their disability, language mental functions and mental health don’t fit easily into the CRA forms. This is a great prejudice to my clientele, and they are grossly underserved and need a disability tax certificate in order to offset the cost of services provided."
"Regardless of what is written on the form, you will request further information. Why not just ask the first time? Or read the information on the form."
"I find the process is not straightforward. I provide a lot of detail on the initial form but am always sent the audit form asking for additional detail. If the audit form is standard, why not include these specific questions with the initial application? It gives more specific information about the areas you are looking for. I also think the initial form should be more specific about which mental functions are considered relevant for the DTC."
There was a sense among some respondents that the CRA was simply asking for more information in order to delay a decision and/or try to deter applicants from pursuing the DTC. In many cases, health providers repeated the same information submitted in the original application, because there was nothing new or additional to provide.
"You ask questions that I feel I have clearly answered, and in the last two years I get another form 3-5 months later asking for more information. I feel you are just pushing to see if people will give up."
Equally serious were the questions raised about the validityof the request. Many health providers indicated that they had filled in the original form both comprehensively and diligently. While they were asked for additional information, it was not always evident which parts of their submission required clarification.
Substance of the clarification letter
In terms of the substance of the clarification letters, many of the questions in these letters are too broad and not always relevant to a specific disability. While the questions generally are not legal tests to determine eligibility for the DTC, a negative response (that is, a no reply) is often used as a conclusive test to deny the DTC. The narrative information is not always helpful to CRA staff who have no specialized medical training.
Some of the questions in the clarification letters rely on a health provider’s recollection of the individual’s medical condition. In fact, the responses may involve some guesswork, since many of the answers are not in the clinical record when the individual signs off on Form T2201 authorizing "the medical practitioner to provide or discuss the information contained in those records."
Challenge to professional competence
Several organizations and many health providers raised a third issue about the clarification letters: challenge to professional judgment and clinical expertise by assessors who appeared to have insufficient training to make complex eligibility determinations concerning health conditions. We heard the following:
"The vague and subjective criteria for cumulative effect seem to disregard providers’ opinion."
"One man, a CFS (chronic fatigue syndrome)/fibromyalgia patient with chronic depression, paid for me to write a 3-page summary of his health, to send with the initial form. I got that second letter back, saying I hadn’t given enough information! I have been so frustrated, I have recently been refusing to fill out this form. It is a waste of my time and a source of remarkable discouragement and disvalidation for my psychiatric patients. Some I have applied for twice... and been refused. I do not want to talk of this more, I just get furious."
"They constantly send back forms with requests for ‘more’ information when the information is already contained in the initial application. It often appears that it is done to discourage clients or delay the process. Or else the individuals reviewing the information do not understand it."
"The form requests information about mental abilities and impact on function. On multiple occasions when I have provided information, including results of standardized assessments and detailed information about the patient's activities of daily living, I have still been asked for further information."
In its recent report Breaking Down the Barriers, the Standing Senate Committee on Social Affairs, Science and Technology also expressed concern about this issue. It noted that all DTC applications must be certified by a medical practitioner. Yet the CRA exercises the right to question the descriptions of disabling effects of the impairment provided by qualified health care practitioners in both Form T2201 and the follow-up clarification letter [Standing Senate Committee, 2018].
Our committee is concerned that the CRA is able to effectively disregard the supporting objective medical evidence submitted by health providers, not only on Form T2201, but also in the clarification letter. The CRA justifies its authority to question medical evidence on the grounds that it is responsible for the administration and enforcement of the Income Tax Act. Subsection 220(1) provides that "the Minister shall administer and enforce this Act and the Commissioner of Revenue may exercise all the powers and perform the duties of the Minister under this Act."
We understand and respect the fact that it is both the role and responsibility of the CRA to administer the Income Tax Act in good faith. That good faith involves both clarification and rejection of applications as appropriate. But it should not involve almost certain questioning and challenge when it comes to the assessment of health conditions, as has become most evident for mental functions and, more recently, type 1 diabetes. As noted in the introduction to this report, there has been an uptick in clarification letters and rejections related to type 1 diabetes, in particular.
The report of the Standing Senate Committee quoted the testimony of Lembi Buchanan: "Unless there is clear evidence of fraud, the CRA should not have the authority to disregard medical evidence certified by qualified health care practitioners acting in good faith" [Standing Senate Committee, 2018: 12].
We are particularly concerned about the seemingly constant challenge of applicants with serious impairment in mental functions. We propose that additional measures be put in place in to ensure a second opinion when it comes to applicants who are refused the DTC in the face of duly completed T2201 forms and the provision of substantiating information.
When an applicant with an impairment in mental functions is denied the DTC even with a duly completed Form T2201 and supporting documentation, the CRA should require a second internal review from a different set of CRA assessors.
Ideally, the CRA would carry out a second-level internal review on all rejected applications with duly completed T2201 forms. While we favour that approach, we recognize the time and costs involved in that process. Moreover, we are especially concerned about the cases involving impairment in mental functions, because this area continues to be so problematic from an eligibility perspective.
If the second-level internal review still rejects the applicant, we propose that the CRA request a consultation with independent external reviewers to get an outside expert opinion on the refused cases. In fact, an outside expert advisory committee could be struck for this purpose. We recommend:
That in the case of determining DTC eligibility for persons with impairment in mental functions, the Canada Revenue Agency include relevant specialized health providers, including, but not limited to, psychiatrists and psychologists, in the review process when applications are disallowed.
Losing eligibility
Another area of concern related to respect for professional judgement is when DTC recipients lose eligibility. Too many Canadians with disabilities, even those who have received the DTC for 10 years, 20 years and more, have lost access to thousands of dollars from income support programs on questionable grounds, often disregarding the medical evidence submitted by health providers even though their condition remains unchanged.
As an example:
"I have been asked to provide an update about whether a patient still has Down syndrome and an intellectual disability. These are not diagnoses that go away. By definition, an intellectual disability diagnosis means that the patient's daily functional abilities are significantly impacted."
In the preceding section of this report, our committee addressed this concern. We recommended that the CRA consider a list of conditions that by any health definition are permanent, with associated permanent and significant effects on impairment.
Time and cost involved in completing a request
In terms of the fifth key concern around the clarification letters, health providers noted the time and cost involved in providing more information for the requested clarification.
"I almost ALWAYS get a request for more information even though I have been quite thorough and detailed in the free text field. This is problematic because then I need to bill the patient a second time for my uninsured time to complete the form and I often end up repeating myself."
"The detail needed to complete, structure of the forms/vague questions whose possible responses are ill/barely defined, and time crunch of providers presently, especially those of us in specialty clinics caring for clients with no primary health care provider, make it challenging to complete these."
"There is nowhere to elaborate on a client’s function. Typically, I receive an additional form to fill in from CRA and often it is long after the initial form is sent in. It is a waste of my time and clients’ time to fill in a form more than once."
"I endorse the T2201 for clients ONLY when I think they are eligible and then CRA sends me a form asking me for more information. It’s highly time consuming and a burden to complete."
We agree with the Standing Senate Committee’s conclusion that the clarification process represents a significant burden to both applicants and health providers:
"This administrative practice adds unnecessary stress, time and expense for those who are entitled to benefit from the credit. It also results in an unnecessary strain on resources within the medical community and the public sector, given the need for qualified practitioners to complete forms, public servants to adjudicate applications and government lawyers to defend appeals" [Standing Senate Committee, 2018: 13].
Lack of transparency
Finally, our committee had numerous and ongoing discussions about the lack of transparency throughout the DTC eligibility process.
The notice of determination does not always provide a reason for disallowing the DTC but relies solely on verses that have little, if any, relevance to the applicant. While the CRA notice of determination may reference additional information submitted by a qualified health provider, it does not include a copy of that information, even though the document is essential for appealing the decision.
Moreover, neither the clarification letters nor their responses from health providers are sent to applicants before or when they receive the notice of determination regarding their case. This process makes it difficult to figure out whether to launch an appeal of the decision, as applicants are lacking the substantive information upon which the determination decision was based.
As noted earlier, the CRA is asking health providers to comment on impairments in daily living that few observe first hand. It is possible that the information provided by a health provider is not always entirely accurate or complete.
The materials that health providers submit in response to clarification letters are particularly important in that their replies are often the basis to disallow the DTC. Yet applicants have no knowledge of the information request unless they are expressly notified by their health provider.
This practice is a change from the past in which the CRA copied applicants when a clarification letter was sent to the health provider. That process enabled applicants to be present when the health provider responded to the clarification request. Many of the questions, as noted, require health providers to speculate about the individual’s activities around the clock.
In short, we are concerned about the fact that the CRA withholds valuable documentary evidence, such as the clarification letter requested of, and completed by, a health provider, when the notice of determination is sent to the DTC applicant. The CRA explained to us that the clarification letter is not included with the notice of determination for several reasons.
The CRA contends that taxpayers should be speaking with their health provider about any information sent to the government on their behalf. The information submitted by health providers is considered confidential between the health provider and the CRA. The CRA does note, however, that Canadians are welcome to contact the CRA and request a copy of this letter at any time.
We disagree with these arguments. The contention that communication between the CRA and the health provider is confidential is problematic. Since individuals own their health information in Canada, it is difficult to understand how one’s health information can be the basis of a confidential communication between parties that don’t include the affected individual. Moreover, the inclusion of applicants themselves in the information exchange would enhance the accuracy of information understood and conveyed.
Finally, our committee believes that it is essential for the CRA to apply transparency throughout the eligibility process. Such transparency would reduce the stress, time and cost involved in applying for the DTC. A more open and respectful process would also reduce the need to appeal CRA decisions regarding DTC eligibility.
We are hopeful that the suite of recommendations we have proposed for more clear definitions of impairment in physical and mental functions and for improved administrative processes will reduce the need for what appear to be automatic clarification letters. At the very least, we believe that the quality assurance framework, discussed below, will help address some of these identified problems.
Yet even with improved administrative processes, we recognize that, for some applicants, clarification letters as well as appeals will be necessary for a fair and transparent process. It is therefore essential to ensure that all relevant information upon which determination decisions are made be shared with applicants at every step of the application process. We recommend:
That the Canada Revenue Agency:
- copy to the applicant all clarification letters sent to the health provider;
- let the health provider know that all communication to a health provider about an applicant will be copied to the applicant and that any communication the health provider submits to CRA will also be made available to the applicant;
- encourage the health provider to contact and consult the applicant as necessary when providing any clarification to the CRA; and
- extend the time for a health provider to file a clarification letter with the CRA from 45 to 60 days and note this timeline on the first page of the questionnaire; and
That the Canada Revenue Agency:
- provide in notice of determination letters a relevant reason as to why a DTC application was denied;
- include in notice of determination letters a copy of the clarification letter and the health provider’s clarification response. This information is vital in case of an appeal; and
- move the consumer survey request to the bottom of the notice of determination letters.
Request a review / Appeal a decision
An appeal process is critical to any fair and transparent process. The process to appeal the rejection of a DTC application is described below.
Prior to a formal appeal process, individuals may write to the appropriate tax centre to request a review of their DTC application. They may also ask their health provider to write a letter and provide any relevant health-related information or reports that have not already been submitted to the CRA. This supplementary information should describe how the impairment affects the activities of daily living. Alternatively, they can reapply for the DTC by submitting another Form T2201 with new information at any time.
Individuals who do not agree with the determination through the review process may subsequently file Form T400A, Notice of Objection – Income Tax Act, (although a letter is also acceptable). The decision would then be reviewed by the Appeals Branch of the CRA. The objection must be filed with one of two regional tax offices of the CRA within 90 days of the date of the notice of assessment disallowing the DTC. As in all other federal appeals, the applicant may be represented by an agent, such as a relative or friend, or may retain a lawyer.
If the objection is disallowed, a notice of appeal may be filed with the Tax Court of Canada within 90 days of the date of the notice of confirmation from CRA. A letter is also acceptable. As noted, the applicant may be represented by an agent, such as a relative or friend, or may retain a lawyer.
The May 2017 Report 2, Income Tax Objections – Canada Revenue Agency by the Auditor General of Canada found that 8% of the objections filed each year with the CRA involved an alleged misapplication of laws, facts and policies by the CRA. It should be noted that the reference to 8% of the objections includes all objections. A breakdown of this overall figure found that DTC objections related to a misapplication of the law/facts/policies represented less than 2% of the DTC cases received by the Appeals Branch. This means that for the 2016 to 2017 fiscal year, the CRA staff incorrectly applied the law to 436 out of 21,795 rejections for the category of mental functions and 903 out of a total of 45,157 rejections in all categories.
In recent years, approximately 10% of the individuals who were disallowed the DTC filed an objection with an average success rate of 55%. The majority of these cases were successfully reversed as a result of additional information provided to the CRA by the individual.
In the past five years, the CRA processed 139 cases related to a DTC claim that moved beyond the objection stage and resulted in a notice of appeal filed with the Tax Court of Canada. Taxpayers were successful in claiming the DTC in 58% of the cases. A number of the successful cases were resolved before there was a formal hearing with a judge.
Very few individuals consult a lawyer. The system is too complicated and the costs too high to fight decisions made by a government agency. Although the odds favour the applicant when appealing a decision disallowing the DTC, the low rate of objections reflects the difficulty of filing an appeal. Compounding this difficulty is the fact that the nature of some conditions, such as some disorders of mental function, impair the very functions upon which navigating a complex and arduous appeal process relies.
Committee member Lembi Buchanan identified key concerns about the process involved in pursuing recourse with the Tax Court of Canada:
- The vast majority of individuals who appeal to the Tax Court of Canada cannot afford to retain a lawyer or even an accountant to represent them.
- Many individuals are too intimidated to follow through with an appeal to the Tax Court of Canada if their notice of objection has been unsuccessful.
- The notice of appeal to the Tax Court of Canada must contain relevant facts and reasons for appeal. Unless the appeals officer has provided accurate details about the reasons why the DTC was rejected, this requirement may prove to be an impossible task for some individuals.
- The Tax Court of Canada system itself is not immune to problems, which may disadvantage a case before the judge, because unrepresented parties are not always familiar with the rules of evidence and court procedures.
- The Tax Court of Canada is not readily accessible to many individuals who live in northern and/or rural communities.
While judicial appeals ideally should be avoided, they do represent an essential secondary safeguard. In fact, the data indicate that it pays to appeal, since many decisions are either in error or a misrepresentation of the Income Tax Act.
Another major issue related to the appeal process was brought to our attention. There has been a notable increase in the number of rejections of individuals reapplying for the DTC after receiving it for more than 5, 10 and 20 plus years, even though their medical condition remained largely unchanged. The loss of financial assets and access to other programs and services is serious, especially if applicants lose their registered disability savings plan (RDSP). We discuss this concern related to the DTC gateway function in Section 5.
Many beneficiaries also experience psychological distress and are fearful of having to go through the DTC eligibility process, once again, in another five years. As a mental health advocate, Committee member Lembi Buchanan has helped many people in their DTC appeal process. For example, she recalls one applicant who had received the DTC for 15 years when asked by the CRA to reapply for the credit. This applicant was rejected and faced the daunting task of having to appeal a decision without being provided with a valid reason for the rejection.
While the decision was reversed upon appeal, the applicant was given to 2024 to reapply. At that time, they will be 71 years old. It is very unlikely their mental functions will be so improved that the applicant will no longer be markedly restricted. It seems inhumane to expect the applicant to face the rigorous process and costs of applying, and possibly having to file another objection to continue to benefit from the DTC.
Another example highlighted by Mrs. Buchanan is the case of a 28-year-old person with autism who received a letter from the CRA in June 2005 approving the DTC from 1990 to 2008. In August 2010, the CRA approved the DTC from 2009 to 2015. In October 2016, the CRA disallowed the DTC for the 2016tax year, despite substantiation of continued serious impairment in function and prior qualification. The individual filed an objection that was disallowed in July 2017. An appeal was filed with the Tax Court of Canada in October 2017. The judgment in March 2018 supported the DTC application and the CRA reinstated the benefit from 2016 to 2022.
In yet another example of positive intervention by the Tax Court of Canada, the CRA approved the DTC in July 2004 for an applicant with impairment in mental functions for the years 1990 to 2003 and future years. In January 2015, the CRA requested a "newly completed Form T2201." Two months later, the CRA disallowed the DTC. The applicant filed a notice of objection, which was disallowed in September 2015. An appeal was filed with the Tax Court of Canada in January 2016. By November 2016, the judgment supported application for the DTC and the notice of redetermination from the CRA allowed the DTC from 2015 and all future years.
Despite these positive outcomes, the current appeal process requires reform in order to make it less complex and intimidating. Perhaps most important, the process must be more transparent and fair. We recommend:
That the minister of national revenue review the current appeals process with a view to creating a straightforward, transparent and informed process where the applicant has access to all relevant information (including the precise reason their application was denied) and documents (including copies of all information submitted by health providers that pertain to their application).
We discussed the importance of sharing substantiating information with applicants earlier in this section. Transparency also involves the provision of clear information on how to file an appeal. That information is not readily available at the current time. Our committee recommends:
That the Canada Revenue Agency include a document (one-page, two-sided information sheet) entitled “Your Rights When a Notice of Determination Denies a Claim for the DTC” that would:
- explain the requirements, timelines and details for filing the following:
- review;
- notice of objection with the Appeals Branch; and
- notice of appeal with the Tax Court of Canada;
- inform taxpayers that other persons (that is, family members, friends or professional advisors) can act on their behalf by submitting Form T1013, Authorizing or Cancelling a Representative, or writing a letter;
- inform taxpayers that they have access to all documents in their files, including a copy of the follow-up questionnaire and any clarification letter completed by the health provider;
- inform taxpayers that they can contact the CRA for a copy of Pamphlet, P148, Resolving your dispute: Objection and appeal rights under the Income Tax Act, if they do not have access to the Internet; and
- provide the correct contact information and mailing addresses for the submission of any required materials.
Quality assurance framework
The CRA has informed our committee that it is always seeking to improve its disability products, including:
- form T2201, Disability Tax Credit Certificate;
- guide RC4064, Disability-Related Information;
- CRA web content;
- clarification letter sent to a health provider; and
- notice of determination sent to an applicant.
Even with improved products and administrative processes, we believe that a baseline set of procedural standards should be introduced to help assess and monitor progress on an ongoing basis. Clearer definitions of physical and mental functions will never eliminate entirely the concerns regarding unfair disability assessments. Unfortunately, errors in judgment and perceived inequity invariably will arise when eligibility involves a determination of functional incapacity.
In order to improve current DTC eligibility procedures, we propose that any assessment process should have in place several layers of checks and balances. First and foremost, it is essential to ensure that the CRA assessors who are assigned to review applications have adequate and consistent training, particularly around impairment in mental functions and episodic conditions. This assessment tends to be more complex than a determination of impairment in other functional areas, such as vision, hearing or mobility.
We are mindful of the fact that the Auditor General of Canada found in a review of Canada Pension Plan disability benefits great variability in the way in which similar eligibility applications were assessed [Office of the Auditor General of Canada, 2015]. He recommended a quality assurance framework to improve the effectiveness and consistency of decisions regarding eligibility. The purpose of such a framework would be to make sure that medical adjudicators followed a clear adjudication process, which would help with making appropriate and consistent decisions.
Moreover, the Auditor General pointed out that the responsible government department (Employment and Social Development Canada) did not appear to analyze the appeal decisions of the Canada Pension Plan Tribunal to determine why it had overturned the department’s decisions. He proposed that the adjudication framework be amended to reflect the rationale in those appeals [Office of the Auditor General of Canada, 2015: 6.58].
The Auditor General concluded that a quality assurance framework likely would have reduced the variability in eligibility decisions [Office of the Auditor General of Canada, 2015: 6.65].
Our committee believes that a quality assurance framework would help deal with inconsistency in DTC eligibility decision making brought to our attention by many health providers. The following comment is just one example:
"The DTC criteria are ambiguous and highly interpretable. Calls to CRA medical support staff for clarification result in conflicting advice/guidance across staff members that affects whether or not one would expect CRA approval of an application."
Quality assurance procedures can also include second-opinion screening. Cases that are considered to be particularly difficult to assess, especially those that involve impairment in mental functions or episodic conditions, could require a compulsory independent assessment screening. We made a recommendation to this effect earlier in this section.
A second, independent team would review any application for benefits or services that has been refused when required forms, duly completed by the appropriate health providers, would indicate otherwise. The opinions of relevant health providers, such as a psychiatrist or psychologist for cases of impairment in mental functions, could be sought for complex cases, as earlier proposed.
While some form of second-level screening would add to the cost of assessment, there may be considerable savings in the long run. Cases are often overturned at the appeal stage, which represents a costly quasi-judiciary process that, if avoided, would benefit all stakeholders.
Finally, a quality assurance framework would require the collection and analysis of program data, including the number of applications and the number of approvals and rejections by physical or mental function. Demographic information, including age, gender and location, would also be vital to collect. This information would provide the basis for ongoing monitoring and assessment of progress. We discuss this issue in Section 4 on CRA communications.
We were pleased to learn in December 2018 that the CRA will be setting up a team to monitor and improve the administration and delivery of the DTC. The CRA noted that this development stemmed from the insight our committee has provided into how the CRA can improve services to Canadians living with disabilities.
The Assessment, Benefit, and Service Branch of the CRA has created a dedicated service improvement team that will take into consideration the Committee’s feedback. The Branch will work to identify additional administrative improvements to products and tools, as well as find simple, efficient and innovative options and processes in order to improve services and communication to Canadians.
Our committee was pleased to learn that quality assurance studies and quality reviews are currently in place. The CRA has completed several studies that gather information on how successfully the CRA accurately processes DTC files and if it is meeting the established performance indicators and targets for the DTC process. The quality assurance review of DTC files is being monitored by areas of the CRA that are not involved in the initial determination process. The CRA also has a review procedure to catch any errors before the system processes a DTC claim and is usually completed on a daily basis. The quality review is completed by staff in the tax centres and monitored by Headquarters. Even though a quality assurance framework exists, there is a need to improve those processes.
But service improvement involves not only changes to actual procedures. It also requires effective communication about those procedures and relevant materials to Canadians and especially persons with disabilities. Fairness as well as the perception of fairness are critical to the success of any process with multiple stakeholders. We turn now to that important task.
Section 4 – Enabling access through improved communications
In the two previous sections of this report, our committee put forward a set of recommendations to improve access to the disability tax credit (DTC).
The first cluster of proposals focused on both clarifying and modifying the DTC eligibility criteria and their articulation in order to address the many problems embedded in the existing program. We proposed several recommendations that would make the DTC eligibility criteria clearer and would link them more closely to both empirical evidence and clinical practice.
The second group of recommendations dealt with the reform of CRA administrative procedures and practices involved in assessing and processing DTC eligibility.
This section addresses yet another key dimension of enabling eligibility for the DTC and other disability tax measures. It considers various ways in which the CRA can improve its communications with Canadians and with organizations representing persons with disabilities. These include:
- raising awareness;
- improving transparency;
- providing clear information;
- clarifying the criteria;
- improving client contact; and
- providing personal assistance.
Raising awareness
Our committee recognizes that over the past year, the CRA has initiated some improvements to how it communicates with Canadians. These are positive developments. At the same time, we believe that more needs to be done to raise awareness about the range of disability tax measures, better explain their purposes and provide information about applying for these benefits.
Unfortunately, there is no way around the fact that tax measures, in general, are not easy to understand. But disability tax measures are typically more complex than most tax measures because the former come with a number of unique conditions that must be met.
Complexity and lack of clarity are only part of the challenge. The equally important problem is that many Canadians have no knowledge of the tax provisions from which they potentially could benefit. La Confédération des organismes de personnes handicapées du Québec (COPHAN) noted in its submission that many persons with disabilities are not aware of all the tax measures to which they may be entitled.
March of Dimes Canada also pointed out to us that individuals currently eligible for the DTC and the registered disability savings plan are often unaware of the benefits available to them. It recommended that the CRA work directly with disability and advocacy organizations to share information and raise awareness about the DTC. It also proposed that front-line staff do further outreach to increase uptake of the DTC.
As an initial step, the CRA must ensure that its web-based materials on disability tax measures contain information that is both up-to-date and easy to grasp. It should review every document with a plain language screen so that all jargon and technical terms that act as barriers to understanding or completing an application are removed at the outset.
People First of Canada told us, for example, that only a small number of individuals are able to navigate the DTC application process. They are slowed down by confusing language and titles, unclear requirements and difficulty completing the form with their physicians. Moreover, "the forms and the process are overwhelming."
In its submission, People First of Canada put forward a set of actions to improve the accessibility of both the information on tax credits and eligibility procedures. Its proposals include:
- present the tax credits in plain accessible language so that the individuals can understand the process and the benefits;
- create a plain language version of Form T2201 that is easy to follow and understand;
- hold regular sessions for the individual caregivers to support learning and increase comfort levels in filling out these forms;
- make available additional assistance for filling out the application Form T2201.
- create more awareness of these tax credits so that they are available for individuals; and
- connect with physicians’ associations to educate them and get the word out on how to fill out these forms.
Our committee proposes that the CRA consult on an ongoing basis with relevant organizations representing persons with disabilities to test the general language and specific terms employed in CRA materials. This is an important way to check the information with consumers to see whether it is easily understood.
But accessibility has another meaning as well. The CRA must ensure that all its materials are made available in multiple formats so that these can be read by individuals with visual impairment. Our committee was pleased to learn that, since 2013, the Government of Canada updated its websites and web applications to ensure a high level of web accessibility, which are set out in Treasury Board of Canada Secretariat guidelines. These guidelines apply to all CRA web pages and applications.
In addition, the CRA offers services for persons with disabilities to ensure they are able to get information in different formats, such as with teletypewriters, operator-assisted relay services, and publications available in multiple formats.
The issue of accessibility is a larger question that relates to the ease of access to disability supports and their associated cost. It is one of the reasons why the DTC has become so significant to Canadians with disabilities. The DTC helps compensate, if only modestly, for some of the disability-related costs that are not reimbursed in any other way.
In short, it is essential that the CRA upgrade its technologies to reflect continually evolving technical aids. At the same time, it must continue to maintain earlier or older versions of its communications equipment. We recommend:
That the Canada Revenue Agency consult on a regular basis with selected community organizations to:
- ensure that all its communications and materials (including letters of correspondence with individuals) are easily accessible by persons with disabilities and are available in plain language. Organizations such as People First can assist with ensuring plain language; and
- determine whether its communications and materials are keeping pace with technological change and with the technologies in common use by communities of persons with disabilities.
The Committee heard other noteworthy proposals from organizations representing persons with disabilities. La Confédération des organismes de personnes handicapées (COPHAN) du Québec suggested, for example, that CRA web content follow Quebec’s lead in making links to related disability programs and supports in other provinces and in the territories.
The links would help Canadians with disabilities navigate more easily through the complex network of programs and services. The CRA section on Canada.ca that is focused on disability tax measures could act as a guide to a range of measures, in addition to its own tax benefits, available throughout the country. We recommend:
That Canada Revenue Agency web content, which outlines disability tax measures, link to relevant provincial and territorial websites that identify disability-related provisions in those jurisdictions, as well as the range of federal and provincial/territorial disability measures that require DTC eligibility in order to qualify.
Improving transparency
Our committee heard from a number of academics and experts working on disability tax measures and income security. They told us how difficult it is to get up-to-date statistical information on the DTC. In fact, we experienced the same problem in many of our discussions, because we lacked the demographic data on current DTC beneficiaries. Having a better understanding of the DTC population with respect to key factors, such as age and gender, will help guide our future discussions and policy proposals.
The CRA has begun to make key data on the DTC more publicly available. Its Disability at a Glance web content is an excellent start.
We look forward to receiving a more detailed breakdown of this information.
Our committee recommends:
That the Canada Revenue Agency provide and make publicly available relevant data on the DTC, including number of applications, approvals, rejections, and appeals; durations of eligibility by function; and a demographic profile of current beneficiaries by age and gender.
Providing clear information
But there is more to improved communications than simply telling Canadians about the tax measures for which they might potentially be eligible. Improved communications also involve providing more clear and relevant explanations about the benefits themselves and associated eligibility criteria.
Sometimes these conditions are difficult for the CRA to explain and/or are difficult for the general public, health providers and tax preparers to understand. We heard this consistently with respect to the DTC and the wording on the application Form T2201. We also learned that families are unclear about which and how many health providers are required to complete Form T2201.
One respondent to our health provider survey suggested that the CRA include information right at the outset about the income cut-off level below which an applicant would not derive any benefit from the DTC. Our committee, however, does not support this proposal.
"An inordinate amount of time is being utilized by NPs (nurse practitioners) and MDs (medical doctors) to complete forms for numerous reasons for patients. It would decrease unnecessary requests if it was clear on the T2201 the amount of annual income a person or their caregiver needs to earn in order for the tax credit to even apply. Forms are being completed when there is no benefit and this is a waste of provider and patient time."
Our hesitation arises from the fact that the DTC has expanded its role significantly since its inception. The DTC is now more than just a tax measure that helps offset additional disability-related costs. It also acts as a gateway to other essential disability benefits. An individual must first qualify for the DTC before gaining access to a wide range of disability-supports and services. We discuss this issue in Section 5.
The gateway function means that the level of income is no longer applicable to everyone. Even if individuals with disabilities fall below the taxpaying threshold, they can still benefit from DTC eligibility in order to gain access to other key disability measures, including the registered disability savings plan and child disability benefit. This expanded role for the DTC means that the income threshold of the applicant is basically irrelevant.
This raises another critical issue that must be better communicated. Most Canadians are not aware of the evolution of the DTC. The CRA needs to explain this additional function in its materials and communication. In fact, our committee raised questions as to whether the expanded role of the DTC needs to be formally acknowledged in the Income Tax Act.
Clarifying the criteria
Sections 2 and 3 of this report dealt at length with the fact that the DTC eligibility criteria are complex and open to interpretation by the CRA, persons with disabilities and health providers. It is difficult for most Canadians to know whether they would qualify or not. Even health providers told us that the rules are hard to understand, let alone respond to, on behalf of DTC applicants.
Our hope is that the many recommendations we proposed in the two previous sections on eligibility criteria and administrative procedures will address at least some of these concerns. But we flag this issue yet again, because it needs to be taken into consideration when the CRA is working on improved communications. While the CRA may improve its communications, even the clearest communication will fail if what is being communicated about (that is, eligibility criteria) remains complex and open to interpretation.
Organizations representing persons with disabilities and health providers told us repeatedly that the phrasing on the application Form T2201 is not well worded. The eligibility requirements are unclear and the terms employed are not consistent with clinical practice, notably when it comes to impairment in mental functions. A respondent to the health provider survey, for example, noted the following:
"As a psychologist completing these forms, I would prefer to know who and how I can support applications prior to completing them. As I become more clear about what a disability is and isn’t, I can provide the right kind of information. I sometimes even have difficulty knowing which parents to mention this tax credit to and which ones not to given the different criteria that seem to be applied."
We also heard that:
"Service Canada could have some brief video clips available on their site showing common scenarios of patients coping with disabilities who would qualify, and perhaps some showing more minor disabilities who would not qualify. Seeing is a powerful teacher to get the point across clearly."
Others felt, however, that the educational materials currently made available by the CRA need to improve. It was pointed out, for example, that "the ‘educational’ video clips that supposedly add clarification only muddy the waters."
As discussed in the two previous sections of this report, some respondents made specific recommendations regarding the clarity of the information provided by the CRA. It was suggested, for example, that the CRA do a better job of explaining certain terms, such as the 90% guideline. One respondent proposed the following:
"What constitutes 90% of the time or an inordinate amount of time... comparatives would help (twice as long or three times longer). Dressing: does it take the individual longer to dress due to a disease/disability only or is the limitation/restriction due to obesity or age-related mobility deficits? Does someone having to take a medication every day (e.g., thyroid disease) constitute a disability? There should be examples. Patients receive advice from companies that they can get approval for having any disease processed (e.g., thyroid, hypertension). The public needs more education as to who can apply."
Throughout the course of our work, we learned that it is not only applicants, organizations representing persons with disabilities, and health providers who have difficulty understanding the DTC eligibility criteria. Our committee also heard that tax preparers and promoters face similar challenges. One health provider suggested that:
"Tax preparers, accountants and bookkeepers, (i.e., anyone handing out this form in an official capacity) need to be better educated on the messaging they provide to patients about the form. This could be conveyed in bold print on the cover page of the form."
Improved information for this group is essential. Many respondents to the health provider survey reported that Canadians frequently are informed by tax preparers that "the doctor just needs to sign this, and I'll get the credit." We discussed this concern in Section 3.
We also heard from tax preparers and other organizations about allowing taxfilers to file online their application Form T2201 and associated materials. This process would make it easier for many individuals to apply for the DTC. Most government transactions are now being conducted through electronic submissions. We recommend:
That the Canada Revenue Agency provide an option for the electronic submission of Form T2201 and related materials that:
- is convenient and accessible for both taxpayers and tax preparers; and
- permits submission of those materials at the same time as, or after, the filing of an income tax and benefit return.
We expect to receive more informative feedback from tax preparers. We look forward to reviewing their responses and analyzing the results.
Finally, in our attempt to ensure improved communications with Canadians with disabilities, the Committee believes that the CRA should introduce a process to continually gather feedback from both current and former DTC beneficiaries.
We feel that it would be invaluable for the CRA to carry out a survey of clients similar to the health provider survey in order to give us yet another source of information. This process could be conducted on an annual basis with different clients, as part of the quality assurance framework that we proposed in Section 3. We recommend:
That the Canada Revenue Agency develop, in collaboration with the Disability Advisory Committee, a client experience survey that would align with the health provider survey, but be modified as appropriate to suit the needs and concerns of the target group comprising a representative sample of current and former DTC beneficiaries.
Improving client contact
More effective communications and clarity of CRA information and materials would go a long way toward enabling access to disability tax measures and to the DTC, more specifically. But while these are necessary steps, they are not sufficient.
It is essential for the CRA to provide in-person assistance, when required, in order to answer questions about both initial and continued eligibility. Such assistance would likely save considerable time, stress and resources down the road.
Several organizations and many health providers informed us that there is nowhere to turn for help. The CRA does offer a telephone assistance service but many organizations and health providers noted that the telephone lines are hard to reach. It can often take days to get through to a person who can assist with an enquiry. Several health providers told us, for example:
"Should you try to speak with someone at CRA to help you complete a form for a patient you cannot get through, the message states all agents are busy, call another time or go to the web site and hangs up."
"It is sometimes difficult to ‘make the case’ as explicitly as required given my busy practice and time restrictions. My assessment reports always contain more than enough detail to justify the need for DTC. I have received several requests for additional information from CRA, and have been unable to reach anyone at CRA by phone for assistance."
"I understand that the CRA may not want the public to be aware of their admission criteria re disability status due to the strong possibility of abuse and misuse of their program and funds. However, when a licensed professional such as a physician, psychologist, occupational therapist, is calling to enquire about such information, there ought to be a way to have a discussion with a person from the CRA to clarify whether or not there is merit to even sending an application form. I am only saying this, as I work in the private sector and my clients pay for my time re: completing the CRA form and the writing of a detailed report to accompany this form, and such a service is not covered by insurance providers (meaning that clients pay out of pocket). I do not want to waste their money nor my time with regards to an application process that is not fair, transparent and equitable."
"It is impossible to reach anyone by phone at the Revenue Canada Agency (RCA) office to discuss criteria and what specific information is necessary for them to consider with regards to their decision making process regarding accepting or refusing a client’s/family’s application for the tax disability credit (last year alone, I contacted four different RCA offices across Canada on numerous occasions between April and December to hear an automated voice tell me that "all lines are busy - please call back later")."
"The form usually needs significant writing to ensure condition is understood. There is no help or feedback when completing forms."
We heard similar concerns from individual Canadians in their submissions to our committee. For example:
"The phone number given indicates that there are no agents available to speak with."
"No results showed up when typing "disability" in the search tab of the website cra.gc.ca.forms."
"CRA representatives gave widely different information. Representatives couldn’t specify what information to submit or couldn’t refer the individual to anyone who could tell them what to submit."
"Call centres give conflicting information."
The Committee was pleased to learn that the CRA is already implementing changes as the result of our work. These changes include an enhanced telephone service to connect Canadians to call centre agents who can address complex DTC-related questions in one phone call.
The service will expand on a project that the CRA piloted to provide faster, more effective service to Canadians facing DTC-related issues. The preliminary results from the pilot were promising and updates were presented at our October meeting. The Committee was supportive of the project and would like to see it continue and expand eventually to include all call centres. We recommend:
That the Canada Revenue Agency provide dedicated support to ensure call centre agents are accessible and have the expertise to answer enquiries related to the DTC form and eligibility.
Our committee was also pleased to learn that the CRA does, indeed, plan to devote resources expressly for this purpose. The expertise component of the recommendation is particularly significant. We heard, as discussed, that many individuals, including health providers, received conflicting information from different CRA agents. Extensive and consistent training is essential to ensure consistency throughout the country.
Providing personal assistance
In addition to raising awareness about the DTC and other disability tax measures, our committee discussed the importance of enabling access to these measures. Once again, changes to the DTC eligibility criteria and improved administrative procedures will help reach this goal.
However, we recognize that many Canadians will still need assistance in learning about the tax measures for which they might be eligible. They may also need help completing the required income tax forms and any other associated materials, such as Form T2201. In a submission to our committee, a parent asked about "any guidance and advice on how I can ensure that my son’s needs are considered for the DTC."
We are especially concerned about the provision of information to, and assistance for, Indigenous Canadians. We know that many Indigenous Canadians do not pay income tax or even file an income tax and benefit return. Fortunately, the taxfiling rate has improved in recent years, because Canadians with children must complete an income tax and benefit return in order to qualify for the Canada child benefit.
Our interest is also linked to the fact that Indigenous Canadians face a disproportionately higher rate of disability than other Canadians. Ensuring that Indigenous Canadians have access to the range of disability benefits and supports for which they potentially are eligible should be a top priority for the federal government.
We also know that there are problems related to access to disability supports in northern and other remote regions of the country. An equally critical challenge involves access to health providers in those regions in order to complete the application Form T2201. Our committee is aware of the fact that Canadians living on low income, those with literacy challenges, newcomers to Canada, young people and seniors also face similar access issues.
We were pleased to learn that the CRA has a program in place to raise awareness among all Canadians about the tax benefits for which they may be eligible and to help them to complete the required forms. Not all Canadians are able to complete their own income tax and benefit return or are able to pay to have it done.
The CRA administers the Community Volunteer Income Tax Program (CVITP) through which community organizations host free clinics where volunteers help complete returns for eligible individuals. In Quebec, the program is called the Volunteer Program and is administered jointly by the CRA and Revenu Québec.
Through the CVITP, community organizations across Canada host free tax clinics where volunteers complete complete income tax and benefit returns for eligible individuals. The CRA provides support to the sponsoring organization through free promotional material, tax preparation software, web-based training for their volunteers, and access to a year-round dedicated help line and guidance from a CRA co-ordinator.
In the 2017 to 2018 fiscal year, more than 3,000 community organizations and 17,500 volunteers completed more than 785,000 income tax and benefit returns for over 700,000 people across Canada. The individuals assisted by the CVITP during 2016 to 2017 were entitled to receive refunds and benefits that totalled more than $1.5 billion.
Our committee would like to see continued support of this valuable program. We recommend:
That the Canada Revenue Agency, through the Community Volunteer Income Tax Program, which supports voluntary organizations to provide and train volunteers, run community tax clinics and raise awareness about the DTC. There should be a special focus on Indigenous communities.
The program may also be able to assist in the early screening of potentially eligible applicants. We heard from health providers that it would be helpful if some form of preliminary screening were in place in order to avoid inappropriate referrals and the associated time and resources that go into the application process. This would be one way to address the concern raised by many health providers who are uncomfortable with the gatekeeper role, earlier discussed, which they are currently expected to play.
Improved personal assistance would be invaluable to all Canadians, potential DTC applicants and their families, and to health providers. It is all the more important, given the expanded role the DTC now plays. It is this gateway function to which we now turn in Section 5.
Section 5 – Enhancing access to other disability benefits
The role of the disability tax credit has expanded over time
The DTC has evolved over the years since its introduction in the Income Tax Act as a tax deduction for Canadians who are blind. While the scope of the DTC has grown significantly, its original intent remains the same.
The primary purpose of the DTC is to reduce the income tax burden for Canadians with severe disabilities who are likely to incur additional costs not experienced by persons without disabilities. These extra expenses are often not readily itemizable, like the costs claimed for the medical expense tax credit or the disability supports deduction, discussed below.
Some disability-related expenses are considered indirect or non-itemizable because they are more difficult to quantify with precision. They include, for example, hiring a trained caregiver rather than a babysitter for a child with a disability. They may involve paying higher prices because of fewer shopping options, higher utility costs for heat or air conditioning, customized tailoring for clothing, or special transportation.
A related assumption is that, compared to other Canadians, workers with severe disabilities may take an inordinate amount of time to carry out a basic activity of daily living or may have to devote substantial time to a life-saving therapy. As a result, income-generating options for a person with a severe disability may be more limited than for someone without such a disability.
The DTC acknowledges these additional costs and/or extraordinary circumstances by reducing the income base on which an individual is required to pay income tax. But the DTC is now playing a larger role in the landscape of disability-related measures. It has become the gateway to establishing eligibility for a number of disability-related benefits and services (see Appendix 8).
Access to the DTC has been a long-standing concern. But access challenges have become all the more serious as many individuals apply not only, or even necessarily, for the financial assistance part of the DTC. The same eligibility criteria now act as the screen for wide-ranging programs and services.
As a result, the DTC has become the centrepiece of disability policy. We believe that the federal government must pay more attention to the implications of this profound shift, and explain the dual role of the DTC. In fact, we asked ourselves whether the Income Tax Act needs to be amended to reflect this broader role. There appears to be no legislative basis for this expanded DTC function. We recommend:
That the Canada Revenue Agencyrevisit and restate the purpose of the DTC in order to reflect its multiple roles.
The registered disability savings plan and the child disability benefit are two of the most significant provisions linked to DTC eligibility.
Access to a registered disability savings plan (RDSP)
The purpose of an RDSP is to help an individual and their family members and friends save for the long-term financial security of a person who is eligible for the DTC. RDSP account holders may also qualify for associated grants and bonds to bolster their long-term savings. The RDSP grant and bond have been especially helpful for persons with severe disabilities living on low or modest income. The federal contributions to their RDSP account enable their personal investment to grow significantly.
Under the Canada disability savings grant, the federal government can match every dollar contributed to an RDSP account with up to $3 for individuals with adjusted net family income less than $95,259 in 2019. Under the Canada disability savings bond, the federal government will deposit $1,000 each year into the RDSP account for a maximum 20 years if the adjusted net family income is below $31,120 (2019 figure). RDSP holders with an adjusted net family income between $31,120 and $47,630 in 2019 can still receive a partial bond.
The unique feature of an RDSP is that anyone can make a contribution on behalf of a given individual with a registered plan. Parents, grandparents, other family members and friends can use this savings vehicle to provide financial assistance to the RDSP beneficiary. Another positive feature of an RDSP is that it is exempt from most provincial disability and income assistance benefits. It does not get clawed back if the RDSP holder receives other benefits and it does not reduce disability benefit payments.
Contributions can be made to an RDSP until the end of the year in which the beneficiary turns 59, but they are not tax deductible. When contributions are withdrawn, they are not included as income to the beneficiary. However, the Canada disability savings grant, the Canada disability savings bond, investment income earned in the plan, and the proceeds from rollovers are included in the beneficiary’s income for tax purposes when they are withdrawn from the RDSP.
We heard from many Canadians who have not been able to open an RDSP because they don’t qualify for the DTC. They are being assessed for eligibility for a vital benefit (an RDSP) for which they may well qualify using a screen that had been designed for a different purpose (the DTC). Thousands of Canadians with disabilities are unable to take advantage of grants and bonds, delivered through an RDSP because of access problems related to the DTC.
Our committee believes that the DTC should not be the only access point to an RDSP. Individuals should be able to open an RDSP if they qualify for other disability-related programs intended for persons with severe disabilities. Long-term provincial/territorial social assistance programs are a logical place to start.
We recognize that broadening the RDSP avenues of eligibility could increase substantially the number of RDSP holders and applications for the RDSP grant and bond. We therefore want to ensure that both the grant and bond retain their value in the event of a larger caseload. The latter simply reflects the profound need for financial assistance among persons with severe disabilities.
Repayment of RDSP grants and bonds
Canadians and organizations representing persons with disabilities brought to our attention another important concern related to the DTC gateway function. When individuals apply for the DTC and they are accepted, a decision is made about the duration of eligibility. If the initial approval is for a designated period only, another application must be filed for the individual to continue qualifying for the credit.
A problem arises for beneficiaries who have already opened an RDSP account and are later declared no longer eligible for the DTC. All or part of the grants and the bonds that have been in the RDSP for fewer than 10 years must be repaid to the federal government. Finandicap and La Confédération des organismes de personnes handicapées du Québec (COPHAN) were among the organizations that noted their concern with this practice.
The loss of the DTC can be financially catastrophic to individuals who have opened an RDSP. Since 2010, 4,503 Canadians with disabilities have lost their RDSP and repaid $26,592,228 to the federal government. This clawback of grants and bonds is unacceptable, considering that these individuals were eligible for the DTC during a designated period.
We are particularly concerned about individuals with lifelong conditions that involve severe and prolonged impairment in physical and/or mental functions. If their functional capacity improves even slightly, say as a result of a new medication or technical aid, they may be deemed no longer eligible for the DTC. If their condition deteriorates, however, they may have difficulty re-establishing their DTC eligibility. It is not a certainty. In the meantime, they would have lost access to the only funds they have been able to save for their future needs. Many of these individuals live continually on the brink of poverty and are particularly vulnerable as a result of the punishing clawback rule.
In our view, any individual who received a federal benefit for which they were legitimately deemed eligible, in this case the RDSP grant and/or bond, should be able to keep those funds. Granted, they would no longer be eligible for any new or additional funds. But they should be permitted to retain the funds that they legitimately and legally received from the government during the time they were DTC-eligible.
A former DTC beneficiary who had to repay the RDSP grant and bond contributions likened the practice to asking a woman to repay the maternity benefits she received while pregnant. After the birth of her baby, she would be expected to return her maternity benefits to the federal government. Similarly, workers who received EI sickness benefits would have to repay those funds after they got well.
These hypothetical examples make no sense. We believe that the RDSP clawback is equally inappropriate and punitive. The practice makes it impossible for many individuals and families to do solid financial planning. They may have already moved to new housing or made other financial commitments on the basis of the funds they believed they were able to keep. Our committee recommends:
That the minister of national revenue work with the minister of families, children and social development to ensure that individuals are able to keep all contributions they made to, and any and all grants and/or bonds they may have received for, their registered disability savings plan for periods during which they qualified for the DTC.
While we focus here on the clawback, there are other challenges associated with the current structure and functioning of the RDSP savings vehicle. In gathering concerns related to DTC eligibility, we heard about many problems with the RDSP savings vehicle because of the links between the DTC and the RDSP programs. While these issues go beyond our mandate, we shared them with Employment and Social Development Canada, the department responsible for the RDSP program (see Appendix 11).
Access to the child disability benefit
The RDSP clawback is an illustration of a larger concern. It reflects the fact that individuals lose access to a range of benefits and programs if their DTC eligibility is denied or withdrawn after a certain time. We want to ensure that Canadians with disabilities still have access to all the other programs and measures linked to DTC eligibility. Access to other vital programs and services should not be revoked.
We cannot imagine the challenges that a family would face, for example, if it were to suddenly lose access to other vital measures, like the child disability benefit that provides crucial financial assistance for families with children with severe disabilities. For the period July 2018 to June 2019, a family may receive up to $2,771 ($230.91 per month) for each child who is eligible for the DTC. The benefit starts being reduced at family net income of more than $65,975. These households typically incur both direct and indirect costs related to severe disability, often up to thousands of dollars a year or much more.
The fact that the DTC acts as a gateway to this vital child disability benefit is troubling for two reasons. First, we earlier discussed how difficult it is for health providers to complete the DTC application Form T2201 on behalf of children. Thousands of households may not be receiving the financial assistance they desperately need through the child disability benefit because of the complexities related to DTC eligibility. We have proposed a number of improvements to this process.
Second, even if the DTC application Form T2201 were clearer, we wondered whether this route is still the best way to help families. We discussed whether the DTC eligibility screen is the most appropriate way to identify the families that may require financial assistance. There is a need to think through the provision of assistance for families with children with disabilities far more thoroughly than our committee mandate permits.
In the meantime, we want to ensure that families continue to receive the child disability benefit even if DTC eligibility is revoked. In fact, access to all gateway benefits and services should remain intact until a set of checks and balances is in place to determine whether the assistance or support provided through other programs should be cut off.
Our committee feels that we must continue to explore the range of concerns related to the DTC as a gateway to other vital disability benefits and services. There needs to be a better system in place to determine whether households no longer eligible for the DTC still require other important assistance, such as the child disability benefit, for which they had qualified.
While this work is under way, we believe that the federal government should introduce a moratorium on its practice of disqualifying individuals and families from other DTC-linked benefits. It should continue to allow access to these vital benefits and services until we have had an opportunity to explore other possible options for establishing eligibility. For example, there could be a secondary screening process for a vital measure, such as the child disability benefit, to determine whether a family should continue receiving that benefit even if their child is considered no longer DTC eligible. They should not be cut off right away with no further assessment or consideration. We recommend:
That, as a short-term measure, the federal government should ensure continued eligibility for related DTC-gateway programs, at least at the federal level, even if DTC eligibility has been revoked. This interim measure would allow for the development of secondary screening processes to determine whether individuals or households can continue to remain eligible for gateway-related services and supports.
Access to disability programs and benefits
This discussion raises serious questions about access to disability measures, more generally. We wondered whether the disability screening process should be removed from the CRA altogether and moved to a social agency, like Service Canada. That agency would determine access to a range of disability benefits and services, including the DTC.
But while this approach enables access to a range of programs and services, a single assessment process can also close the eligibility door. Individuals who are refused DTC eligibility find that they are cut off from other essential supports.
One solution is to identify a cluster of gateway programs, such as long-term social assistance and the Canada Pension Plan disability (CPPD) benefits in addition to the DTC. Several organizations representing persons with disabilities, including the Multiple Sceloris Society of Canada and the Regroupement des organismes de personnes handicapées de la région 03, made this proposal.
Our committee also discussed ways to streamline the DTC eligibility process. For example, we considered whether individuals who receive a CPPD benefit should automatically qualify for the DTC. Those who receive the DTC would not, however, be automatically eligible for a CPPD benefit.
The TAC had proposed in 2004 that the CRA undertake a study to determine the links between a CPPD benefit and the DTC. Our committee initially had intended to recommend a follow-up to this original study, given that it had been carried out more than 10 years ago.
However, we learned from its results that the two populations were quite distinct. The idea assumes that CPPD benefit and DTC populations are similar in terms of the presence of severe and prolonged disability. The difference is that the CPPD benefit program asks about the ability to work while the DTC program does not. We decided not to proceed with recommending a follow-up study.
Because of its important gateway role, we still feel that the CRA needs to consider possible ways to ease its eligibility process. At the very least, it should ensure better integration with Quebec, which administers a disability tax credit with its own eligibility criteria. We recommend:
That the Canada Revenue Agency, in collaboration with the Province of Quebec, determine a single eligibility process for the DTC in order to avoid separate eligibility at different levels of government.
In the longer term, we believe that the CRA should explore related program alliances that could lead to automatic DTC access. Possible alliances include veterans benefits and provincial/territorial long-term social assistance. Beneficiaries of these programs have already been through intensive disability-related screening.
We also wondered whether additional criteria, such as age, might be used for screening purposes. We will have a better idea about this issue when we receive the DTC demographic data currently being compiled by the CRA. Alternatively, we discussed whether a certain criterion (again, such as age) should result in removal from the DTC caseload and the provision of modest financial assistance through a new or existing program, such as a top-up to the guaranteed income supplement.
We considered whether certain diagnoses should enable automatic eligibility, as it does in the case of blindness. Paraplegia and dementia are possible examples. We recognize, however, the many challenges associated with a list-based approach.
Larger questions about the DTC
It is clear that the expanded role of the DTC requires a more fulsome discussion. There are no easy answers to the question about whether a gateway process is enabling or problematic. On the one hand, a gateway program, such as the DTC program, streamlines eligibility procedures because it removes the need for multiple applications. At the same time, refusal for the gateway program closes the door to a range of other benefits and services.
The gateway questions made us challenge even more fundamental assumptions about the DTC. Does its tax equity function still make sense? Are the objectives that the DTC seeks to achieve still valid? Does it remain a useful measure to offset disability costs? It is the latter question to which we now turn.
Section 6 – Recognizing the additional costs of disability
Most persons with severe disabilities face additional costs related both directly and indirectly to their disability. Direct costs refer to readily itemizable goods and services. They include, for example, technical aids and devices or home modifications to which a specific price tag can be attached. The medical expense tax credit and disability supports deduction help offset these costs.
Other disability-related expenses are considered indirect or non-itemizable because they are more difficult to quantify with precision. The DTC acknowledges these additional costs by reducing the income base on which a given individual is required to pay income tax.
Disability tax credit
Several DTC cost issues were brought to the attention of our committee:
- costs related to DTC procedures;
- costs related to Form T2201;
- extraordinary costs; and
- DTC refundability.
Costs related to DTC procedures
The submissions we received from many individuals and organizations representing persons with disabilities highlighted their concerns related to DTC procedures. Several noted that the complexities of the system forced many persons with disabilities to seek the assistance of tax promoters and others who charge a high fee for their services. Some promoters even take a percentage of the DTC claim, if the application is successful. We learned about contingency fees of up to 35% or more of the tax refund for assistance in completing Form T2201.
Our committee acknowledges the fact that many tax promoters put in substantial time and effort to assist DTC applicants. At the same time, we want to ensure that tax promoters are not charging inordinately high fees for their services, leaving DTC claimants with only a relatively small portion of their DTC claim, if they qualify.
We recommend:
That the Canada Revenue Agency cap the fee that consultants can charge to assist with an initial DTC application and act as expeditiously as possible to draft the regulations introducing this cap.
Our committee discussed whether the cap should take the form of a flat fee or a percentage of the amount for which a successful applicant was deemed eligible. We agreed that a modest flat fee of between $100 and $200 would be appropriate and could be applied consistently and fairly to all cases and throughout the country.
We recognized, however, that many cases are complex and may require more intervention, such as the receipt of a clarification letter or launch of a DTC appeal. In these instances, we agreed that it would be appropriate for tax promoters to charge a modest additional fee for their services.
We also heard concerns about unfair and inconsistent decisions regarding DTC eligibility. Many Canadians feel compelled to appeal their case and even take it as far as the Tax Court of Canada. For example:
"The system is too complicated or expensive for people to challenge its decisions."
"Canadians should be able to access the DTC without having to pay expensive legal bills for lawyers to represent them in court or excessive contingency fees to companies to act on their behalf."
We hope that the recommendations on reforming DTC eligibility criteria and procedures, as well as our proposed quality assurance framework, will reduce the need for applicants to challenge the determinations made in their case.
Costs related to Form T2201
Many health providers are not compensated adequately or at all by the health care system for the time they spend completing Form T2201 or a follow-up questionnaire for clarification when required. Some charge the applicant a fee to compensate for their time.
There appears to be no standard practice regarding billing for this form. Charges vary widely by health provider. The fee can be prohibitive, especially for individuals living on low income. The Canadian Mental Health Association told us:
"Because a health care professional must fill out the application form (T2201) and there is no limit to what the professional can charge, the DTC application is cost-prohibitive for individuals with disabilities, many of whom have limited income."
Connections is an Alberta-based organization that supports individuals with cognitive disabilities. It suggested that completion of Form T2201 be considered an insured health service so that the provincial government will cover the cost. Connections proposed a flat fee for completing the form, which the individual could also use if applying for long-term social assistance.
Our committee considered the option of the CRA paying or helping to offset the cost of completing Form T2201. But we acknowledged it is unlikely that the CRA would assume this cost. Such a practice would encourage virtually any individual with some form of functional impairment to apply for the DTC.
However, it seemed reasonable to ask the CRA to pay the cost incurred in providing additional information or clarification if Form T2201 has already been duly completed. There is policy precedent for this approach.
Service Canada, for example, reduces the cost of the medical report required when applying for a Canada Pension Plan disability benefit by paying up to $85 directly to the doctor or nurse practitioner. Any amount above $85 is the responsibility of the applicant. Veterans Affairs Canada (VAC) goes even further in its repayment practices.
Veterans Affairs Policy Document 1477 states that:
"When a medical examination and/or testing is requested by VAC, both the specific testing and/or the examination requirements in addition to the reporting expectations will be clearly articulated to the qualified medical practitioner or other qualified health professional providing the report. This is to prevent billing of unnecessary services."
"Pursuant to the provisions outlined in this policy, VAC will reimburse an applicant or provider at a reasonable rate in accordance with the provincially recommended fee for uninsured third-party requests for each completed VAC medical questionnaire form in support of a disability benefit application or reassessment."
In recognition of these policy precedents, we recommend:
That the Canada Revenue Agency reimburse an applicant or provider at a reasonable rate in accordance with the provincially recommended fee for the time involved in responding to CRA clarification letters in support of a DTC application or reassessment.
Extraordinary costs
It became clear in reviewing the submissions and responses to the health provider survey that many individuals and households face high disability-related costs. Families often struggle with very high expenses when they have children with severe disabilities.
We heard from a family that was unable to cover the extra cost of a pediatric therapist to assess and counsel their child. Another family wrote about their child who has autism and they needed financial aid to help pay the cost of therapy. Health providers indicated the following:
"Some children attend special schools because of their ADHD (attention deficit hyperactivity disorder) and or LD (learning disability) and these schools are expensive. The parents need the money from the DTC to help pay tuition, so that their child can get a good education, one that they were not able to receive through the public school system."
"There are families with significant struggles managing their children, having to stop working because of behavioural issues that their child shows in relation to a diagnosis, but they don't get the DTC. In contrast, I hear of people getting it for slight hearing loss."
"The current system makes no provision for families who cannot leave a young person with a developmental disability unattended despite intact basic language and cognitive skills. Families (and society) incur enormous costs/productivity losses under these circumstances."
It is one of the reasons why families and health providers raised concerns about the difficulties they experience when applying for the DTC on behalf of children. Even the modest DTC would help these households.
We recognize that the DTC was not designed as a measure to offset extraordinary costs. The financial challenges that families face when they have children with severe disabilities go beyond our tax-based mandate. However, we do want to bring this serious problem to the attention of the federal government.
DTC refundability
The fact that the DTC is non-refundable means that it is of little or no value to Canadians who are too poor to pay income tax, except for any benefits resulting from the DTC being a gateway to other programs. Yet these individuals and households still must face high costs if they have a severe disability. (These individuals may still be eligible for other disability-related programs and services as a result of the DTC gateway function, earlier described.)
To address this problem, there have been discussions over the years about converting the non-refundable DTC into a refundable credit. A non-refundable tax credit is subtracted from taxes owing and can only reduce taxes to zero. This represents a policy shift from a non-refundable tax credit that recognizes the impact of non-itemizable, disability-related expenses on an individual’s ability to pay income tax to a refundable credit providing a degree of income support.
A refundable tax credit, by contrast, not only reduces income taxes to 0, but also pays a benefit if the taxpayer deducts the value of the credit from taxes owing and has a negative balance. In other words, Canadians who are below the taxpaying threshold and have no other government debt would receive a refund from the federal government. A refundable DTC would provide some financial assistance to lower- and modest-income individuals with severe disabilities to help offset their disability-related costs.
The possibility of a refundable DTC was first raised in 2004 in Disability Tax Fairness, the report of the TAC on Tax Measures for Persons with Disabilities. A refundable DTC was proposed in submissions to us by several individuals and organizations, including the Multiple Sceloris Society of Canada and March of Dimes Canada.
A refundable DTC has also been put forward in reports by several academics and disability groups, including the Coalition for Disability Tax Credit Reform, the Council of Canadians with Disabilities, the Planned Lifetime Advocacy Network, the Canadian Association of the Deaf, the Canadian Hearing Society and the Canadian Paraplegic Association.
Our committee acknowledges that a refundable DTC would deliver only very modest assistance to Canadians with incomes below the taxpaying threshold. For the 2018 tax year, the maximum value of the DTC was $1,235.25. That is the maximum amount by which a DTC-eligible recipient would be able to reduce their income tax payable.
If, however, the DTC credit were made refundable, any Canadian who qualified for the DTC on the basis of severe and prolonged disability would be eligible to receive some benefit from the federal government, even if they owed very little or no income tax. While the amount they would receive would vary according to their level of net income, the highest possible benefit would be $1,235.25.
A refundable DTC would be of great assistance to low-income Canadians with severe and prolonged disabilities. By virtue of the fact that they have a disability that is severe and prolonged, they incur the same disability-related costs as higher-income households. A refundable DTC would help offset these costs.
But because the amount of a refundable DTC would be modest (a maximum $1,235.25 for the 2018 tax year), it would not provide anything near a basic level of income support for persons with disabilities, which has been identified as a major gap in Canada’s income security architecture. It could, however, serve as the foundation upon which a basic income for persons with disabilities would be built. This proposal was put forward in 2010 by the Caledon Institute and by several other academics, including University of Calgary professors, Stephanie Dunn and Jennifer Zwicker, who sent us a research paper on this issue.
Converting the DTC to a refundable credit would be an important first step, a foundation, in creating a basic income for Canadians with severe disabilities who face disproportionately high rates of poverty. Tax credits can go only so far in tackling poverty alleviation. Income security programs are required to address this objective. There is significant policy precedent for this action in Canada.
The federal government has played a key leadership role in alleviating poverty among seniors and children in this country. It has created and directly administers income security programs, notably the guaranteed income supplement and Canada child benefit, which provide financial assistance to low-income seniors and low-income households with children under the age of 18, respectively. (The federal government administers many other income security programs as well, but the two identified here are poverty-related measures, in particular.)
Our committee believes that it is now time for the federal government to turn its attention to tackling the serious problem of poverty among persons with disabilities. We recommend:
That the minister of national revenue work collaboratively with the minister of finance, the minister of families, children and social development, and the minister of sport and persons with disabilities to:
- identify ways of addressing the disproportionate poverty of Canadians with disabilities, or alternatively, that the minister of national revenue request the establishment of a parliamentary committee to address this issue and bring forward recommendations;
- transform, as a first step, the current DTC from a non-refundable credit into a refundable credit in order to recognize the non-itemizable costs incurred by lower-income Canadians with disabilities; and
- ensure that the poverty alleviation of Canadians with disabilities is a focus of all relevant federal-provincial/territorial ministers’ meetings and that there be no provincial/territorial clawback of any new or improved federal measures.
The importance of reliable data was raised in a conference call that our committee organized with selected experts in the country on the issue of DTC refundability. A list of questions (see Appendix 12) and a backgrounder on DTC refundability were prepared for the call.
Several participants noted that it is impossible to make good policy decisions in the absence of reliable data on actual and potential numbers of refundable DTC beneficiaries and the associated costs. We recommend:
That the Canada Revenue Agency, in partnership with the Department of Finance Canada, Statistics Canada and the disability community, undertake a study of the current data needs regarding the DTC and identification of appropriate new ways of tracking needed DTC information, including the estimated number of Canadians who potentially would be eligible for the DTC but are unable to benefit because of its non-refundable status.
Medical expenses tax credit
The medical expenses tax credit (METC) provides financial relief for the cost of designated heath- and disability-related items (see canada.ca/taxes-medical-expenses). The credit is available to all Canadians and not just persons with disabilities.
Several submissions highlighted concerns about the METC. Costs only above a certain threshold may be claimed. More specifically, only expenses in excess of the lesser of $2,302 for 2018 or 3% of net income can be claimed.
The Niagara Pain Support Group told us that many individuals with disabilities live on low income. They are unable to claim all their medical expenses because the basic threshold is too high. There is no provincial program that provides assistance for this ongoing problem.
Finally, the METC is a non-refundable tax credit. It is of limited value to low- and modest-income households, which pay little or no income tax. They do not benefit from a tax reduction.
Fortunately, a medical expense supplement was introduced by the federal government in order to address this very issue. It was one of the recommendations of the TAC on Tax Measures for Persons with Disabilities [Department of Finance Canada, 2004]. However, most Canadians are unaware of this tax provision. To be eligible for this supplement, the individual must have employment or self-employment income exceeding $3,566 in 2018. For 2018, the maximum supplement is the lesser of $1,222, or 25% of both medical expenses and disability supports expenses. This is reduced by 5% of combined net income (taxpayer and spouse) in excess of $27,044. It is eliminated when combined net income reaches $51,484.
Disability supports deduction
The disability supports deduction may be claimed by taxpayers who incur disability-related costs in order to earn employment or self-employment income or attend an educational institution. The disability supports deduction was announced in the federal Budget 2004 in response to a recommendation made by the TAC on Tax Measures for Persons with Disabilities. The introduction of the disability supports deduction represented a significant advance.
The disability supports deduction built upon and significantly modified the former attendant care deduction. In the past, the latter had allowed taxpayers who were eligible for the DTC and who required attendant care in order to go to school or work to deduct the costs of this care from their taxable income, thereby reducing their income tax payable.
The former attendant care deduction recognized only attendant care as a valid educational or employment expense and did not cover other disability-related costs. Claimants of the former deduction also had to pass the DTC screen. Taxpayers with disability-related costs other than attendant care relied on the medical expense tax credit.
There are several issues, however, which need to be addressed. Our first concern relates to the fact that few Canadians appear to be aware of this measure. It appears to have a low take-up rate. While the CRA was not able to provide requested data on the take-up of this measure, current tax expenditures tell an important story.
Since 2014, the disability supports deduction has cost the federal government an estimated $3 million a year. This is a small sum compared to the more than $1 billion price tag ($1,090 million in 2018) for the DTC. We recommend:
That the Canada Revenue Agency:
- raise awareness about the disability supports deduction, including special information sessions to inform disability organizations, post-secondary educational institutions and student networks, unions, employer organizations, training programs and the general public about the availability, purpose and provisions of this tax measure;
- in collaboration with the disability community, review on an annual basis the list of allowable items within the disability supports deduction to ensure it keeps pace with technological updates and changes; and
That the Canada Revenue Agency take steps to raise awareness among employers about any tax measures that provide incentives for hiring persons with disabilities and/or that help offset any of the costs of accommodation.
Our second concern relates to the current list of items allowed under the measures. The following items may be claimed for the disability supports deduction:
- attendant care expenses (special provisions apply);
- Bliss symbol boards;
- Braille note-taker devices;
- Braille printers, synthetic speech systems, large print-on-screen devices;
- deaf-blind intervening services;
- devices or software designed to allow a person who is blind or has a severe learning disability to read print;
- electronic speech synthesizers;
- job-coaching services;
- note-taking services;
- optical scanners;
- page turner devices;
- reading services;
- real-time captioning;
- sign language interpretation services;
- talking textbooks;
- teletypewriters;
- tutoring services; and
- voice recognition software.
While the current list is extensive, there is always a problem with lists because important items may be excluded. New technologies may take some time to be recognized. Items that might be added to the current list include the following:
- reclining work chairs (with prescription);
- bed-positioning devices for work (with prescription);
- mobile computer cart for sit/stand work at home (with prescription);
- alternative input devices (keyboards/mice);
- digital pens; and
- navigation devices for low vision.
Ideally, there would be no list. Persons with disabilities would be able to deduct any essential items they require for education and employment-related purposes. Prescriptions and receipts currently must be kept for most items as proof of need in case of audit. This check and balance in the existing system could be retained.
Our committee also looked at several technical aspects of the disability support deduction. We wondered whether individuals would be better off if the deduction were converted to a credit. This question requires further analysis. We recommend:
That the Canada Revenue Agency:
- amend the disability supports deduction to allow the deduction of any form of disability-related technical aid, equipment and service required for education, employment and participation in the community; and
- study and report on the implications of converting the current disability supports deduction from a deduction to a credit.
Finally, our committee raised questions about the disability supports deduction in comparison to the METC. The preferred option from a tax perspective was not clear to us.
We requested that the CRA analyze the tax impact of these two measures. While the comparison would be a theoretical analysis only, it would advance our understanding of the relative benefit of these two measures. This comparative data can provide a foundation for future recommendations.
Appendix 1 – List of Committee Members
The Committee members whose work produced this report are:
- Frank Vermaeten, Co-Chair of the Committee, Assistant Commissioner with the Canada Revenue Agency, from Ontario
- Dr. Karen R. Cohen, Co-Chair of the Committee, CEO, Canadian Psychological Association, from Ontario
- Sherri Torjman, Vice-Chair of the Committee, former vice-president, Caledon Institute of Social Policy, from Ontario
- Laurie Beachell, Baker Law, from Manitoba
- Gary Birch, Neil Squire Foundation, from British Columbia
- Dr. Jeff Blackmer, Canadian Medical Association, from Ontario
- Lembi Buchanan, Coalition for Disability Tax Credit Reform, from British Columbia
- Michael Edgson, RBC Financial, from British Columbia
- Roberta Heale, Nurses Practitioner Association of Canada, from Ontario
- Emily Johnson, Diabetes Canada, from Alberta
- Véronique Vézina, COPHAN, from Quebec
- Karen Wiwchar, H&R Block Canada, from Alberta
Appendix 2 – Recommendations
1
That in the determination of DTC eligibility, the Canada Revenue Agency ensure that the principle of parity guides its actions with respect to physical and mental functions including, but not limited to, the removal of multiple screens of eligibility for persons with impairment in mental functions.
2
That the Canada Revenue Agency amend the list of mental functions on Form T2201 as follows:
- attention;
- concentration;
- memory;
- judgment;
- perception of reality;
- problem solving;
- goal setting;
- regulation of behaviour and emotions
- (for example, mood disturbance or
- behavioural disorder);
- verbal and non-verbal comprehension; and
- learning.
3
That the Canada Revenue Agency replace on page 5 of Form T2201 the term “effects of the impairment” with the following:
“The effects of the individual’s impairment must restrict their activity (that is, walking, seeing, dressing, feeding, mental functions, eliminating, hearing, speaking or some combination thereof) all or substantially all of the time, even with therapy and the use of appropriate devices and medication.”
4
That the Canada Revenue Agency delete the reference to “social activities” on page 5 of Form T2201 due to the contradiction on page 3 of the form. Page 5 states that one is ineligible on the basis of social and recreational activity, while page 3 states that the inability to initiate and respond to social interactions makes one eligible, as does the inability to engage in common simple transactions.
5
That the Canada Revenue Agency change the question on page 5 of Form T2201 about the likelihood of improvement to ask health providers whether the individual’s illness or condition that is responsible for the impairment in function, such as walking or cognitive functions, is likely to improve, as in the following example:
“In thinking about the individual’s impairment, please consider whether the condition that causes the impairment (for example, blindness, paraplegia, schizophrenia or bipolar disorder) can be expected to last for a continuous period of at least 12 months.”
6
That the Canada Revenue Agency no longer interpret all or substantially all as 90% of the time and no longer interpret an inordinate amount of time as three times the amount of time it takes a person without the impairment.
7
That in the DTC assessment process, the Canada Revenue Agency employ the following definition to determine marked restriction in mental functions:
“The individual is considered markedly restricted in mental functions if, even with appropriate therapy, medication and devices (for example, memory and adaptive aids):
- all or substantially all the time, one of the following mental functions is impaired, meaning that there is an absence of a particular function or that the function takes an inordinate amount of time:
- attention;
- concentration;
- memory;
- judgment;
- perception of reality;
- problem solving;
- goal setting;
- regulation of behaviour and emotions (for example, mood disturbance or behavioural disorder);
- verbal and non-verbal comprehension; or
- learning; OR
- they have an impairment in two or more of the functions listed above none of which would be considered a marked restriction all or substantially all the time individually but which, when taken together, create a marked restriction in mental functions all or substantially all the time; OR
- they have one or more impairments in mental functions which are:
- intermittent; AND/OR
- unpredictable; AND
- when present, constitute a marked restriction all or substantially all the time.”
8
That the Canada Revenue Agency remove specific references to activities in the T2201 section on mental functions and include examples of activities in the current Guide RC4064 to help health providers detail all the effects of the markedly restricted mental function(s), as in the following illustration:
“The individual is considered markedly restricted in mental functions if they have an impairment in one or more of the functions all or substantially all of the time or takes an inordinate amount of time to perform the functions, even with appropriate therapy, medication, and devices. The effects of the marked restriction in mental function(s) can include, but are not limited to, the following (this list is illustrative and not exhaustive):
- with impaired memory function, the individual cannot remember basic information or instructions such as address and phone number or recall material of importance and interest;
- with impaired perception, the individual cannot accurately interpret or react to their environment;
- with impaired learning or problem solving, the individual cannot follow directions to get from one place to another or cannot manage basic transactions like making change or getting money from a bank;
- with impaired comprehension, the individual cannot understand or follow simple requests;
- with impaired concentration, the individual cannot accomplish a range of activities necessary to living independently like paying bills or preparing meals;
- with impaired ability to regulate mood (for example, depression, anxiety) or behaviour, the individual cannot avoid the risk of harm to self and others or cannot initiate and respond to basic social interactions necessary to carrying out basic activities of everyday life; or
- with impaired judgment, the individual cannot live independently without support or supervision from others or take medication as prescribed.”
9
That the Canada Revenue Agency consider a child and an adult version of Form T2201, with eligibility criteria tailored as necessary.
10
That the Canada Revenue Agency revise the list of functions on Form T2201 to the following:
- vision;
- speaking;
- hearing;
- lower-extremity function (for example, walking);
- upper-extremity function (for example, arm and hand movement);
- eliminating;
- eating/feeding; and
- mental functions.
11
That the Canada Revenue Agency, in respect of the parity principle, create a list of examples of activities for each impaired function for inclusion in the current Guide RC4064 to help health providers detail all the effects of markedly restricted function(s), as in the following proposed guidelines (this list is illustrative and not exhaustive):
- with impaired lower-extremity function, the individual cannot walk;
- with impaired upper-extremity function, the individual cannot feed or dress themselves, or cannot attend to basic personal hygiene; or
- with impaired eating/feeding, the individual cannot swallow or eat food.
12
That the Canada Revenue Agency review the current eligibility criteria for hearing, which are out of date.
13
That the Canada Revenue Agency work in collaboration with the Department of Finance Canada to consult with relevant health providers and stakeholders before introducing any legislative changes to the Income Tax Act with respect to the definition of mental or physical functions.
14
That the Canada Revenue Agency replace the current eligibility criteria for life-sustaining therapies as set out in Form T2201 with the following:
Individuals who require life-sustaining therapies (LSTs) are eligible for the DTC because of the time required to administer these therapies. These are therapies that are lifelong and continuous, requiring close medical supervision. Without them, the individual could not survive or would face serious life-threatening challenges. Close medical supervision is defined as monitoring or visits, at least several times annually, with a health provider. These therapies include but are not necessarily limited to: intensive insulin therapy for type 1 diabetes; chest therapy for cystic fibrosis; renal dialysis for chronic and permanent renal failure; and medically prescribed formulas and foods for phenylketonuria (PKU).
15
That the Canada Revenue Agency:
- consider whether some conditions, such as a complete paraplegia or tetraplegia, schizophrenia or a permanent cognitive disorder with a MOCA below 16, should automatically qualify for the DTC in the way that blindness does. (MOCA is a mental status examination of cognitive functions used commonly to assess impairment that results from conditions such as dementia, head injury or stroke.); and
- examine the eligibility criteria employed in other federal and provincial/ territorial programs, such as the Ontario Disability Support Program and the programs for Canada Pension Plan disability benefits and, veterans disability pensions, to identify the conditions/diagnoses that establish automatic eligibility for those programs.
16
That the Canada Revenue Agency examine the new eligibility form being used for Canada Pension Plan disability benefits to identify areas in which there might be synergies regarding eligibility for the DTC, such as including the presenting condition or diagnosis as supplementary information to identifying functional limitations.
17
That the Canada Revenue Agency test or pilot various approaches that would remove the gatekeeper role from health providers. One such approach would be for community tax clinics to take on a screening or advisory function. Another would be to establish a Canada Revenue Agency call centre explicitly for this function.
18
That the client experience survey on the DTC and other disability tax measures to be carried out by the Canada Revenue Agency include a question as to whether the individual or recipient had any difficulty accessing a health provider for the purposes of completing Form T2201 and, if so, for which activity. Clients should also be invited to provide any additional comments on this question. Special attention should be paid in this survey to the needs and concerns of Indigenous Canadians.
19
That the Canada Revenue Agency develop a process for expanding the list of health providers with the appropriate expertise who can assess eligibility for the DTC.
20
That in the case of determining DTC eligibility for persons with impairment in mental functions, the Canada Revenue Agency include relevant specialized health providers, including, but not limited to, psychiatrists and psychologists, in the review process when applications are disallowed.
21
That the Canada Revenue Agency:
- copy to the applicant all clarification letters sent to the health provider;
- let the health provider know that all communication to a health provider about an applicant will be copied to the applicant and that any communication the health provider submits to Canada Revenue Agency will also be made available to the applicant;
- encourage the health provider to contact and consult the applicant as necessary when providing any clarification to the Canada Revenue Agency; and
- extend the time for a health provider to file a clarification letter with the Canada Revenue Agency from 45 to 60 days and note this timeline on the first page of the questionnaire.
22
That the Canada Revenue Agency:
- provide in notice of determination letters a relevant reason as to why a DTC application was denied;
- include in notice of determination letters a copy of the clarification letter and the
- health provider’s clarification response. This information is vital in case of an appeal; and
- move the consumer survey request to the bottom of the notice of determination letters.
23
That the Minister of National Revenue review the current appeals process with a view to creating a straightforward, transparent and informed process where the applicant has access to all relevant information (including the precise reason their application was denied) and documents (including copies of all information submitted by health providers that pertain to their application).
24
That the Canada Revenue Agency include a document (one-page, two-sided information sheet) entitled “Your Rights When a Notice of Determination Denies a Claim for the DTC” that would:
- explain the requirements, timelines and details for filing the following:
- review;
- notice of objection with the Appeals Branch; and
- notice of appeal with the Tax Court of Canada;
- inform taxpayers that other persons (that is, family members, friends or professional advisors) can act on their behalf by submitting Form T1013, Authorizing or Cancelling a Representative, or writing a letter;
- inform taxpayers that they have access to all documents in their files, including a copy of the follow-up questionnaire and any clarification letter completed by the health provider;
- inform taxpayers that they can contact the Canada Revenue Agency for a copy of Pamphlet, P148, Resolving your dispute: Objection and appeal rights under the Income Tax Act, if they do not have access to the Internet; and
- provide the correct contact information and mailing addresses for the submission of any required materials.
25
That the Canada Revenue Agency consult on a regular basis with selected community organizations to:
- ensure that all its communications and materials (including letters of correspondence with individuals) are easily accessible by persons with disabilities and are available in plain language. Organizations such as People First can assist with ensuring plain language; and
- determine whether its communications and materials are keeping pace with technological change and with the technologies in common use by communities of persons with disabilities.
26
That Canada Revenue Agency web content, which outlines disability tax measures, link to relevant provincial and territorial websites that identify disability-related provisions in those jurisdictions, as well as the range of federal and provincial/territorial disability measures that require DTC eligibility in order to qualify.
27
That the Canada Revenue Agency provide and make publicly available relevant data on the DTC, including number of applications, approvals, rejections, and appeals; durations of eligibility by function; and a demographic profile of current beneficiaries by age and gender.
28
That the Canada Revenue Agency provide an option for the electronic submission of Form T2201 and related materials that:
- is convenient and accessible for both taxpayers and tax preparers; and
- permits submission of those materials at the same time as, or after, the filing of an income tax and benefit return.
29
That the Canada Revenue Agency develop, in collaboration with the Disability Advisory Committee, a client experience survey that would align with the health provider survey, but be modified as appropriate to suit the needs and concerns of the target group comprising a representative sample of current and former DTC beneficiaries.
30
That the Canada Revenue Agency provide dedicated support to ensure call centre agents are accessible and have the expertise to answer enquiries related to the DTC form and eligibility.
31
That the Canada Revenue Agency, through the Community Volunteer Income Tax Program, which supports voluntary organizations to provide and train volunteers, run community tax clinics and raise awareness about the DTC. There should be a special focus on Indigenous communities.
32
That the Canada Revenue Agency revisit and restate the purpose of the DTC in order to reflect its multiple roles.
33
That the Minister of National Revenue work with the Minister of Families, Children and Social Development to ensure that individuals are able to keep all contributions they made to, and any and all grants and/or bonds they may have received for, their registered disability savings plan for periods during which they qualified for the DTC.
34
That, as a short-term measure, the federal government should ensure continued eligibility for related DTC-gateway programs, at least at the federal level, even if DTC eligibility has been revoked. This interim measure would allow for the development of secondary screening processes to determine whether individuals or households can continue to remain eligible for gateway-related services and supports.
35
That the Canada Revenue Agency, in collaboration with the Province of Quebec, determine a single eligibility process for the DTC in order to avoid separate eligibility at different levels of government.
36
That the Canada Revenue Agency cap the fee that consultants can charge to assist with an initial DTC application and act as expeditiously as possible to draft the regulations introducing this cap.
37
That the Canada Revenue Agency reimburse an applicant or provider at a reasonable rate in accordance with the provincially recommended fee for the time involved in responding to Canada Revenue Agency clarification letters in support of a DTC application or reassessment.
38
That the Minister of National Revenue work collaboratively with the Minister of Finance, Minister of Families, Children and Social Development, and the Minister of Sport and Persons with Disabilities to:
- identify ways of addressing the disproportionate poverty of Canadians with disabilities, or alternatively, that the Minister of National Revenue request the establishment of a parliamentary committee to address this issue and bring forward recommendations;
- transform, as a first step, the current DTC from a non-refundable credit into a refundable credit in order to recognize the non-itemizable costs incurred by lower-income Canadians with disabilities; and
- ensure that the poverty alleviation of Canadians with disabilities is a focus of all relevant federal-provincial/territorial ministers’ meetings and that there be no provincial/territorial clawback of any new or improved federal measures.
39
That the Canada Revenue Agency, in partnership with the Department of Finance Canada, Statistics Canada and the disability community, undertake a study of the current data needs regarding the DTC and identification of appropriate new ways of tracking needed DTC information, including the estimated number of Canadians who potentially would be eligible for the DTC but are unable to benefit because of its non-refundable status.
40
That the Canada Revenue Agency:
- raise awareness about the disability supports deduction, including special information sessions to inform disability organizations, post-secondary educational institutions and student networks, unions, employer organizations, training programs and the general public about the availability, purpose and provisions of this tax measure; and
- in collaboration with the disability community, review on an annual basis the list of allowable items within the disability supports deduction to ensure it keeps pace with technological updates and changes.
41
That the Canada Revenue Agency take steps to raise awareness among employers about any tax measures that provide incentives for hiring persons with disabilities and/or that help offset any of the costs of accommodation.
42
That the Canada Revenue Agency:
- amend the disability supports deduction to allow the deduction of any form of disability-related technical aid, equipment and service required for education, employment and participation in the community; and
- study and report on the implications of converting the current disability supports deduction from a deduction to a credit.
Appendix 3 – Disability Advisory Committee Terms of Reference
1. Mission statement
- To advise the Canada Revenue Agency (CRA) on interpreting and administering tax measures for Canadians living with disabilities in a fair, transparent and accessible way.
2. Mandate of the Committee
- To provide advice to the Minister of National Revenue and the Commissioner of the CRA on the administration and interpretation of laws and programs for disability-related tax measures administered by the CRA;
- To provide advice on how the needs and expectations of the disability community can be considered by the CRA as they interpret and administer disability-related tax measures. This may involve recommendations for information gathering and collaboration between the CRA and the disability community;
- To provide advice on how the CRA can increase:
- overall awareness of tax measures for persons with disabilities; and
- take-up of tax measures for persons with disabilities.
- To provide advice on how the CRA can best:
- engage persons with disabilities and their support communities; and
- deliver information, education and outreach initiatives about disability-related tax measures and important administrative changes to:
- persons with disabilities;
- those who support persons with disabilities;
- professionals who advise persons with disabilities;
- health practitioners; and
- not-for-profit agencies and various levels of government;
- To review and make recommendations for improvement to the CRA's administrative practices in order to enhance the quality of the services and products the CRA provides to persons with disabilities;
- To provide the CRA with a formalized means of consulting with various stakeholders; and
- While legislative change is beyond the mandate of the Disability Advisory Committee and the role of the CRA, recommendations for legislative change to disability tax measures may be made by the Committee for consideration and will be forwarded to the Department of Finance Canada.
3. Composition
Membership on the Committee will be determined on the following basis:
- The Committee consists of a blend of service providers (e.g. health, tax professionals, lawyers, accountants), advocates of the disability community and persons with disabilities;
- The Committee will be composed of 12 members and 2 co-chairs, appointed for a term not to exceed forty-eight (48) months (starting with the first meeting of their appointment);
- One of the Committee members will act as vice-chair, to support the private sector co-chair and provide activities at the discretion of co-chairs such as;
- help setting the agenda for the in-person meetings; and
- participate in discussions with co-chairs as to the progress of the Committee and the work that needs to be undertaken.
- The Minister and the Commissioner appoint the members and determine the length of their terms;
- In order to have some continuity of membership, during the first four years of the Committee, the members will be given different terms:
- four (4) members will be appointed for forty-eight (48) months;
- four (4) members will be appointed for thirty-six (36) months; and
- four (4) members will be appointed for twenty-four (24) months.
- Thereafter, members will be appointed for terms of thirty-six (36) months;
- Should a member not be able to serve his or her full term of appointment, the Minister jointly with the Commissioner will then appoint a suitable individual to complete the remaining portion of the term of appointment created by that vacancy;
- Membership is voluntary and members will not be paid to attend meetings. However, reasonable travel and accommodation expenses to attend meetings will be reimbursed according to the CRA Travel Policy, and meetings will be held in accordance with section 9 (below); and
- Other federal departmental representatives (e.g Sport and Persons with Disabilities, Finance, Employment and Social Development) may be welcomed in the role of observers or resource people.
4. Role of Committee members
- The roles and responsibilities of Committee members include:
- awareness of the needs and experiences of persons with disabilities to inform the Committee's deliberations and recommendations to the CRA on its disability-related tax measures;
- identifying topics for consideration or presentation to the CRA;
- offering advice, comments and recommendations on CRA services, products, and administrative policies and other issues and initiatives that are presented to the Committee;
- undertaking activities to inform its advice and recommendations to the CRA such as mechanisms for stakeholder engagement and collaboration (e.g. surveys, focus groups);
- committee members have been selected to represent the views of their respective communities and associations. The members agree not to use the Committee as a means to advance their own personal interests or further the sole interests of the associations they represent;
- committee members agree not to act as advocates to address the tax situations of specific taxpayers or to raise cases with the Committee that are before the courts; and
- committee members are expected to participate in a collaborative and constructive manner that promotes tangible outcomes and upholds public confidence in the Committee’s mandate, advice, and recommendations. Members are asked to address any individual concerns through dialogue with the co-chairs and, as appropriate, the Committee as a whole.
- Committee members are not spokespersons for the CRA. Each member is a stakeholder, representing themselves as an expert or as an advocate of persons with disabilities;
- Any information developed in consultation with other groups or shared by Committee members will become part of the formal and public proceedings of the Committee upon consensus of the Committee; and
- Members may discuss consultative initiatives of the Committee with their communities and colleagues unless expressly advised that they should not do so for reasons of confidentiality.
5. Establishment of co-chairs
- The Assistant Commissioner, Assessment & Benefit Services Branch (ABSB) of the CRA, will serve as co-chair of the Committee alongside a co-chair from the private sector;
- The private sector co-chair must be a Committee member;
- The term of a private sector co-chair will be twenty-four months (starting with the first meeting of his/her appointment);
- After the initial appointment of a private sector co-chair by the Minister and the Commissioner for twenty-four (24) months, the private sector co-chair can be renewed by the Minister and the Commissioner for a subsequent term of twenty-four months, or a new private sector co-chair can be appointed by the Minister and the Commissioner;
- Members of the Committee can be eligible for appointment as co-chair after serving a term of twenty-four (24) months or more;
- Should the private sector co-chair not be able to serve his or her full term of appointment, an appointment will take place according to 5.b), c) d) and e); and
- The outgoing co-chair will have the opportunity to remain a member of the Committee for an additional 12 months to ensure continuity between the co-chairs. This could mean that the Committee will be composed of 13 members on some occasions.
6. Roles of co-chairs
- Ensure that the Committee adheres to its mandate and the members fulfill their roles;
- Develop meeting agendas in concert with the Committee's mandate and roles;
- Facilitate meetings and lead the discussions, including during video or teleconferences;
- Ensure that all members are heard, engaged and respected in the work of the Committee;
- Report on the progress made by the Committee to the Minister and the Commissioner; and
- Serve as spokespersons for the Committee.
7. Responsibilities of the co-chair from the CRA
- To be the liaison between CRA and the Committee; and
- To provide secretariat services to the Committee which includes, but is not limited to providing the Committee with data necessary to informing their work and any recommendations such as:
- how the CRA currently liaises with disability stakeholder groups;
- how the CRA handles inquiries regarding disability;
- processes the CRA uses to decide on DTC eligibility;
- requirements of persons to maintain their DTC eligibility;
- rates of acceptance and rejection by activity; and
- appeal processes and data.
8. Responsibilities of the co-chair from the Committee
- To be the liaison between the 12 members of the Committee and the CRA in its secretariat function;
- To represent the views of the Committee as a whole; and
- To guide the Committee in its advisory function.
9. Meetings
- Upon initial formation, the Committee will meet three times per year. The frequency of meetings will be periodically re-examined to ensure best use of Committee members' time;
- The meetings will be held in Ottawa at location(s) that are accessible to those participants who are persons with disabilities. Other methods of meeting may also be utilized in order to keep costs at a reasonable level, such as videoconferences, teleconferences or on-line consultation in lieu of face-to-face meetings, in accordance with section 3.g); and
- In order for a meeting to take place, a quorum is necessary and will be met when a minimum of 7 members are in attendance.
10. Topics of discussion
- The co-chairs are responsible for setting meeting agendas in consultation with Committee members. Any member of the Committee can submit relevant topics for discussion to the co-chairs;
- An agenda item presented for discussion or activity that is not aligned with the mandate and role of the Committee and/or that does not meet with the consensus of the Committee will not be pursued;
- In the event of dissent arising about whether an agenda topic or activity is aligned with the mandate and role of the Committee, the co-chairs and/or the Minister and the Commissioner will have the authority to rectify the dissent;
- The Minister or the Commissioner may request the Committee discuss and analyze a specific topic; and
- The Committee can request information as defined in 7.b necessary to informing a topic of discussion.
11. Reporting
- A record of meeting proceedings will be kept and submitted to the Minister and Commissioner as well as made publicly available;
- The Committee may report on a specific topic to the Minister and the Commissioner in the format of a letter sent to the Minister and the Commissioner indicating the summary of the findings and the recommendations of the Committee;
- In the event that the Minister or Commissioner requests the Committee to discuss and analyze a specific topic, the Committee will report on this discussion and analysis will be sent to the Minister and the Commissioner in the format of a letter indicating the summary of the findings and any attendant recommendations;
- At the end of each year (following three meetings per year), the Committee will report to the Minister and the Commissioner with a summary of all topics discussed as well as recommendations for all topics; and
- Meeting proceedings (a), specific reports (b) and annual reports (c) will be reviewed and approved upon consensus of Committee members.
The CRA will assist the Committee in ensuring that all meeting materials and Committee reports are fully accessible.
12. Secretariat
- The Committee co-chair is the Assistant Commissioner of the ABSB or as an alternate, the Director General of Benefit Programs Directorate; and
- The Assessment, Benefit, and Service Branch will provide secretariat services for the Committee, performing functions such as:
- maintaining membership lists and coordinates of each member;
- circulating agendas, minutes and documentation to Committee members;
- organizing materials and all logistics for Committee meetings; and
- supporting the co-Chairs in their roles and responsibilities communicating with the Commissioner, the Minister and other stakeholders.
Appendix 4 – List of Organizations We Heard From
- Arthritis Society
- Cadesky Tax
- Canadian Chiropractic Association
- Canadian Medical Association
- Nurse Practitioner Association of Canada
- Canadian Association of Optometrists
- Speech-Language & Audiology Canada
- Canadian Academy of Audiology
- Canadian Association of Occupational Therapists
- Canadian Physiotherapy Association
- Canadian Psychological Association
- PLAN Institute
- Registered Disability Savings Plan Action Group
- University of Calgary
- Canadian Mental health Association
- Canadian Veterans Advocacy
- Centre intégré du réseau en neuro-développement de l’enfant
- Chronic Pain Association of Canada
- Niagara Chronic Pain Support Group
- Confédération des organismes de personnes handicapées du Québec
- Connections Counselling
- Council of Canadians with Disabilities
- Diabetes Canada
- Disability Tax Fairness Alliance
- Finandicap
- Manitoba League of Persons with Disabilities
- March of Dimes Canada
- Multiple Sclerosis Society of Canada
- National ME/FM Action Network
- Ostomy Canada Society and Nurses Specialized in Wound, Ostomy and Continence Canada
- Parkinson Canada
- People First of Canada
- Regroupement des associations de personnes handicapées de l’Outaouais
- Regroupement des organismes de personnes
Appendix 5 – Health Providers Survey
Appendix 6 – Financial Advisors and Tax Preparers Survey
Appendix 7 – Description of Federal Measures for Persons With Disabilities
Disability tax credit
The disability tax credit (DTC) is a non-refundable tax credit that helps individuals with disabilities or their supporting individuals reduce the amount of income tax they may have to pay. To be eligible for the DTC, an individual must have a severe and prolonged impairment in physical or mental functions, as defined in the Income Tax Act, and has to be certified by one of the following medical practitioners:
- medical doctor;
- nurse practitioner;
- optometrist;
- audiologist;
- occupational therapist;
- physiotherapist;
- psychologist; or
- speech-language pathologist.
Eligibility is not based on a diagnosis, but rather on the effects of the impairment on the ability to perform the basic activities of daily living.
Once the individual with a disability is eligible for the DTC, they may claim the disability amount of $8,235.If the individual qualifies for the disability amount and was under 18 years of age at the end of the year, they may claim an additional supplement of up to $4,804.
A supporting individual or the spouse or common-law partner of the eligible individual with a disability may be able to claim all or part of an unused disability tax credit.
Tax measures for persons with disabilities
Canada caregiver credit
The Canada caregiver credit (CCC) helps caregivers with the expenses involved with taking care of their spouse or common-law partner or dependant who has an impairment in physical or mental functions.
The CCC is based on two amounts. A higher maximum amount of $6,986 (in 2018) may be claimed by a caregiver in respect of each infirm dependant who is an eligible relative. This amount will be reduced dollar-for-dollar by the amount of the dependant’s net income above $16,405 (in 2018). A lower maximum amount of $2,182 for infirm dependants will remain as part of the following amounts:
- the maximum spousal or common-law partner amount;
- the maximum amount for an eligible dependant; and
- the amount for infirm children under age 18 at the end of the tax year.
In cases where an individual claims an amount for an infirm spouse or common-law partner or an amount for an eligible dependant who is infirm, the individual must claim the CCC at the lower amount (maximum $2,182 for 2018). Where this results in less tax relief than would be available if the CCC higher amount (maximum $6,986 for 2018) were claimed instead, a top-up will be provided to offset this difference.
Home accessibility expenses
An individual may be able to claim home accessibility expenses as a non-refundable tax credit if they own a home in Canada and paid for eligible renovations to improve the safety or accessibility of the home.
An individual may be eligible for this credit if, at any time in the year, they meet one of the following criteria:
- are 65 years of age or older; or
- are eligible for the DTC.
They may claim up to $10,000 per year in eligible expenses. They may also claim this credit on their income tax and benefit return for a dependant, if certain criteria are met.
The renovations must be for the main residence of the individual who is 65 years of age or older or eligible for the DTC. Also, the renovations must be permanently part of the home and meet one of the following criteria:
- allow the individual to gain access to the home or be mobile or functional within the home; or
- reduce the risk of harm within the home or in accessing the home.
Home buyers’ amount
An individual may claim the home buyers’ amount of $5,000 if they meet both of the following criteria:
- they or their spouse or common-law partner bought a qualifying home; and
- they did not live in another home owned by them or their spouse or common-law partner in the year the home was bought or in any of the four preceding years (first-time home buyer).
However, they do not have to be a first-time home buyer if they meet one of the following criteria:
- are eligible for the DTC; or
- bought the home for the benefit of a related individual who is eligible for the DTC.
The purchase must be to allow the individual with the disability to live in a home that is more accessible or better suited to their needs.
Working income tax benefit
The working income tax benefit (WITB) is a refundable tax credit intended to provide tax relief for eligible working low-income individuals and families who are already in the workforce and to encourage other Canadians to enter the workforce.
The WITB consists of a basic amount and a disability supplement.
For single individuals without children, the maximum amount of WITB is paid if working income is between $7,236 and $12,016 for 2018. The WITB payment is gradually reduced when net income is more than $12,016 (this is referred to as the base threshold). No WITB is paid when net income exceeds $19,076. These amounts vary slightly for residents of Alberta, Quebec, Nunavut and British Columbia.
For families, the maximum amount of WITB is paid if the family's working income is between $10,688 and $16,593 for 2018. The WITB payment is gradually reduced when family net income is more than $16,593 (this is referred to as the base threshold). The WITB payment is reduced to zero once family net income exceeds $29,407. These amounts vary slightly for residents of Alberta, Quebec, Nunavut and British Columbia.
An individual may be able to claim a WITB disability supplement, of up to $529, if they meet both of the following criteria:
- are eligible for the DTC; and
- had working income in the year.
They may claim the WITB on their income tax and benefit return. However, eligible individuals and families may be able to apply for advance payments for the following tax year.
For the 2019 tax year, the WITB will be replaced by the Canada workers benefit.
Measures for children with disabilities
Child care expenses deduction
The child care expenses deduction is to provide some relief for taxpayers who incur child care expenses in order to work, carry on a business or undertake certain educational activities. An individual or their spouse or common-law partner may have paid someone to look after their child who, at some time in 2018, was under 16 years of age or had an impairment in physical or mental functions. For a child who is eligible for the DTC, the annual child care expense amount may be up to $11,000.
Child disability benefit
The child disability benefit (CDB) is a tax-free additional monthly benefit included with the Canada child benefit made to families who care for a child under age 18 with a severe and prolonged impairment in physical or mental functions. To get the CDB:
- an individual must be eligible for the Canada child benefit; and
- their child must be eligible for the disability tax credit.
For the period of July 2018 to June 2019, an individual could get up to an additional amount of $2,771 ($230.91 per month) for each child who is eligible for the disability tax credit.
The CDB is also paid with the children’s special allowances to the agency.
Savings and pension plans related to the DTC
Registered disability savings plan
A registered disability savings plan (RDSP) is a savings plan that is intended to help parents and others save for the long-term financial security of an individual who is eligible for the DTC.
Contributions to an RDSP are not tax deductible and can be made until the end of the year in which the beneficiary turns 59. Contributions that are withdrawn are not included as income to the beneficiary when they are paid out of an RDSP. However, the Canada disability savings grant (grant), the Canada disability savings bond (bond), investment income earned in the plan, and the proceeds from rollovers are included in the beneficiary's income for tax purposes when they are paid out of the RDSP.
The grant is an amount that the Government of Canada pays into an RDSP. The Government will pay a matching grant of 300%, 200%, or 100%, depending on the beneficiary's adjusted family net income and the amount contributed. Up to $3,500 in matching grants can be paid into an RDSP in one year, and up to $70,000 over the beneficiary's lifetime. A beneficiary's RDSP can receive a grant on contributions made until December 31 of the year in which the beneficiary turns 49.
The bond is an amount paid by the Government of Canada directly into an RDSP. The Government will pay a bond of up to $1,000 a year into the RDSPs of low-income Canadians with disabilities. No contributions have to be made to get the bond. The lifetime bond limit is $20,000. A bond can be paid into an RDSP if an application is made on or before the end of the year in which the beneficiary turns 49.
Amounts paid from a registered retirement savings plan or a registered retirement income fund upon the death of an annuitant
If an individual was a financially dependent child or grandchild of the deceased annuitant or member who depended on a annuitant or member because of an impairment in physical or mental functions, they may contribute to their registered retirement income fund (RRIF) any amounts they receive or are considered to have received from a deceased annuitant's or member's:
- registered retirement savings plan (RRSP);
- pooled registered pension plan (PRPP); or
- specified pension plan (SPP).
An individual can roll over the proceeds of a deceased annuitant's or member's RRIF, RRSP, RPP, SPP or PRPP to the registered disability savings plan of a financially dependent child or grandchild who has an impairment in physical or mental functions.
Medical expenses
Medical expense tax credit
The medical expense tax credit is a non-refundable tax credit for individuals who have sustained significant medical expenses for themselves or certain of their dependants. These expenses include a wide range of products, procedures, and services, such as:
- medical supplies;
- dental care; and
- travel expenses.
An individual may claim the total of the eligible expenses minus the lesser of the following amounts:
- $2,302; or
- 3% of the individual’s or dependant’s net income for the year (in respect for whom the credit is claimed).
Certain medical expenses that have to be certified by a medical practitioner. Medical practitioners include a wide range of individuals in the medical profession, such as doctors, pharmacists, and nurses.
Refundable medical expense supplement
The refundable medical expense supplement is a refundable tax credit available to working individuals with low incomes and high medical expenses. An individual may be able to claim this credit if all of the following conditions apply:
- they made a claim for medical expenses or for the disability supports deduction;
- they were resident in Canada throughout 2018; and
- they were 18 years of age or older at the end of 2018.
They must also meet the criteria related to income.
Disability supports deduction
The disability supports deduction provides tax relief for individual taxpayers who have paid for certain medical expenses to enable them to do one of the following:
- perform the duties of an office or employment;
- carry on a business, either alone or as a partner actively engaged in the business;
- attend a designated educational institution or a secondary school at which the taxpayer is enrolled in an educational program; or
- carry on research or any similar work for which the taxpayer received a grant.
Only the individual with the disability can claim this deduction.
There is a list of the specific types of expenditures that will qualify for the disability supports deduction. In many cases, a medical practitioner must prescribe the particular device, equipment or service, or must certify that the individual requires the device, equipment or service because of their impairment.
Students with disabilities
Certain education-related benefits that require an individual to be a full-time student, such as the scholarship exemption, may be claimed by a part-time student if they meet one of the following criteria. The student:
- is eligible for the disability tax credit (DTC) for the year; or
- has an impairment in physical or mental functions, and a medical practitioner has certified in a letter that the impairment would not reasonably allow the student to be enrolled full-time.
Appendix 8 – Disability Measures Linked to DTC Eligibility
- Disability tax credit (federal and provincial, except Quebec. Quebec will accept a copy of Form T2201 for their "amount for a severe and prolonged impairment in mental or physical functions," instead of Form TP-752.0.14-V, Certificate Respecting an Impairment)
- DTC child supplement (federal and provincial, except Quebec, see note above)
- Child disability benefit
- Home accessibility credit
- Home Buyers’ Plan
- Registered disability savings plan
- Qualified disability trust
Adult with a severe and prolonged disability
- Disability tax credit (federal and provincial, except Quebec, see note above)
- Home accessibility credit
- Disability-related employment benefits
- Registered disability savings plan
- Home Buyers’ Plan
- Qualified disability trust
Other items that are impacted by DTC eligibility:
- Medical expenses tax credit
- Child care expenses deduction
- Tuition, education and textbook amount
- Home buyers’ amount
Appendix 9 – Form T2201
Appendix 10 – DTC Data for Mental Functions
| Year | Total number of new applications | Total number of rejections |
|---|---|---|
| 2016 – 2017 |
117,020 | 21,795 |
| 2015 – 2016 |
115,043 | 14,199 |
| 2014 – 2015 |
113,844 | 13,389* |
| 2013 – 2014 |
116,190 | 13,389* |
| 2012 – 2013 |
104,766 | 14,385 |
| 2011 – 2012 |
103,795 | 12,768 |
*Although identical, these numbers are correct.
Appendix 11 – RDSP Concerns
The registered disability savings plan (RDSP) rules and administration have become impossibly complex and very difficult for most people to understand.
There are problems regarding initial eligibility because of difficulties qualifying for the disability tax credit (DTC). Some Committee submissions have suggested that other programs, such as long-term provincial/territorial social assistance, act as a gateway to an RDSP as well. But one key informant was concerned that opening the eligibility door too widely will invariably raise the costs of the RDSP program and might result in a substantial reduction of Government of Canada contributions to the program’s grant and bond components. Those components are vital and should be protected.
One individual proposed that the eligibility assessment process be removed from the Canada Revenue Agency and placed instead with Employment and Social Development Canada, Service Canada or a new federal-government body responsible for disabilities.
Eligibility for an RDSP is particularly difficult for persons with intellectual impairment or development disability. They often must subject themselves to guardianship before they can open an RDSP. This requirement has implications for other aspects of their lives.
In 2012, the Government changed the RDSP rules to allow parents, spouses and common-law partners to open up an account on behalf of people deemed not contractually competent. But many people don’t have that designated person in their lives. Moreover, each jurisdiction appears to treat these clients differently.
There is a need for a national solution or pan-Canadian supported decision-making approach to banking. There likely are similar concerns regarding people with dementia and other related conditions. Who oversees the appropriate use of funds on behalf of the individual?
Ottawa claimed several years ago that it does not have the jurisdiction to act on a supported decision-making approach to banking. However, the Government does have jurisdiction over banking and it did change the RDSP law in 2012, thereby representing an important policy precedent. Moreover, the RDSP provisions are written into the Income Tax Act, so there is a policy lever to introduce changes in this area.
Eligibility problems are essential to resolve because new cohorts are aging out of the plan every year. Age 49 is the last year that the Government can contribute a $10,000 retroactive Canada disability savings grant and a 10-year retroactive Canada disability savings bond to individual RDSPs. Each year, individuals who turn age 49 are missing out on these retroactive payments that are worth $20,000 per person.
If an RDSP has been opened by parents and the parents die, the status of the RDSP is unclear. There is uncertainty as to what the banks are doing with these accounts if they deem that the beneficiary is not contractually competent to manage the plan. Are they requiring a legally authorized attorney to act on the person’s behalf? This requirement may have associated costs and may present financial barriers for the account holder. The current status of these accounts and their associated assets appear to be unknown territory.
People who lose eligibility for the DTC should be allowed to maintain their RDSP. Moreover, they should not be required to pay back Government contributions made on their behalf during the time that they were DTC-eligible. This is a tremendous burden to place on RDSP beneficiaries. Because individuals who qualify for the RDSP grant and bond have low to modest incomes, most are not in a position to easily repay these funds if they were counting on them in their financial decision making.
There are concerns with respect to current beneficiaries accessing funds. The problem is the result of the 10-year rule for withholding funds combined with the fact that an annuity-like formula for lifetime disability payments is applied. The formula is calculated as a fixed market value divided by life expectancy (83) minus age. The problem is that most beneficiaries will not live long enough to access the funds in their RDSP. It takes at least 25 years to get the maximum funds out of an RDSP.
The Government could consider an approach in which beneficiaries are permitted to withdraw a certain amount in stages. Right now, there are limits with respect to how much plan holders can withdraw and when they can withdraw. A Senate committee has recommended a reduction of the withholding time to five years. But this change alone will not fully resolve the problem. The formula for lifetime disability payments must also be reviewed.
It should be noted that beneficiaries can access their funds prior to the 10-year withholding period if they pay a penalty. There were some changes in 2012 but some exemptions are still needed.
The RDSP savings vehicle is being seen and treated increasingly as a retirement fund. The 10-year withholding rule reinforces that mindset. While tax-deferred growth is important, retirement was not the original intent of this policy measure. It was intended as a way to get more money into people’s pockets and to improve the quality of their lives.
Poverty is a serious problem among persons with disabilities and a suite of measures is required to adequately address it. The RDSP measure was seen as one way to harness private contributions, along with matched Government dollars, so that people with disabilities could live a better life. The RDSP savings vehicle was designed more as an anti-poverty measure and should be viewed in that light, especially when any changes to its grant and bond portions are considered. The registered-retirement-savings-plan type of design of the RDSP savings vehicle has embedded barriers and complexities and altered its basic purpose.
Appendix 12 – Questions for DTC Refundability Conference Call
1. What are the strengths and potential pitfalls of making the DTC refundable with respect to:
- eligibility criteria;
- increased demand;
- adequacy of benefit;
- links to provincial/territorial social assistance;
- clawback of other benefits;
- RDSP eligibility; and
- other factors?
2. What discussions are under way in the country regarding poverty reduction and persons with disabilities? Would a refundable and/or a refundable/enhanced DTC act as an effective base upon which to build a larger income benefit?
3. What are the advantages of designing a broader disability income benefit in this way? What are the possible pitfalls (if different from the above)? Should the DTC be removed from the income tax system altogether and converted into an entirely new benefit or monthly allowance? Reports by the Caledon Institute and by Quebec researchers have put forward this proposal.
4. Should seniors be eligible for a refundable DTC or should this group be assisted through some other measure?
5. What is strategically possible within the current federal-provincial/territorial environment? Is a refundable DTC seen as something achievable in the short term?