
2022 Third Annual Report of the Disability Advisory Committee
Table of Contents
- Recommendations at a Glance
- Part 1: Achievements to Date
- Part 2: DTC Eligibility
- Part 3: Ongoing Committee Work
- Part 4: Indigenous Issues
- Part 5: DTC Data
- Part 6: Registered Disability Savings Plans
- Appendices
- Appendix A: Terms of Reference
- Appendix B: Committee Members
- Appendix C: Committee Recommendations
- Appendix D: Federal Measures for Persons with Disabilities
- Appendix E: Disability Measures Linked to DTC Eligibility
- Appendix F: DTC Application Form T2201
- Appendix G: Resources on Language and Disability
- Appendix H: Selected Legal Issues
- Appendix I: Canada Disability Benefit
- Appendix J: Factsheet – Indigenous Peoples
- Appendix K: Updated Tables for the DTC Statistical Publication
Recommendations at a Glance
Third Annual Report of the Disability Advisory Committee
The Disability Advisory Committee (DAC) provides advice to the Minister and the Canada Revenue Agency (CRA) on improving the administration and interpretation of tax measures for Canadians living with disabilities.
Our third report summarizes our work, the progress of previous recommendations, and provides the following 10 new recommendations:
Disability Tax Credit (DTC) Eligibility
1. The CRA and the Department of Finance Canada should change the term ‘impairment’ to ‘limitation’ in all DTC-related administrative and legislative documents.
2. Decisions to expand the pool of health providers, one provider group at a time, who can complete the DTC application form (T2201) take time and expertise that neither CRA nor the Department of Finance Canada possess.
3. Any licensed health provider, whose license is in good standing, be permitted to complete the DTC application (Form T2201).
4. The CRA should replace the current eligibility criteria for life-sustaining therapies as set out in the DTC application (Form T2201) with a designated list of identified therapies.
DTC Review and appeals
5. CRA to share DTC appeals data with the Committee to better understand which demographic groups are experiencing challenges.
6. The CRA should better communicate to DTC applicants who launch an objection or appeal, that they will remain eligible for all DTC-related benefits and credits until the appeal is resolved.
DTC Legal issues
7. The Department of Finance Canada should amend the Income Tax Act (ITA) and/or the CRA amend its policy, to allow a person with a mental disability to appoint a representative to manage their tax affairs without resorting to legal guardianship.
8. Over the long-term, the federal government should apply the Peace, Order and Good Government clause to encourage the creation of a national minimum-standard legislative framework for supported decision-making laws.
9. The CRA encourage the Department of Finance Canada to exempt DTC beneficiaries from the capital gains on the sale of a home entrusted to them.
10. The federal government broaden the list of persons defined as “qualified family member” in the ITA to include siblings to act as RDSP plan holders for persons with mental disabilities.
Part 1: Achievements to Date
Context
In 2017, Minister of National Revenue Diane Lebouthillier announced the creation of the Disability Advisory Committee to provide advice on tax measures for persons with disabilities. Since our first meeting as a group in 2018, we have covered a wide range of issues. Our mandate and current membership can be found in Appendices A and B, respectively.
In our two previous reports, we made a combined total 50 recommendations for improving disability tax measures in Canada. This third annual report adds another 10 recommendations to the list. Appendix C includes the full list of earlier and new recommendations.
Disability tax credit
While there are several tax measures intended specifically for persons with disabilities (Appendix D), the Committee focused our work this past year primarily upon the disability tax credit, commonly known as the DTC.
The DTC plays a significant role in the disability landscape. While the credit itself is not an income program, it has a major impact on income security in two ways:
- it reduces the amount of income taxes that persons with severe and prolonged disabilities must pay
- it acts as an entry point or gateway to other disability-related benefits and programs (Appendix E)
Individuals may apply for this credit for one or both of these purposes. For some applicants, the DTC acts only to reduce the amount of income taxes they owe. These individuals may not be eligible for or require any of the other programs linked to this credit.
Other applicants, by contrast, do not have sufficient taxable income and they owe little or no income tax. However, they apply for the DTC in order to establish eligibility for the related programs.
Finally, some Canadians may apply for the DTC for both purposes: to reduce their income taxes and to gain access to other benefits.
Needless to say, the dual role of the DTC adds a layer of complexity that is unique to this tax measure. It is difficult to explain this double purpose, which affects both income taxes and income levels of recipients.
This dual role seems to have evolved for a good reason. Prior to 2008, the disability tax credit acted only to reduce income taxes. When the Registered Disability Savings Plan (RDSP) was introduced in 2008, the Department of Finance Canada made the decision to use the DTC as the eligibility criterion for opening an RDSP account.
The decision made sense at the time. The rationale was to reduce the application burden by requiring persons with disabilities to go through a single eligibility process. There appeared to be a need for a single-entry point to the suite of federally-delivered programs and benefits. Using the DTC as a gateway to the RDSP helped reduce red tape as well as the time and costs involved in applying for the new program.
Over the years, the so-called gateway role of the DTC evolved to include access to a number of other disability-related programs. While there are many advantages to this approach, there are also clear disadvantages. If an applicant is refused at the single-entry point, there is nowhere to turn – other than to a review or appeals process.
The alternative is to have applicants qualify over and over again for every program for which they potentially are eligible. That process represents a heavy administrative burden, the costs of which would be better applied to the programs themselves. It is always best to minimize, to the extent possible, the administrative burden by simplifying various eligibility procedures.
But herein lies another challenge. The application process for the DTC is anything but simple and it involves a significant administrative apparatus. DTC applicants must complete the Disability Tax Credit Certificate (Form T2201) and a designated health provider must attest to the type and extent of disability related to the DTC claim.
The complexities involved in the DTC application process have given rise over the years to multiple committees and reports about the problems embedded in this process and the need for reform. Our Committee studied these various reports. In 2018, we carried out a pan-Canadian survey of health providers qualified to complete the T2201 to which we received more than 1,100 responses. Through our DAC portal, we heard from disability organizations and individual Canadians who described their lived experience.
Based on this evidence and our discussions, the Committee made DTC-specific recommendations in our two previous annual reports that pertained to three distinct areas:
- eligibility criteria
- administrative procedures for approving or denying claims
- communication and outreach for conveying information about this tax measure
We are pleased to present brief highlights of several legislative, administrative and communication reforms that have been introduced as a result of our work. At the same time, we acknowledge that significant challenges remain, which are discussed in the next sections of this report.
Key achievements
i. Legislative changes
Our first two annual reports described at length our many concerns about the DTC eligibility criteria. We identified multiple problems related to the list of functions as set out on the application Form T2201.
We were particularly concerned about the definition of mental functions. For one thing, some of the defined impairments in mental functions had to all be present in order to qualify under mental functions. We noted that this conjunctive requirement did not apply to any of the physical functions. It effectively meant that a higher eligibility bar was being applied to the mental functions category. Moreover, the list of mental functions was an odd combination of functions and activities of daily living.
The conjunctive requirement, an incomplete list of eligible mental functions and the inclusion of adaptive activities, which depend on but are not mental functions, combine to create great difficulty for health providers in completing the Form T2201. The eligibility criteria for mental functions have little clinical relevance.
Many health providers who responded to our survey about the T2201 noted that an application for impairment in mental functions typically generated a clarification letter, which the Canada Revenue Agency (CRA) sent to the health provider to request additional information. Health providers told us that they often had no new information and would send back the same responses originally provided.
To tackle these challenges, our Committee spent time identifying the many problems in the current eligibility criteria regarding impairment in mental functions. We also drafted a proposed new definition of mental functions for inclusion in the Income Tax Act. The Committee was pleased that the 2021 federal Budget announced a significant change in the definition of mental functions which, for the most part, was based on our recommendations.
While there are some differences from what we had proposed, we believe that the new list better reflects the components that comprise the mental functions category. The revised criteria will be more relevant to the health providers who complete the Form T2201. The conjunctive requirement that previously applied to mental functions was removed. The new definition of mental functions is discussed in the next section.
The 2021 federal Budget also announced a change in the definition of life-sustaining therapy (LST). It reduces the number of times that a therapy had to be administered from three times a week to twice a week in order to qualify for the DTC. It also allows for the time that secondary caregivers spend in administering life-sustaining therapy. The Committee supports these changes in that they ease the previous eligibility criteria related to LST.
At the same time, we believe it is time for a significant modernization of the definition of life-sustaining therapy. In our view, the eligibility criteria as currently defined are largely unverifiable by health providers.
ii. Administrative improvements
The CRA is bound in its actions by terms and definitions set out in the Income Tax Act, while the Department of Finance Canada is responsible for changes to this legislation. However, the CRA is in a position to introduce administrative reforms that can ease eligibility for various tax measures. We were pleased that the CRA has made several procedural changes that we believe will enable access to the DTC.
One of the most noteworthy actions was the creation of an electronic application Form T2201, a reform that the Committee had proposed. We had noted in our earlier annual reports that an electronic application is consistent with government practice to allow online submission of all kinds of information, applications and payments. It also aligns with the fact that the regular income tax process can now be done completely online.
Perhaps more importantly, the DTC electronic application allows for the provision of a substantial amount of information to both applicants and health providers. Multiple drop-down menus in various places can provide a more detailed explanation of the specific requirements on the Form T2201. The electronic application can include examples of impairment in function, which the Committee has provided, to help health providers interpret the various eligibility provisions.
Yet another advantage to the electronic application is that it enables the tabulation of additional data on the DTC. With a new list of mental functions, for example, it will be easier to collect more detailed information in that area.
Right now, there is no disaggregation of this information. All the applications related to impairment in mental functions are lumped together into one category. It is impossible to know the relative distribution of applicants in the various categories, such as impairment in function related to memory compared to impairment in function linked to emotional regulation. By contrast, there is a detailed breakdown of the categories related to impairment in physical function. We discuss this issue in the section on DTC Data.
Our Committee had also recommended that more assistance be provided to applicants right from the start to ease the complex eligibility process. The CRA introduced a designated call centre with staff trained specifically to respond to DTC-related questions.
In response to another Committee recommendation, the CRA created the new position of Navigator to help applicants with particularly complex cases. There is now a Navigator in each of the three major tax branches throughout the country. Navigators receive referrals from the DTC call centre and assist the referred individuals to work their way through the DTC application process.
All three improvements – the electronic application Form T2201, DTC call centre and Navigator positions – have only recently been introduced. But already, the CRA is reporting a reduction in the number of clarification letters and their associated delays and costs in DTC applications. This is just one barometer of an improved eligibility process. The impact of these new measures must continue to be monitored and assessed over time.
iii. Communication and outreach
Our two previous annual reports had called for improved communications with respect to the DTC and other disability tax measures. We note that the CRA continues to extend its outreach activities and is producing materials in plain language. It is also introducing materials and assistance in various formats to ensure their accessibility to applicants with visual and/or hearing impairments. Our own annual reports were produced as full documents and as one-page organigrams.
However, we recognize that there is still much work to do in terms of ensuring that the CRA web pages and its materials are accessible. We believe that the CRA should carry out regular accessibility audits of its web pages and public materials. All documents and forms should clearly indicate that they are available in alternate formats.
We note in this report the many areas in which improved communication and outreach are required. There is significant work to be done to improve access to disability tax measures by Indigenous peoples. Many are unaware of various tax measures or do not believe they would be eligible to apply.
The Committee was pleased to learn that the CRA recently reorganized its operations by creating a new Disability, Indigenous, and Benefits Outreach Services Directorate. It will reach out specifically to populations that have largely been excluded from tax reductions and tax-delivered income programs.
Other barriers include access to qualified health providers to complete the Form T2201. The Committee has received requests from health provider groups not currently deemed qualified to complete the T2201. These provider groups cited better access as the chief reason why their qualification was necessary. In this third annual report, the Committee recommended that rather than making ad hoc legislative changes as each new provider group seeks eligibility, the CRA should seek one legislative change, entitling any regulated health provider to complete a T2201 in areas consistent with their legislated scope of practice.
Our Committee explored the application of the Jordan’s Principle to the DTC and found that the expense involved in completing the Form T2201, at least for Indigenous children, would be covered by the federal government. Jordan’s Principle was named in memory of Jordan River Anderson. Its purpose is to guarantee that all First Nations children, regardless of their place of residence or condition, have access to the services they require to support their development and meet their needs.
However, more work is required to improve access to disability tax measures and various tax-delivered benefits. Current activities and plans are discussed in the section on Indigenous Issues.
Finally, the Committee has done considerable analysis of DTC data. This analysis provided a picture of trends over time and helped us identify several “red flags” that we highlighted in our previous annual reports. These concerns are discussed in the section on DTC Data.
One notable issue involved the relatively low uptake of the DTC in Quebec. We recently learned that Employment and Social Development Canada (ESDC) has funded a Quebec-based study to determine why this is the case. Lack of information might be the problem. Alternatively, some potential applicants may believe that they cannot claim both the Quebec disability tax credit and the federal DTC at the same time. Either way, the results of this study will be important for DTC communication and outreach in future.
The disability landscape
Before discussing the Committee’s ongoing work, it is important to highlight several notable changes in the disability landscape that have affected our recent discussions. Perhaps the most significant development was the 2020 federal Throne Speech announcement of a Disability Inclusion Action Plan, which will focus on:
- reducing poverty among persons with disabilities
- getting more persons with disabilities into good quality jobs
- helping to realize the goal of the Accessible Canada Act to achieve a barrier-free Canada
- making it easier for persons with disabilities to access federal programs and services
- fostering a culture of inclusion
The Committee was especially pleased to see reference to the federal government’s plan to introduce a Canada Disability Benefit, which it indicated would be modelled on the Guaranteed Income Supplement for older Canadians. The proposed new benefit could go a long way toward reducing the high rate of poverty among persons with disabilities.
Our Committee had also responded positively to the June 2020 federal announcement of a one-time, tax-free, non-reportable payment recognizing that most persons with severe and prolonged disabilities faced extraordinary pandemic-related costs.
In our second annual report, we noted the limitations in using the DTC as the primary eligibility criterion. Because this tax credit alone proved to be too narrow an eligibility screen, other disability-related programs had to be added to broaden the entry point to the new one-time benefit. The COVID-19 Disability Benefit was eventually paid to all DTC recipients.
This problem proved to be an important lesson in light of the Canada Disability Benefit that the federal government proposed in the Throne Speech. The DTC alone cannot be the sole entry point for this new program. We discuss this issue later in our report.
The Committee notes as well the significance in the disability landscape of the obligations set out in the Accessible Canada Act, which took effect in July 2019. The Act creates a framework to identify, remove and prevent barriers to accessibility and the inclusion of persons with disabilities.
The work of our Committee was also influenced by the fact that Canada is a signatory to the United Nations Convention on the Rights of Persons with Disabilities (CRPD). Its purpose is to promote, protect and ensure the full and equal enjoyment of all human rights and fundamental freedoms by all persons with disabilities and to promote respect for their inherent dignity. Ratification of the Convention obliges signatory state under international law to implement its provisions.
Perhaps most significant from our perspective is the intent of the Convention to move away from a medical model of disability. The DTC, in particular, is a step in this direction because it employs functional capacity as the key eligibility criterion. However, the DTC still requires qualified health providers to attest to the type and degree of functional impairment, which is of course the foundation of the medical model of disability.
The conflict of social and medical models is well illustrated in the DTC. Eligibility criteria are based on function, all or substantially all of the time. While it is applicants and their close contacts who have a first-hand understanding of their function all or substantially all of the time, applications still rely on the judgment of a health provider. The Committee has frequently pointed out that health providers are not with the applicants all or substantially all of the time.
This tension remains unresolved to this day. It will likely continue to present challenges as the federal government contemplates ways to modernize the eligibility process for disability benefits and programs.
Summary
The Committee is pleased that many of our DTC-related recommendations have been implemented. We also note that our concerns regarding longer-term income security improvements are being taken into consideration by the federal government.
Significant work remains, however, with respect to DTC eligibility criteria and administrative procedures, Indigenous issues, DTC data, Registered Disability Savings Plans (RDSPs) and work-related tax measures. We turn now to these areas of ongoing work.
Part 2: DTC Eligibility
Introduction
In this section and throughout our report, the Committee has used the term ‘impairment’ in function because it is consistent with the language in the Income Tax Act and the DTC application Form T2201 (Appendix F). However, we have always been concerned about the impact of language and have tried to encourage the use of terminology that is more consistent with the intent of the UN Convention on the Rights of Persons with Disabilities.
In both this section and our report, we have retained the term ‘impairment’ for consistency with current legislative and administrative language as well as our earlier recommendations. However, we propose that the term ‘limitation’ be used in all future CRA documents and Committee reports. Moreover, we recommend:
That, in respect of the intent of the Convention on the Rights of Persons with Disabilities, the Department of Finance Canada and the CRA change the term ‘impairment’ to ‘limitation’ in all of its relevant legislation and administrative procedures and documents.
i. New definition of mental functions
Over the years, it has become clear to the Committee and the disability community, more generally, that most of the eligibility challenges linked to the DTC have arisen around impairment in mental functions. There are problems with respect to how mental functions are defined in the Income Tax Act and how they are assessed on the DTC application Form T2201.
The policy and administrative challenges related to the DTC are not new. They have been documented by many organizations and in various reports for nearly 20 years. Applicants and their families have raised a wide range of concerns, including the complexity of the eligibility criteria. Health providers also told us about the difficulties they face in completing the Form T2201, particularly with respect to impairment in mental functions. Challenges include the fact that the DTC eligibility criteria are not clinically meaningful (e.g. they confuse functions with activities and do not contain a complete list of mental functions) and that the CRA would regularly send requests for additional information to supplement the extensive DTC application already provided.
In 2003, the federal government created the Technical Advisory Committee (TAC) on Tax Measures for Persons with Disabilities. While the TAC made a number of recommendations for reforming the DTC, it identified impairment in mental functions as the most significant eligibility challenge. One of the most important recommendations made by the TAC was a redefinition of mental functions to one that was more accurate, and thereby more fair, when assessing eligibility on the basis of a mental disorder.
The TAC defined mental functions as the range of processes that govern how people think, feel and behave. These processes include “memory, problem solving, judgment, perception, learning, attention, concentration, verbal and non-verbal comprehension and expression, and the regulation of behaviour and emotions.” These processes cover the range of functions upon which we all rely to accomplish the activities of everyday life, such as self-care, health and safety, social skills and simple transactions.
The Income Tax Act was amended in 2005 to modify the definition of mental functions necessary for everyday life. Unfortunately, the amendments at that time were far from what the TAC had recommended and provided little clarity to applicants and to health providers when completing applications for the DTC.
More specifically, the definition of mental functions was modified in the Income Tax Act to read as follows. It remained this way on the application Form T2201 until its recent 2022 update:
- adaptive functioning (for example, abilities related to self-care, health and safety, abilities to initiate and respond to social interactions, and common, simple transactions);
- memory (for example, the ability to remember simple instructions, basic personal information such as name and address, or material of importance and interest); and
- problem-solving, goal-setting, and judgment, taken together (for example, the ability to solve problems, set and keep goals, and make the appropriate decisions and judgments)
It is not clear how the federal government arrived at this redefinition of mental functions. It did not accurately reflect the recommendation on mental functions that the TAC had made. More importantly, the redefinition made no clinical sense for the following reasons:
- It included some but not all mental functions as noted in the redefinition the TAC had proposed
- It required a conjunctive interpretation of problem solving, goal setting and judgment. The requirement not only makes no clinical sense but also discriminates against people with mental disorders since no other category of eligibility (e.g., walking, seeing, speaking) requires a conjunctive presence of multiple symptoms.
- It is a mix of functions and activities. Adaptive functioning is not a mental function. The accomplishment of adaptive activities depends on mental functions. For example, in order to ride a bus or make a purchase in a grocery store, one must be able to attend, learn, make judgments and interact with others.
When the Committee began our work in 2018, one of our first tasks was to identify the many concerns regarding the 2005 revision to the mental functions definition in the Income Tax Act. We reviewed the proposals of the earlier Technical Advisory Committee which, in our view, were still sound.
In 2018, the Committee also carried out an extensive pan-Canadian survey of health providers and received more than 1,100 responses. While the respondents represented several different health professions, psychologists and physicians described the challenges they faced in trying to interpret the impairment in mental functions provisions.
Survey respondents made clear that the eligibility criteria for this functional area are neither clinically meaningful nor easy to understand. The large volume of clarification letters sent by the CRA to health providers completing the application on behalf of persons with impairment in mental functions confirmed the many challenges with the current definition.
The first recommendation in our first annual report proposed that the principle of parity guide CRA actions with respect to physical and mental functions. By this, we meant that the treatment of persons with impairment in mental functions should be the same as those with impairment in physical functions. There should be no additional barrier or higher eligibility bar for applicants with impairment in mental functions.
By requiring a conjunctive presence of impairment in multiple mental functions, an inequity has been created and perpetuated. As noted, no other category of eligibility (e.g., walking, seeing speaking) involves a conjunctive presence of multiple impairments.
Requiring problem solving, goal setting and judgment to all be impaired for a person with a mental disorder to qualify for the DTC is like requiring a person’s nerves, muscles and bones all be impaired for a person who cannot walk. Just as a person with nervous system impairment alone is eligible for the DTC if they cannot walk, a person whose judgment alone is so impaired that they cannot engage in the adaptive activities of everyday life should also be eligible for the DTC.
To address these issues, the Committee searched various international classifications of mental functions to ensure that our proposed new definition would be consistent with clinically recognized and respected taxonomies. Our reformulation of the definition of mental functions derives from international classifications from both the World Health Organization and the U.S.-based National Institute of Mental Health. As noted, we also considered the data from the health providers we surveyed who reported their challenges with Form T2201.
Our goal was to ensure that a revised list of mental functions would make clinical sense, be more clear to applicants and health providers, and be more easily interpreted by the CRA. In Recommendation #2 of our earlier annual reports, we proposed:
That the CRA amend the list of mental functions on Form T2201 as follows:
- attention
- concentration
- memory
- judgment
- perception of reality
- problem solving
- goal setting
- regulation of behaviour and emotions (for example, mood disturbance or behavioural disorder);
- verbal and non-verbal comprehension
- learning.
The Committee took this recommendation even one step further by providing a definition of marked restriction in mental functions. Our Recommendation #7 proposed:
The individual is considered markedly restricted in mental functions if, even with appropriate therapy, medication and devices (for example, memory and adaptive aids):
- all or substantially all the time, one of the following mental functions is impaired, meaning that there is an absence of a particular function or that the function takes an inordinate amount of time:
- attention
- concentration
- memory
- judgment
- perception of reality
- problem solving
- goal setting
- regulation of behaviour and emotions (for example, mood disturbance or behavioural disorder);
- verbal and non-verbal comprehension; or
- learning
Or
- they have an impairment in two or more of the functions listed above none of which would be considered a marked restriction all or substantially all the time individually but which, when taken together, create a marked restriction in mental functions all or substantially all the time;
Or
- they have one or more impairments in mental functions which are: intermittent; and/or unpredictable; and when present, constitute a marked restriction all or substantially all the time.
The Committee was pleased to see that the federal government announced in the 2021 Budget its intent to revise the definition of mental functions in the Income Tax Act. The announcement was a recognition of the many problems in the definition of impairment in mental functions upon which eligibility for the DTC relies. While the proposed change was consistent with our Recommendation #2, it also differed somewhat from our proposal.
In its 2021 Budget, the federal government proposed the following list for its new definition of mental functions:
- attention
- concentration
- memory
- judgement
- perception of reality
- problem solving
- goal setting
- regulation of behaviour and emotions
- verbal and non-verbal comprehension
- adaptive functioning
The Committee was generally supportive of this proposal, which we conveyed in a written submission to the Department of Finance Canada. On the plus side, the federal proposal allows for the disjunctive, rather than conjunctive impairment in problem solving, goal setting and judgment. As noted, there is no conjunctive requirement for any of the identified physical functions. The removal of this requirement is an important step toward parity in the treatment of physical and mental functions.
We were also pleased that the federal proposal largely reflects the list of mental functions that our Committee had presented. We believe that the new list more closely reflects actual mental functions, all of which affect the ability to carry out the activities of daily living. We are concerned, however, about two of the changes that the federal government proposed regarding mental functions.
First, the new definition removed “learning” as a mental function, which was the final entry on our proposed list. We had included “learning” on the list of mental functions for an important reason. We had heard from many health providers, through both focus groups and our health provider survey, who believed that applicants with a severe learning disability would not be eligible for the DTC.
This perception that people with learning disorders are categorically ineligible is not accurate. There is no condition or impairment in function that is categorically excluded from DTC eligibility. While it may be true that learning depends on functions already on the list (e.g., attention, concentration, problem solving), it is also true that applicants and health providers appear to believe that no one with a learning disability would be eligible for the DTC.
It will be important to make clear, in DTC communications and through examples on the Form T2201, that someone with a learning disability may be eligible for the DTC if the learning disability prevented them from engaging in the adaptive activities in everyday life. This might be the case, for example, if a person’s learning disability was so profound that they couldn’t follow directions, make a bank deposit or make a store purchase.
The Committee concluded that omitting learning from the new list of mental functions is not necessarily a problem since learning depends on the ability to attend, concentrate, remember and solve problems – all of which are on the list of functions. As noted, it would be important for the CRA to make clear by example and communication that someone with a learning disability is not necessarily categorically ineligible for the DTC.
The federal government made a second change to the Committee’s proposed list of mental functions. It included “adaptive functioning.” We were concerned to see this addition because the confusion that has long existed among health providers when completing the T2201 is in large measure because the eligibility criteria treats activities as functions.
As mentioned above and in our two previous annual reports, adaptive activity itself is not a mental function. Rather, adaptive activities depend on mental functions. In our view, including adaptive functioning does nothing to make the proposed new list more clear and clinically relevant. In fact, it may perpetuate confusion for health providers who complete the T2201 on behalf of applicants with impairment in mental functions.
In the call by the Department of Finance Canada for public feedback on the proposed legislative change, we pointed out these weaknesses in the hope that these areas could be addressed prior to being introduced into law. We came to understand that adaptive functioning was included out of concern that its exclusion might leave out some applicants who had previously qualified because their ability to carry out adaptive functions was impaired.
We believe that a few factors can mitigate this concern. A critical component of eligibility is that the mental function is so impaired that it prevents adaptive activity all or substantially all of the time. This can be made clear in the form with the use of examples about how disorders in function lead to impaired adaptive activity. It would not be possible to have an impairment in adaptative activities without a disorder of function – following directions, making change in a store, undertaking basic social transactions all depend on mental functions.
Further, to be eligible under mental functions, the adaptative activities that the applicant is unable to perform are very basic ones. A person’s memory must be so impaired, for example, that they cannot make a transaction in a store or follow directions. One will not be deemed eligible for the DTC if one’s memory impairment gets in the way of learning to do complex activities like performing calculus or playing bridge. Just as is the case for learning, we believe that communications and examples of mental functions must make clear that impairments must be severe enough to get in the way of very basic adaptive activities.
Despite the concerns noted above, we supported the proposed changes to the list of mental functions because they are a preferable alternative to the current definition in the Income Tax Act. In our submission to the Department of Finance Canada, we also pointed out other areas of concern. The federal proposal made no reference to the other components with respect to marked restriction in mental functions that we had recommended. These are:
Or
- they have an impairment in two or more of the functions listed above none of which would be considered a marked restriction all or substantially all the time individually but which, when taken together, create a marked restriction in mental functions all or substantially all the time;
Or
- they have one or more impairments in mental functions which are: intermittent; and/or
unpredictable; and when present, constitute a marked restriction all or substantially all the time.
The Committee believes it is essential to make clear that severe and prolonged restriction can be created by impairment in two or more mental functions, when none of the functions creates severe and prolonged impairment on its own.
In addition, the often unpredictable and episodic or intermittent nature of the symptoms of some mental disorders creates severe and prolonged impairment. This fact should be acknowledged in the eligibility criteria.
Our Committee will continue to advocate for these changes. We believe that they are critical in recognizing the potentially profound impact of impairment in mental functions.
We appreciate that, at the time of this writing, the implementation of the proposed legislative changes to the DTC were underway. As of June 23, 2022, the criteria for mental functions and life-sustaining therapy were expanded as detailed above. We respect the intent that these measures would create a fairer and clearer application process and result in more families and people living with disabilities qualifying for the DTC. As mentioned, these changes were very positive but fell short of our recommendations.
It is clear that the changes implemented in June 2022 were informed by our recommendations. The Committee’s understanding of the experiences of relevant stakeholder groups (e.g. health providers, persons with lived experience of disability) can help ensure that legislative changes meet their intended objectives.
Consultation before any future proposals are finalized will help ensure an accurate understanding and interpretation of our recommendations. Fairness for applicants, clarity for health providers and efficiency in the administration of the DTC will more likely be achieved if this consultation is considered.
ii. Interpretation of the new definition
The Committee hopes that the CRA will introduce appropriate administrative solutions to clarify the interpretation of the revised definition of mental functions. The Form T2201 can provide valuable guidance to health providers.
To enable the interpretation of the new definition of mental functions, the Committee suggested that various examples be developed to explain how each of the identified mental functions on the list can be interpreted. In Recommendation #8 of our first two annual reports, we proposed:
That the CRA remove specific references to activities in the T2201 section on mental functions and include examples of activities in the current Guide RC4064 to help health providers detail all the effects of the markedly restricted mental function(s), as in the following illustration:
“The individual is considered markedly restricted in mental functions if they have an impairment in one or more of the functions all or substantially all of the time or takes an inordinate amount of time to perform the functions, even with appropriate therapy, medication, and devices. The effects of the marked restriction in mental function(s) can include, but are not limited to, the following (this list is illustrative and not exhaustive):
- with impaired memory function, the individual cannot remember basic information or instructions such as address and phone number or recall material of importance and interest;
- with impaired perception, the individual cannot accurately interpret or react to their environment;
- with impaired learning or problem solving, the individual cannot follow directions to get from one place to another or cannot manage basic transactions like making change or getting money from a bank;
- with impaired comprehension, the individual cannot understand or follow simple requests;
- with impaired concentration, the individual cannot accomplish a range of activities necessary to living independently like paying bills or preparing meals;
- with impaired ability to regulate mood (for example, depression, anxiety) or behaviour, the individual cannot avoid the risk of harm to self and others or cannot initiate and respond to basic social interactions necessary to carrying out basic activities of everyday life; or
- with impaired judgment, the individual cannot live independently without support or supervision from others or take medication as prescribed.
These examples make clear that the impairments in mental functions must be severe and significant enough that they impact the adaptive activities of everyday life, such as remembering a phone number, following directions and assessing the risk of harm. It would also be helpful for the CRA to conduct surveys or organize focus groups involving health providers to determine whether ongoing improvements to the paper format and electronic applications are required. Respondents may contribute additional examples or helpful clarifications.
The Committee recognizes the need to keep the written Form T2201 to a reasonable length. Fortunately, the electronic application makes it easier to modify various examples or to include new ones.
We were pleased to learn that early feedback from health providers on the electronic application has been positive. We suggest that the CRA continue to update the Committee on a regular basis regarding the content and implementation of the electronic form.
iii. Consistency across impairments
We noted in our first two annual reports the inconsistency in the physical and mental functions set out in the Income Tax Act and Form T2201. Some of the impairments listed as grounds for DTC qualification are functions. They include vision, speaking, hearing, eliminating and eating.
Other categories, notably walking and dressing, represent impairments in activities. Mental functions, as noted, combine an incomplete list of functions (memory, problem solving, goal setting and judgment) as well as activities (adaptive functions).
There is a need for consistency across impairments that grant eligibility for the DTC. It is essential to make a clear distinction between a function or series of functions that are necessary for an activity.
Some activities may be affected because of one or several impairments – e.g., an individual cannot dress because of visual spatial impairment or cannot walk because of upper extremity impairment, fatigue and/or lower extremity impairment.
In fact, the Committee proposed in Recommendation #10 in our first two reports that the CRA revise the list of functions on Form T2201 as follows:
- vision
- speaking
- hearing
- lower-extremity function (for example, walking)
- upper-extremity function (for example, arm and hand movement)
- eliminating
- eating/feeding
- mental functions
The Committee acknowledges that this proposed list would require an update to the Income Tax Act. Because the Form T2201 must reflect the wording of the Act, the CRA cannot introduce this change on its own. But it certainly is an area worth discussing with the Department of Finance Canada.
In Recommendation #11, we made an associated proposal regarding the preparation of a list of activities associated with each impaired function. More specifically, the Committee suggested:
That the CRA create a list of examples of activities for each impaired function for inclusion in Guide RC4064 to help health providers detail all the effects of markedly restricted function(s), as in the following proposed guidelines (this list is illustrative and not exhaustive):
- with impaired lower-extremity function, the individual cannot walk
- with impaired upper-extremity function, the individual cannot feed or dress themselves, or cannot attend to basic personal hygiene
- with impaired eating/feeding, the individual cannot swallow or eat food
Once again, it is possible that some of these areas can be clarified with examples in the drop-down menus of the electronic DTC application. While legislative change is clearly desirable, it is still feasible for the CRA to address the intent of this recommendation through administrative improvements that help achieve its purpose.
iv. The 90% guideline
In order to qualify for the DTC, the mere presence of impairment is not sufficient. Rather, the effect of the impairment upon the basic activities of daily living must be severe and prolonged. In fact, the restriction must be present all or substantially all the time, which has been interpreted by the CRA to generally mean at least 90% of the time.
During the first year of our mandate, discussions around this recommendation were held with Department of Finance Canada officials who raised two issues. First, they argued that a numeric standard provides a more rigorous guideline for decision-making than a set of qualitative benchmarks alone. Second, they noted the policy precedent for this percentage. The 90% guideline is employed in several other contexts, including business and charitable accounts.
Our first annual report documented the many problems with this guideline when applied to the DTC. This requirement acts as a major barrier to DTC eligibility, particularly for persons with impairment in mental functions or other physical conditions (e.g. Multiple Sclerosis) which have many symptoms, some or all of which may be episodic. Symptoms which may be present only 50% of the time, can be as debilitating to the performance of adaptive activities as other symptoms that may be present all of the time.
Take, for example, an individual whose memory or perception of reality is impaired 50% of the time. That person is likely seriously and significantly impaired, and undoubtedly would require a combination of supports, remedial treatments and devices, or medication. Add to that list the fact that intermittent or episodic symptoms are often unpredictable. It is easy to see that if one has a mental or cognitive disorder that results in severe but unpredictable impairment in memory or judgment even 50% of the time, successfully finding the way home from an errand or managing a transaction online or in the store could be at significant risk.
The Committee has also pointed out in the past that there is no basis in law for the 90% guideline. In fact, several judgments in Tax Court cases involving impairment in mental functions have challenged the use of the 90% guideline. It is an administrative practice that is employed to provide a guideline to practitioners and assessors of DTC applications.
In Recommendation #6 of our first and second annual reports, the Committee proposed:
That the CRA no longer interpret all or substantially all as 90% of the time and no longer interpret an inordinate amount of time as three times the amount of time it takes a person without the impairment.
We were pleased to learn that the CRA has agreed to exclude explicit reference to 90% in the DTC electronic application. In addition, DTC assessors now have access to the guidelines in the document Mental functions necessary for everyday life. The guidelines permit more flexibility in the interpretation of “all or substantially all of the time” by noting that the effects of the impairment must be present and challenging “most of the time” rather than the arbitrary 90% rule.
v. Automatic eligibility
While the question of whether certain conditions can create automatic eligibility for the DTC is not new, it remains a challenge. There is no doubt that the presence of certain conditions will likely be associated with higher disability-related costs. In our first two annual reports, we recognized this reality in Recommendation #15:
That the CRA:
- consider whether some conditions, such as a complete paraplegia or tetraplegia, schizophrenia or a permanent cognitive disorder with a MOCA below 16, should automatically qualify for the DTC in the way that blindness does. (MOCA is a mental status examination of cognitive functions used commonly to assess impairment that results from conditions such as dementia, brain injury or stroke); and
- examine the eligibility criteria employed in other federal and provincial/territorial programs, such as the Ontario Disability Support Program and the programs for Canada Pension Plan disability benefits and veterans’ disability pensions to identify the conditions/diagnoses that establish automatic eligibility for those programs
The purpose of this recommendation was to enable access to the DTC. The Committee noted that while diagnosis alone should not necessarily qualify someone for the DTC, the presence of a particular condition may help CRA assessors make their eligibility determinations. Certain conditions, such as paraplegia or dementia, have a predictably stable impact upon daily functioning. Moreover, there is precedence for automatic eligibility – applicants who are blind automatically qualify for the DTC.
At the same time, we acknowledged the problems embedded in this approach. A specific diagnosis does not necessarily result in – or equate with – serious impairment in activity.
We also acknowledged that designated lists in any area of public policy invariably raise questions of fairness about the groups, items or conditions that were left out.
In addition, social models of disability encourage us to consider not just the impairment but the way in which society accommodates impairment. For example, someone who is paraplegic with a fitted wheelchair, transportation, and a community that supports wheelchair use will have less difficulty in accomplishing the activities of everyday life than somebody who does not have access to these resources. After all, the DTC is a tax measure intended to help people reduce their costs because, to some significant degree, society does not accommodate them.
This is clearly a complex recommendation that will need to be revisited in future. It will no doubt come up as an issue as the federal government works to update its procedures involved in disability determination, which we noted in the first section of this report.
vi. Qualified health providers
Throughout our mandate, the Committee has heard from various organizations seeking to expand the list of health providers approved to complete the Form T2201. There were several factors that prevented us from making a recommendation one way or the other about adding other health providers to the list:
- To the best of our knowledge, there are no criteria in place with which the government decides on the inclusion of specific health provider groups and not others.
- We felt that neither our Committee nor the CRA had the authority to expand the list of health providers. Since they are listed in the Income Tax Act, we assumed that the Department of Finance Canada had this authority.
- It is our view that even with the authority, neither the CRA nor the Department of Finance Canada has the expertise to decide which health providers have or do not have the licensed skill sets necessary to support an application for the DTC.
- We felt that we did not have sufficient information about the nature and extent of the difficulty in accessing health providers to complete the T2201 that some had suggested. Several professional groups lobbying to expand the list of health providers had cited the access problem.
The Committee suggested that the CRA include a question in its Client Experience Survey and any other relevant communications, asking about access challenges with respect to the designated health providers identified on Form T2201. We also had proposed the following action in Recommendation #19:
That the CRA develop a process for expanding the list of health providers with the appropriate expertise who can assess eligibility for the DTC.
This recommendation recognized that the CRA likely would receive requests on an ongoing basis to update and expand the list of health providers who can assess for DTC eligibility. We suggested the development of criteria to guide any expansion of the list in future.
Following our second annual report, the Committee struck a Health Provider Task Group, which came up with additional proposals to address this issue. The Task Group suggested that any regulated health provider be allowed to complete the Form T2201 on behalf of applicants.
As a set of new recommendations, the Committee proposes:
That neither the CRA nor Finance decide which health provider can complete the form for which functions but rather let the licensed scope of practice of a health provider guide which functions they will assess on behalf of the DTC applicant.
That any licensed health provider, whose license is in good standing, be permitted to complete the T2201 for any area of function.
We are making these recommendations for the following reasons:
- Health providers are accountable to their licensed scope of practice and transgressing that scope places their license in jeopardy. For instance, an optometrist’s license would not permit them to assess or treat an individual with impaired elimination. A psychologist’s license would not permit them to assess or diagnose diabetes. Accordingly, it is unlikely that a health provider would attest to an area of function around which they had no expertise. Further, if the CRA queried whether a health provider had the expertise to assess the area of function upon which the T2201 is based, they can ask for justification.
- The current assignment of health providers to areas of function is not entirely accurate. An impairment in dressing, for example, may be due to a cognitive impairment (e.g., impaired visual spatial skills) rather than just a motor problem in moving one’s arms. While psychologists are often the health providers who assess and diagnose visual spatial impairment, only occupational therapists, physicians and nurse practitioners can currently complete the Form T2201 for individuals with dressing impairments.
- Allowing the licensed provider to complete the Form T2201 guided by their licensed scope is simpler for the government. It would no longer need to set criteria or make decisions about expanding the list of eligible health providers. The purpose of regulating health professions is public protection to ensure that health providers have the knowledge and skills necessary to assess and treat health problems, and to make these professionals accountable to their knowledge and skills. If they certified an illness or condition without requisite skill, much more is at risk than is gained by completing a Form T2201.
vii. Life-sustaining therapy
The federal Budget 2021 also included a proposed legislative change to the definition of life-sustaining therapy for the purposes of DTC eligibility.
Right now, applicants may be eligible for the DTC if they require life-sustaining therapy. A medical doctor or nurse practitioner must certify that several conditions are met.
An individual must require this therapy in order to support a vital function. This condition applies even if the therapy has eased the symptoms. Previously, the applicant needed this life-sustaining therapy at least three times a week and for an average of at least 14 hours per week. The adoption of proposed changes in Budget 2021 reduces this requirement from three to two times a week.
Over the course of our mandate, the Committee heard several concerns about the eligibility criteria for life-sustaining therapy. These concerns are documented in our first annual report. Perhaps most important, there were questions about the empirical basis for the 14-hour minimum weekly time requirement.
The 14-hour rule includes only the time related to the actual therapy. The requirement assumes that people must take time away from their normal everyday activities in order to receive the therapy. The time may also be spent administering life-sustaining therapy to a child.
In reviewing the eligibility criteria, the Committee has always believed that the requested information on the Form T2201 was too intrusive and likely unnecessary. By definition, a life-sustaining therapy must be frequently administered.
We also wanted to modernize the definition of life-sustaining therapy. Instead of asking health providers for details that they may or may not have, we thought it would be more appropriate to grant DTC eligibility according to the type of therapy required. In fact, very few therapies actually would qualify under the revised definition that we had proposed in Recommendation #14 of our first two annual reports (which we have modified slightly for the purposes of this report):
That the CRA replace the current eligibility criteria for life-sustaining therapies as set out in Form T2201 with the following:
Individuals who require life-sustaining therapies (LSTs) are eligible for the DTC because of the time required to administer these therapies. These are therapies that are life-long and continuous, requiring close medical supervision. Without them, the individual could not survive or would face serious life-threatening challenges. Close medical supervision is defined as monitoring or visits, at least several times annually, with a health provider. These therapies include but are not necessarily limited to: intensive insulin therapy for type 1 diabetes; chest therapy for cystic fibrosis; renal dialysis or chronic and permanent renal failure; intravenous feeding for certain genetic conditions and Crohn’s Disease; and foods for metabolic conditions that prevent the safe breakdown of proteins by the liver, including medically prescribed formulas and foods for phenylketonuria (PKU) and Maple Syrup Urine Disorder (MSUD).
The DAC recommendation basically proposes that any condition which requires life-sustaining therapy, as clearly defined in the above recommendation, should be eligible for the DTC. In our view, the calculation of frequency and time spent are often not readily verifiable by a health provider and should not be required.
The legislative amendment proposed in the federal Budget 2021 basically kept the current LST definition in place. It slightly altered the existing definition by reducing the LST administration from three times to twice weekly.
The amendment also spells out the activities that may or may not be counted in the calculation of the 14-hour rule. These activities include, for example, determination of the dosage of medication; consumption of medical food, formula or compound; and supervision of children or those unable to attend to LST without supervision.
In addition, due to the legislative amendments, an individual diagnosed with type 1 diabetes is now deemed to have met the 2 times and 14 hours a week requirements for life-sustaining therapy. The updated criteria will make it easier for individuals to be assessed and give more eligible people access to the DTC and other benefits.
Committee members would have preferred that the legislative change introduce a more significant reform than the one actually proposed. Nonetheless, we expressed our support for the new measure in that it is a step – albeit a modest one – toward simplifying the DTC eligibility provisions.
Part 3: Ongoing Committee Work
DTC review and appeals
i. Mental functions
The Committee has always been concerned about the eligibility challenges faced by applicants with impairment in mental functions. They face barriers to access and their applications are often denied by the CRA or are sent back to health providers with a request for clarification. Many health providers have informed us that the additional information they submit to the CRA is often identical to or only slightly different from the original application.
In order to reduce the number of cases that go to review, the Committee had proposed the following process in Recommendation #24 in our first and second annual reports:
That in the case of determining DTC eligibility for persons with impairment in mental functions, the CRA include relevant specialized health providers, including, but not limited to, psychiatrists and psychologists, in the review process when applications are disallowed.
In response to this recommendation, the CRA made a commitment to provide better and more consistent training to current and new assessors of DTC cases that involve an impairment in mental functions, and to consult with mental health professionals around selected cases.
All applications denied the DTC involving impairment in mental functions are sent for secondary review by a CRA team not involved in the initial decision.
DTC assessors as well as DTC Objections Centres of Expertise also have access to the guidelines in the document “Mental Functions necessary for everyday life.” The guidelines permit greater flexibility in the interpretation of “all or substantially all of the time” by noting that the effects of the impairment must be present and challenging “most of the time” rather than the arbitrary 90% rule. As noted in an earlier section, the Committee proposed in Recommendation #6 of our first and second annual reports:
That the CRA no longer interpret all or substantially all as 90% of the time and no longer interpret an inordinate amount of time as three times the amount of time it takes a person without the impairment.
The Committee can also monitor progress in this area by continuing to review the DTC data and the approvals with respect to the various functional categories. We can flag concerns related to a drop in approvals related to mental functions.
ii. Improved procedures
The Committee’s earlier annual reports described a range of concerns regarding the DTC assessment process and associated eligibility decisions. We put forward several recommendations to simplify the review process and to make it easier for Canadians to understand and access its various components.
Applicants have the right to challenge decisions with respect to their claim for the DTC. The Appeals Branch has developed an income tax decision tree to explain the process if DTC applicants choose to object to a CRA determination. The decision tree guides them through a series of steps based on their personal circumstances. It is available here: Income tax objections decision tree - Canada.ca.
The Committee had argued that greater awareness of the review process for DTC decisions would help resolve cases at an earlier stage and reduce the need for DTC applicants to challenge decisions regarding their case. We also proposed in Recommendation #23 a broader review:
That the Minister of National Revenue review the current appeals process with a view to creating a straightforward, transparent and informed process where the applicant has access to all relevant information (including the precise reason their application was denied) and documents (including copies of all information submitted by health providers that pertain to their application).
Briefly, there are three main routes to challenge DTC decisions: case review, Notice of Objection and Notice of Appeal. We described these steps in more detail in our second annual report.
For a case review, applicants who receive a Notice of Determination disallowing the DTC are advised that they can request a review of their case. Applicants are required to provide additional relevant medical information that had not already been included with the Form T2201 and clarification letter.
Applicants may also choose to formally object to the initial decision by filing a Notice of Objection, Form T400A, with the Appeals Branch of the CRA (a letter is also acceptable).
Applicants may file an objection regarding a DTC Notice of Determination if they think that the CRA misinterpreted the facts of their circumstances or applied the tax law incorrectly.
The CRA has prepared a video on the objections process, which explains how to file an objection or formal dispute about a DTC determination. It is available here: File an objection – Income tax - Canada.ca.
A second video explains what happens when an applicant registers a formal dispute or objection. It is available here: Processing times and complexity levels - Income tax and GST/HST objections - Canada.ca.
The third step in challenging a DTC determination involves appealing to the Tax Court of Canada. Under what is known as the “Informal Procedure,” the applicant can file a Notice of Appeal (at no fee) within 90 days of the date of the Notice of Confirmation outlining the relevant facts and reasons for the appeal.
The CRA Appeals Branch has prepared a video on how applicants can appeal to the Tax Court if they disagree with the CRA regarding their DTC determination. It is available here: File an appeal to the Court - Canada.ca.
While the Tax Court ensures fairness within the legislative and parliamentary intent of the Income Tax Act, the formal legal route is never the most desirable option in any dispute.
Even with these visual aids and explanations, the process remains intimidating and complex. The Committee struck a Review and Appeals Task Group to continue the discussion related to our ongoing concerns. The Task Group proposed that the CRA provide more detailed information about the various steps involved in questioning a DTC decision. The CRA prepared the following flowchart.
Taxpayer appeals the decision on an objection filed with the CRA
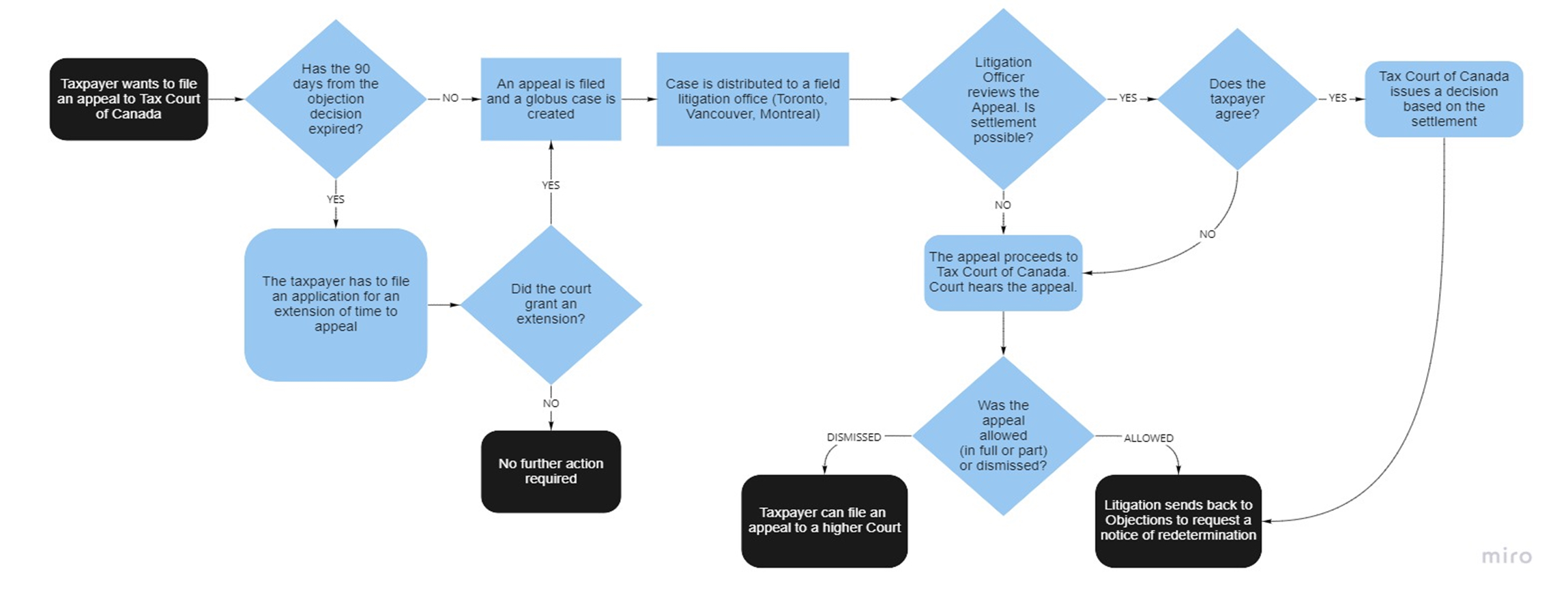
The Task Group also suggested that, in addition to DTC caseload numbers, it would be important to track data on the number of objections and appeals received, approved and rejected. The CRA has informed the Committee that these numbers are, in fact, being tracked by both the appeals Branch and by Navigators. In light of this information, the Committee recommends:
That the CRA shares the data it currently collects on the number of objections and appeals, their nature and the time taken to resolve them in order to determine which groups are experiencing challenges in this regard.
Because of the important gateway role of the DTC, the Task Group wanted to ensure that DTC beneficiaries who are denied eligibility upon request for renewal and then launch an objection or appeal continue to remain eligible for gateway benefits, such as the RDSP and Child Disability Benefit, until the appeal is resolved. The CRA has provided assurance that these gateway benefits are indeed protected. In respect of this fact, the Committee recommends:
That the CRA make clear in its communications that DTC applicants who file an objection or appeal remain eligible for all DTC-related gateway benefits until such time as the objection or appeal is resolved.
Finally, the Task Group undertook an initial review of the language used in the CRA Notice of Determination letters. The review found repeated use of the 90% interpretation of “all or substantially all of the time,” despite the fact that the Committee has been calling for an end to this interpretation.
In our earlier annual reports, the Committee had also expressed concern about the standard being used to determine “hearing” limitations. The Notice of Determination letters use “in a quiet setting” as part of the test. Task Group members questioned whether this requirement recognizes the reality of people’s work lives or their ability to function in a variety of settings.
Under mental functions, the Notice of Determination letter states: “For this credit, difficulties in areas such as working, housekeeping, recreational activities, academic skills (e.g., in mathematics or languages) managing a bank account, and/or driving a vehicle are not considered.” This language does not appear to acknowledge that limitations are increased by barriers within the community. Disability should not be defined simply by an individual’s limitations but also by the barriers that prevent their full participation and citizenship.
The sample language also includes: “Eligibility for the disability tax credit is based on the effects of impairment not on the condition itself.” In relation to mental functions, the Committee has raised questions as to whether a combination of diagnosis and functional limitations or impairments might be used. Mental health conditions are not necessarily a static condition but can fluctuate over time.
Another sample phrase states that: “Children who are not eligible for the disability tax credit are also not eligible for the child disability benefit.” Notice of Determination letters should include the other benefits for which applicants who are refused the DTC may be ineligible.
The Task Group proposed that the following statement be inserted at the head of the Notice of Determination letter: “Information in this letter will be provided in alternative format upon request.” The letter might also provide information about the role of Navigators and their ability to assist with the appeals process.
The Task Group inquired as to whether the CRA website, publications, communications and forms have undergone an accessibility audit. All forms should clearly state that they will be provided in alternate format upon request. They all need to run through language, design and cultural sensitivity toolkits/screening. Appendix G provides a list of resources on language and disability to enable this process.
It was suggested that the CRA hire a student from the Ontario College of Art and Design (OCAD) University’s inclusive design master’s program to review sample communications and potentially create a style guide. The CRA should consider a training module on person-first language for anyone responsible for communicating with the public.
The Task Group also proposed a review of wording of CRA communications to address any issues of cultural sensitivity. Our Committee learned, for example, that there is no word for disability in Indigenous languages. Other Indigenous Issues are discussed in the next section of this report.
iii. Promoters Restrictions Regulations
The complexities involved in applying for the DTC have forced many persons with disabilities to seek assistance from tax promoters and others who charge a contingency fee for their services as well as a percentage of the DTC claim if the application is successful.
In our previous annual reports, the Committee acknowledged that many legitimate tax promoters put in substantial time and effort to assist DTC applicants. At the same time, we wanted to ensure that tax promoters were not charging inordinately high fees for their services. Our Committee had recommended that a cap be placed on these services related to an initial application.
The CRA subsequently drafted regulations that would have capped the promoters fee at $100 for the entire DTC process, including any appeals. However, an injunction launched by a BC-based promoters’ group was granted by the Supreme Court of British Columbia. The legal action halted the imposition of the $100 fixed-fee schedule that was due to take effect November 15, 2021.
In response to the BC Court injunction, the CRA reviewed and amended an administrative policy related to the Disability Tax Credit Promoters Restrictions Regulations (the Regulations). The CRA’s interpretation of the term “disability tax credit request,” for the purposes of the Regulations, no longer includes the filing of a Notice of Objection. This means the maximum fee of $100 will not apply to work done to assist with the filing of Notices of Objection.
DTC Legal Issues
Several legal issues related to the DTC were brought to the attention of the Committee. These pertain to legal representation and the Trust and Principal Residence Exemption.
i. CRA legal representative
If a person with a mental disability is found at any time to be incapable of managing their financial affairs, the CRA requires that another person be named as the legal representative to manage tax matters on that person’s behalf. The definition of legal representative is spelled out in the Income Tax Act (see Appendix H).
The CRA specifies that a legal representative includes “someone with a power of attorney, someone named in a representation agreement or a guardian.” This means that a person with an impairment in cognitive mental function, in particular, must be represented by a legal guardian if they are deemed incapable of managing property or appointing someone as an authorized representative.
In provinces or territories without supported decision-making legislation, a DTC applicant may not meet the legal threshold to grant a power of attorney for property. In this case, a trusted family member would have to be appointed, for CRA purposes, as the person’s legal guardian.
This requirement gives rise several problems. Applying for legal guardianship is often a complicated process, involving capacity assessment of the person with a disability, application with the court, and significant time and cost commitment. Moreover, the appointment of a legal guardian removes the ability of the individual to make decisions regarding their property.
The lack of supported decision-making options in the Income Tax Act contravenes the United Nations Convention on the Rights of Persons with Disabilities, which Canada has ratified. The CRA insistence on the appointment of a legal representative is also inconsistent with social assistance programs across the country, which generally allow for representatives to be named without resorting to legal guardianship.
It is important to note that, in 2004, a CRA Technical Interpretation allowed for “next-of-kin” to qualify as a legal representative of a person with a disability, in accordance with the definition of legal representative in the Income Tax Act.
This Technical Interpretation makes it possible to appoint a representative on an informal basis. It saves cost and time as well as respects personal autonomy. The representative’s involvement in the individual’s personal affairs is limited to tax matters only and their representation can be revoked by the individual at any time. This Technical Interpretation, however, has not been operationalized by the CRA.
The Department of Finance Canada has the authority to amend the Income Tax Act to improve access to CRA-administered measures by persons with impairment in cognitive mental functions. Even in the absence of legislative change, the CRA is able to reform its administrative practices. It can allow these individuals to appoint a representative to support them in managing their tax affairs. British Columbia’s Representation Agreement Act may be an appropriate precedent for CRA to include supported decision-making options for people who currently face barriers to engaging with CRA (see Appendix H).
To resolve the legal representation issue, the Committee recommends:
That the Department of Finance amend the Income Tax Act (ITA) and/or that the CRA amend its policy to allow a person to appoint a representative to support them with respect to the management of their tax affairs. This objective can be achieved by:
- adding “supported decision-maker” to the enumerated legal representatives in the definition of legal representatives in s. 248(1) then adding a new section to the Income Tax Act that sets out the procedure for appointing a supported/supporting decision-maker; or
- revising the policy applying to the appointment of an “authorized representative” such that it applies to people who may not meet the current capacity requirements to carry out this process.
That, as a broader and more long-term strategy, the federal government apply the Peace, Order and Good Government clause to encourage the creation of a national minimum-standard legislative framework for supported decision-making laws. While amending the Income Tax Act would address the issue of accessing CRA services, persons with disabilities face barriers accessing many other supports and services due to the federal government’s general position that it must defer to provincial laws on legal capacity.
ii. Trust and principal residence exemption
The Income Tax Act allows for exemption from capital gains on the sale of a principal residence bequeathed to relatives in a Will. Persons with disabilities can benefit from the exemption under what is known as a testamentary trust. A testamentary trust is a legal relationship within which the trustee manages the assets of a deceased person in accordance with instructions in a person's will.
However, persons with disabilities are not able to benefit from a provision in the Income Tax Act that exempts DTC beneficiaries from capital gains on the sale of a home bequeathed to them through what is known as an inter vivos trust, which is created while an individual is still alive.
In 2019, the Department of Finance recommended that the Minister of Finance amend the Income Tax Act to allow inter vivos trusts, thereby permitting an eligible beneficiary with a disability to claim the exemption. To date, no action has been taken to resolve this issue.
The Committee hopes that the CRA will act to resolve these legal issues. We recommend:
That the CRA encourage the Department of Finance to adopt its recommendation regarding the exemption DTC beneficiaries from the capital gains on the sale of a home bequeathed to them through an inter vivos trust.
Other Disability Tax Measures
As part of the realization of a barrier-free Canada, the Accessible Canada Act aims to advance organizational and cultural change within areas under federal jurisdiction and, more broadly, across Canada. There are several tax measures related to improving accessibility. The disability supports deduction (DSD), in particular, allows the deduction of costs for the purposes of education, training or work, is particularly noteworthy in this regard.
While our Committee proposed several recommendations related to this tax measure in our earlier annual reports, there has been virtually no progress on this front. The suggested improvements set out in Recommendations #40-#42 remain unfulfilled though no less important than when we first put them forward several years ago.
Our second annual report highlighted our concerns regarding the medical expense tax credit (METC). Some of its provisions are confusing, particularly with respect to attendant care. Because the METC is a non-refundable credit, it is of little value to low- and modest-income Canadians.
The income tax system includes a refundable medical expense supplement. This provision was introduced upon the recommendation of the Technical Advisory Committee in its 2004 report Disability Tax Fairness. Yet relatively few Canadians claim this benefit, let alone know of its existence. It should be noted that Quebec also has a refundable tax credit for medical expenses, which is explained in the booklet “Taxation and Persons with Disabilities”: Taxation and Persons with Disabilities (revenuquebec.ca).
These are areas around which future work is required. There will certainly be a need for outreach with respect to these tax measures in addition to all the communication efforts around the DTC, earlier described. Other areas of ongoing Committee work related to Indigenous Issues, DTC data and Registered Disability Savings Plans (RDSPs) are discussed in the next sections.
Canada Disability Benefit
The Committee was pleased to see the 2020 Throne Speech announcement of a new Canada Disability Benefit (CDB). Our first and second annual reports highlighted our concerns about the disproportionately high rates of poverty among persons with disabilities in Canada.
The extent to which the new CDB will reduce poverty will depend, not surprisingly, upon its design. We discuss possible design options for the CDB and their implications in Appendix I.
Regardless of the design that the federal government decides to employ for this new benefit, the Committee believes that it is important to make clear the following points:
- A CDB that is intended to increase incomes to enable beneficiaries to pay for basic needs, such as food, housing and utilities, will not replace the need for the DTC whose purpose is to help offset disability-related costs.
- The DTC is claimed by Canadians of all ages while the proposed CDB will be targeted toward persons of working age. The implications of these age differences are considered in Appendix I.
- The DTC can act as one of several eligibility screens for the new CDB. We acknowledge that significant work is still required to clarify and improve the DTC eligibility criteria. At the same time, we believe that their reliance on functional limitation rather than medical diagnosis moves them closer than other disability-related programs to a social model of disability contemplated by the UN Convention on the Rights of Persons with Disabilities.
Finally, in respect of the principle of equity, the Committee continues to support the refundability of the DTC. It is unfair, in our view, that only middle- and higher-income Canadians are able to benefit from this tax provision. It would be essential to ensure, however, that a refundable DTC would be treated as exempt income by provincial/territorial social assistance programs.
On October 18, 2022, the federal bill responsible for the Canada Disability Benefit (Bill C-22) passed Second Reading in the House of Commons.
Part 4: Indigenous Issues
Key Concerns
The Committee’s second annual report described the many concerns that Indigenous Peoples have identified over the years regarding the DTC and the income tax system, more generally. These issues are summarized below.
There is low awareness of the DTC and other tax measures. Many Indigenous Peoples living with a disability as well as service and support providers in those communities are not aware of the DTC or that it is a gateway to other benefits to which they may be entitled. Others do not believe they are eligible or that they will benefit due to their tax-exempt First Nation Status.
Even when applicants believe they may qualify for the DTC, its complex eligibility criteria create major, and often insurmountable, barriers. For example, the need to verify that a disability impairs functioning 90% of the time (the CRA’s interpretation of all or substantially all of the time) is a very high bar.
Limited access to health providers is another major barrier. It can be difficult to access a recognized health provider to complete the DTC application Form T2201. As is the case for any person living in a rural or remote community, health providers typically visit only sporadically. Because of their intermittent contact, health providers completing the Form T2201 often have limited knowledge of or relationship with the applicant.
The fees that health providers may charge for completing the Form T2201 are another significant burden. Persons living in poverty or in remote communities generally do not have access to transportation or the funds to pay for the travel to see a health provider who can complete the form or pay for the form completion itself.
Assessment challenges often arise because many Indigenous Peoples living with a disability have not been formally assessed as a youth within or outside of the school system. They subsequently transition into adult services where there is typically no funding for this purpose. As a result, the disability of these individuals may never have been properly evaluated or the assessor may lack social and cultural appreciation of the applicant. Indeed, many Indigenous cultures do not have a word for disability, a cultural difference not readily understood by health providers, administrators, or governments.
Adults experience even more assessment challenges. They face all the above barriers for assessments required for DTC eligibility combined with the fact that there is no federal funding for services for adults as there is for youth through the Jordan's Principle.
Jordan’s Principle was named in memory of Jordan River Anderson. Its purpose is to guarantee that all First nations children, regardless of their place of residence or condition, have access to the services they require to support their development and meet their needs.
It is important to note that these concerns regarding the income tax system are embedded in a broader context. Indigenous Peoples continue to experience systemic discrimination, racism, and the social and economic impact of programs and services that are seen by many as an extension of colonization.
Moreover, priorities related to poverty, harmful relationships, poor housing conditions, community political and family dynamics, health issues, lack of employment and limited communications have made the DTC less of a priority than these other pressing concerns.
DAC Recommendations
In response to these and other issues discussed in our second annual report, the Committee made several recommendations:
That the CRA develop an educational program for leaders, employees and committees in relation to Indigenous Peoples, Indigenous disability issues, funding and government initiatives to promote a better understanding of Indigenous systems in Canada and how the CRA and DTC interact with them.
That the CRA seek financial authority and obtain funding to support community organizations with strong ties to Indigenous Peoples, to engage and assist individuals and communities in their efforts to understand and apply for the DTC and other benefits, once DTC eligibility has been confirmed.
That the CRA develop an assessment package, similar to the one used for the Canada Pension Plan application for disability benefits, which speaks to Indigenous Peoples and can be:
- completed by the individual or an assessor, which considers how a person’s disability affects them “all, or substantially all, of the time” or an “inordinate amount of time”
- confirmed by a designated health care provider and attached to the main application
That the CRA, in consultation with Indigenous Peoples and disability organizations, develop mechanisms for collecting data related to age, gender, type of disability similar to other DTC databases, while respecting the confidentiality of the individual and community. Any new DTC application form should include an option for applicants to identify as Indigenous, Métis, Inuit or member of a First Nation (status or non-status).
Ongoing Work
To follow up on our earlier work, the Committee struck an Indigenous Issues Task Group to identify priority actions, discussed below.
i. Appreciation of Indigenous culture
The Task Group acknowledged that any work in this area must begin with a deep respect for and appreciation of Indigenous culture and practices. Members suggested ways in which the Committee itself could be more respectful of Indigenous practices, including land acknowledgment and appreciation of traditions, such as the role of Knowledge Keepers.
In terms of Knowledge Keepers, Indigenous communities recognize Elders for their cultural knowledge and wisdom. There are also Indigenous Knowledge Keepers who may not yet be known as “Elders” but who nonetheless are recognized for their expertise in carrying traditional teachings and practices. This group includes cultural practitioners, and teachers of song, dance, stories, art and environmental stewardship. The CRA is working with an Indigenous Knowledge Keeper to ensure that its practices remain sensitive and respectful.
When asking a Knowledge Keeper to engage in any work or consultation, it is appropriate to offer a gift to open a contract for the exchange of information. The Knowledge Keeper should also be compensated for knowledge provided to the government from which it will benefit.
The CRA has implemented several initiatives to improve awareness of barriers faced by Indigenous Peoples. Indigenous staff have been hired and CRA staff have received cultural sensitivity training.
More work must be done in this area, particularly to ensure that CRA staff answering public calls be sensitive to how they respond to inquiries from Indigenous Peoples. In 2019, the CRA opened three Northern Service Centres in Yellowknife, Iqaluit and Whitehorse in order to improve services in the Territories. Staff who field phone calls from area codes in the North have received special training.
The CRA plans to hire Indigenous Navigators to complement the services provided by the CRA Navigators who assist DTC applicants with complex cases. This role was discussed in the first section of this report on Achievements to Date.
The Committee was pleased to hear about these developments. In our second annual report, we noted the relatively low numbers of DTC applications and approvals from the North. We flagged this finding as a concern, given Statistics Canada’s figures we presented in that report on the relatively high rate of disability among Indigenous Peoples.
ii. Awareness of tax measures
The CRA has undertaken several initiatives to improve awareness of tax measures. This work is important given that the tax system not only reduces income taxes but also delivers several substantial income benefits. The Canada Child Benefit (CCB) is the prime example of a significant tax-delivered income benefit.
The CCB is worth thousands of dollars a year to low- and modest-income families with children. Households qualify for the benefit based on their family net income as declared on their income tax return. A public service campaign helped explain that despite having tax-exempt status or having little or no income, these families are eligible for the CCB if they file their income tax return.
In 2018, Service Canada and the CRA collaborated on a CCB journey map project to identify challenges in CCB eligibility and opportunities for greater uptake. A streamlined income tax form and CCB application subsequently was piloted in 2019, and expanded to include all First Nations communities in 2020. Eligibility was further expanded for the 2021 tax year to apply to all Indigenous Peoples, including Inuit and Métis.
A committee consisting of representatives from various CRA branches has been set up to tackle challenges linked to low tax awareness and limited access to various tax measures. The CRA is working with Indigenous Services Canada and the Indigenous Services Branch at Employment and Social Development Canada on a tool to encourage Indigenous Peoples to file their tax returns. In fact, the Benefits Finder was designed to help all Canadians receive the benefits for which they may be eligible.
The Task Group on Indigenous Issues found out about a helpful booklet entitled Get Your Benefits! It is a plain language publication developed by a Manitoba-based coalition of health care providers, researchers, community agencies and not-for-profit organizations. Ensuring access to relevant programs and benefits was considered an important intermediary step in reducing poverty. The Task Group suggested that this booklet would be a good model for a similar federal publication.
iii. Co-design and co-production
Beyond concerns related to awareness and sensitivity, Task Group members emphasized the need to ensure that representatives of Indigenous Peoples are actively engaged in the co-design, implementation and delivery of programs and services intended for their benefit. It is essential for the CRA and the federal government, more generally, to adhere to the “nothing without us” principle in moving toward the decolonization of the country.
It should be noted that efforts are under way throughout the federal government to engage more Indigenous Peoples in this process and move toward the Indigenization of many of its procedures.
iv. Outreach
The Task Group has urged the CRA to broaden and deepen its partnerships with local Indigenous organizations to ensure the development of culturally sensitive approaches tailored to the needs of individual communities. Outreach efforts should include information not only about the DTC but also about other disability benefits and programs that require DTC eligibility.
As a preliminary action, the CRA posted a factsheet on benefits and credits for Indigenous Peoples and associated graphics on Canada.ca (see Appendix J). Our Committee is aware of the many outreach efforts that the CRA is spearheading through its Community Volunteer Income Tax Program (CVITP). The program supports community organizations across Canada to host free tax clinics in which volunteers fill in income tax returns for eligible individuals who have modest income and relatively straightforward tax circumstances.
Wherever possible, the CRA outreach representatives should be of Indigenous ancestry or have completed cultural safety training through First Nations communities and urban services. Specially trained outreach workers would be in the best position to inform individuals and health providers about the DTC and how to complete an application that responds to the CRA’s interpretation of “all or substantially all of the time.”
Our Committee had noted in the past that nurse practitioners often work with Indigenous Peoples, particularly in Northern and remote communities. The CRA can also target this group of health providers to inform Indigenous Peoples about the DTC and other DTC-linked benefits and to assist with the completion of Form T2201.
The CRA advised our Committee that it has been involved in several partnerships with Indigenous organizations and other federal departments. The Financial Consumer Agency of Canada pilot project will provide information for an in-class curriculum intended for Indigenous Peoples. The CRA also worked with the Aboriginal Financial Officers Association (AFOA) of Canada on the podcast series: Money Smarts – AFOA Canada Talks Indigenous Financial Wellness with the Experts.
A nationally broadcast webinar for Indigenous Peoples and associated organizations was hosted by the CRA in March 2022. Its purpose was to provide information on benefits and credits, Northern resident deductions, tax-exempt income, a simplified tax and benefit package for Indigenous Peoples, the CVITP and the new Northern Service Centres.
The Committee has proposed that the CRA present regular reports on its activities regarding Indigenous issues. These reports will help update members on ongoing developments and provide opportunities for feedback and additional recommendations.
We recently were informed of the CRA’s plan to reorganize its internal operations, including the creation of a Disability, Indigenous, and Benefits Outreach Services Directorate. This separate directorate will be in a position to devote more time and attention to populations that have largely been excluded in the past from the benefits and tax reductions provided through the income tax system.
v. DTC eligibility and costs
As noted, limited access to qualified health providers is a serious concern in remote communities and the North. There are often high costs involved in travelling to see a health provider eligible to complete the Form T2201. Many health providers have no established relationship with the applicant and complete the form with relatively little knowledge of that person.
Our Committee has been considering other possible options for assessing DTC eligibility for Indigenous Peoples, in particular. We have raised the question of whether designated individuals who are widely recognized in the community, such as early childhood educators, teachers and local healers, could be included as qualified health practitioners for the purposes of completing the DTC application. This is an area that requires further exploration.
As for the cost of completing the Form T2201, the Indigenous Issues Task Group reached out to federal officials responsible for the administration of the Jordan’s Principle to ensure that DTC applicants are aware of the available financial assistance. Because this measure covers the cost of applying for the DTC on behalf of children and young adults, it is essential to ensure that Indigenous communities know about this provision.
Jordan’s Principle addresses all Indigenous Peoples, Métis, Inuit and First Nations children in Canada up to age 18 years, regardless of where they live. This is a child-first and needs-based policy principle to ensure that First Nations children living on and off reserve have equitable access to all government-funded public services. In order to ensure substantive equality, these can include services not ordinarily available to other children. In Quebec, persons under age 21 who are studying full-time at the high school level (e.g., adult education, vocational school diploma) may also be eligible.
This measure pays for the cost for health, social and education to meet the needs that current programs do not meet. Services that are covered include but are not limited to:
- screening assessments and tests (e.g., ADHD, autism, Fetal Alcohol Spectrum Disorder)
- professional services (e.g., speech therapy, physiotherapy, occupational therapy)
- mental health services
- transportation to the appointment location or specialized school transportation
- medical supplies and related equipment
- long-term care for children with special needs, including respite and home assistance
- special education services
- teacher or tutoring assistants
vi. Information and data
In our second annual report, the Committee pointed out the need for data regarding DTC claims by Indigenous Peoples. The collection and analysis of DTC data represent important ways to track decisions with respect to DTC eligibility. The data and trends over time help identify ‘red flags’ in terms of disproportionately low rates of eligibility in certain regions or for selected conditions, age groups or populations.
We acknowledged that any data collection efforts related to Indigenous Peoples must be subject to the OCAP® principles of ownership, control, access and possession. OCAP® asserts that First Nations have control over data collection processes in their communities, and that they own and control how this information can be used.
The challenge arises from the fact that the DTC figures are tabulated according to information reported on the Form T2201. At the current time, that form does not include any questions related to ethnicity or Indigeneity.
The Committee’s Data Task Group proposed that the DTC electronic application include questions related to Indigeneity. It suggested that this approach be tested for a limited time to identify any potential challenges, such as confidentiality problems linked to small sample size. The collection of this information would be carried out within the OCAP® framework.
Part 5: DTC Data
In our second annual report, the Committee included a detailed analysis of the data that the CRA had provided on the DTC. We were pleased to receive this information because it enabled us to create a profile of DTC beneficiaries and to assess trends in the caseload composition over time.
The analysis summarized the many important points we learned about the DTC. Some of the findings came as no surprise. We had expected them, based on what we had heard from the voices of lived experience, a health provider survey that our Committee had conducted in the first year of our mandate, and many disability-related reports.
We already knew, for example, that applicants with impairment in mental functions faced serious barriers in accessing the DTC. The numbers regarding approvals for physical functions compared to approvals for mental functions provided confirmation.
Other results, such as the age composition of the DTC caseload, came as a surprise. A breakdown of the caseload by age group found that 43.7% of DTC beneficiaries were aged 65 older in 2019 (latest available data). Applicants under the age of 18 made up another substantial group, at 16.9% in that year. Canadians between the ages of 18 and 64 comprised only 39.4% of the total DTC caseload.
Prior to analyzing the data, we were not aware of the fact that the DTC uptake was relatively low in Quebec as well as in all three Territories. We also questioned why such a large proportion of applications related to life-sustaining therapy were approved on a temporary basis only. Presumably, life-sustaining therapy is required for the duration of a person’s life.
Our recent conversations on these and other findings identified several additional areas that merit further exploration. There appear to be more ways to analyze the data through cross-tabulation and other combinations of variables.
To continue the conversation on these issues, the Committee struck a Data Task Group. Its members suggested that the CRA provide the list of variables that it currently collects so that other possible combinations of data could be considered. For example, the Committee had recommended a table combining age, province/territory and restriction (the CRA agreed to this) and a table combining province/territory, restriction and duration.
At the same time, the Task Group acknowledged the need to narrow the scope of future inquiry, given that the resources to collect and analyze data are somewhat limited. We realized that our main challenge was to determine what the Committee really needs to know.
The Task Group decided to prioritize the wide-ranging scope of possible data issues into the following key areas, which should continue to be addressed in future.
i. Mental functions
The DTC numbers on physical functions are broken down into several categories. Mental functions, by contrast, are clustered together into a single large group. This is not surprising, given that the numbers follow the way in which the various functions are listed on Form T2201 – and, in fact, in the Income Tax Act.
However, given the ongoing eligibility problems related to mental functions, we thought it would be instructive to have more information about this particular category. Would it be possible, for example, to disaggregate impairment in cognitive functions from impairment in other mental functions?
This information would help determine, for instance, whether individuals with impairment in mental function related to emotional challenges appear to face more challenges in accessing the DTC than those with impairment in cognitive function. The former may experience higher rates of DTC rejection and/or temporary approvals. We just don’t know.
The new DTC electronic application may help address this data gap. The application allows for the inclusion of drop-down menus in order to provide explanatory information, which ideally will make Form T2201 easier to complete. It can incorporate categories, such as the following:
- executive functioning skills such as planning, problem-solving, working memory, orientation to time and space and learning rules
- mood and emotional regulation, attention and impulsivity, and initiating, inhibiting and terminating actions
Health providers can be asked to indicate the specific areas that apply to the applicant. The information can then be collected and analyzed to determine patterns and trends regarding impairment in mental functions. This profile can be developed over time as the electronic application itself evolves with ongoing testing and associated amendments.
ii. Regional variations
Our initial analysis of the DTC data calculated the number of approvals as a percentage of the population of each jurisdiction. It is difficult to know what the figures on any given chart truly represent unless they are presented as a proportion of a baseline amount. The analysis of comparisons or percentages tell a far more complete story.
In fact, the Committee had proposed in our second annual report that DTC data should always be produced in both actual numbers and in percentage terms. Without percentages, it is difficult to highlight specific problems and to identify trends over time.
As noted, we were surprised by the results of the initial analysis, which found lower rates of DTC approval in Quebec and strikingly low rates of DTC approval in the North. We also pointed out regional variations, such as the higher rate of temporary approvals in the Atlantic region compared to the higher rate of permanent approvals in Quebec. The Committee wondered whether some of the differences in approval rates represented regional variations in training – though the CRA has indicated that staff training is fairly standard across the country.
Questions regarding lower DTC approvals from Quebec remain unanswered. Because that jurisdiction has its own disability tax credit, we wondered whether prospective applicants are unaware of the federal tax measure. Alternatively, it is possible that the time and cost involved in completing two separate applications for a disability tax credit may be a barrier for some individuals. Ideally, approval for the Quebec disability tax credit should create automatic eligibility for the federal DTC.
We learned recently that Employment and Social Development Canada (ESDC) has funded a Quebec-based study to determine why this is the case. The results of this study will be important for DTC communication and outreach in future.
The Committee was pleased to learn that the CRA has introduced DTC-related call centres in its Northern offices. We also hope that the numbers of applications and approvals will increase as a result of expanded outreach to Indigenous communities, described in the section on Indigenous Issues.
iii. Caseload composition
As noted, the Committee had not appreciated that DTC beneficiaries aged 65 and over comprised such a significant proportion of the DTC caseload. We wondered whether it would be possible to determine how many of these beneficiaries are new applicants and how many current DTC recipients who are aging into the 65-plus category.
We also acknowledge, however, that the relatively high numbers for this age group are not surprising. Many individuals experience some form of visual, hearing, mobility and/or cognitive impairment as they age.
Committee members questioned whether the DTC was the best way to offset the costs associated with the needs of this age group. We discussed other possible options, including an increase in the value of the age tax credit or a new program to enable access to disability supports. We acknowledged that these options could have potentially higher costs than the current arrangement.
iv. Temporary and indeterminate approvals
Committee members were surprised to see such a large proportion of temporary approvals for individuals who applied under the life-sustaining therapy category. The need for life-sustaining therapy implies a permanent condition.
It would be helpful to have a better understanding of the criteria employed for temporary and indeterminate approvals by age, by function and for life-sustaining therapy. It is possible that the CRA expects that the development of new technologies may, in future, require much less time and effort than is currently the case. We believe that it is important to understand the basis on which these decisions are made.
v. Data as quality improvement tool
DTC data should be tracked on an ongoing basis in order to identify trends and monitor the impact of new CRA policies and procedures. The most recent DTC figures are attached as Appendix K. The data can be used for continual quality improvement in DTC determinations.
As soon as we received the initial data, the Committee produced an extensive analysis of these numbers. We propose that the CRA continue to carry out these analyses in future. It should also continually look for “red flags” or concerns that the data may have raised.
Other issues
In our second annual report, the Committee questioned the need to maintain marital status as a key variable. We were not sure that this information contributed substantively to the analysis.
However, Data Task Group members felt that it would be important to maintain marital status and not drop it as the DAC had earlier proposed. If one spouse does not have enough income, claiming the DTC would not reduce their tax payable. However, if the other spouse’s income is high enough, they could claim it on the other’s behalf and thereby reduce the tax payable.
The DTC Task Group also raised several questions that are not necessarily captured in the DTC numbers but that are nonetheless important. How can we learn more, for example, about the experience of DTC recipients? What assistive devices and services do they currently use or need? What is their ecosystem of support?
Because these questions cannot be answered through the information currently available on Form T2201, they would need to be addressed through some other data collection methodology. It may be appropriate to add a few questions of this nature to the Client Experience Survey conducted on a regular basis by the CRA.
It is also important to obtain data on who is not being accepted for the DTC and why. Again, it may be necessary to set up a separate survey process for addressing this issue.
The Data Task Group also noted that DTC expenditures went down in 2019 despite a higher DTC caseload. We wondered whether this information could mean that more individuals were applying for the DTC in order to gain access to other disability benefits and programs rather than as a credit to reduce their income taxes.
We posed this question because it has always been difficult to get a sense of how significant the DTC gateway role has been relative to its tax reduction role. It is not possible to determine at this time whether its vital gateway function is well understood or utilized by potentially eligible individuals. The Committee has long identified the need for ongoing and improved communication around the dual DTC role.
Finally, our second annual report had proposed the collection of DTC data on Indigenous Peoples. We discuss this work in the section on Indigenous Issues.
Part 6: Registered Disability Savings Plans
The Committee’s two previous annual reports explained the importance of Registered Disability Savings Plans (RDSPs) and discussed the many concerns that had been brought to our attention. In this report, we highlight some new issues related to this important program.
As we have noted in the past, a key challenge arises from the fact that the CRA is responsible for only a certain component of the RDSP. Three federal departments actually play a role in the design and administration of this measure:
- the Department of Finance Canada develops the overall policy parameters, which are set out in the Income Tax Act
- the CRA is responsible for the administration of the Income Tax Act. Its role includes approving RDSP plans, authorizing financial institutions to offer RDSPs and registering plans
- Employment and Social Development Canada administers the Canada disability savings grant and Canada disability savings bond, described below. It also conducts outreach to improve awareness and the uptake of these measures.
Financial institutions, known as RDSP issuers, are responsible for the day-to-day administration of individual RDSPs.
What is an RDSP?
An RDSP is a savings plan whose purpose is to help people with disabilities save for their long-term financial security. Applicants must first qualify for the DTC in order to open an RDSP.
For children under the age of majority, a parent or legal guardian/public department/agency/ institution that is legally authorized to act for the child can be the holder of their RDSP. When the child reaches the age of majority, the parent can continue to be the holder of the RDSP, transfer the role to the beneficiary or become joint plan holders with the beneficiary if the financial institution allows for joint holders.
For adult beneficiaries who are unable to be the RDSP plan holder because they cannot enter into a contract due to capacity concerns, only a parent, spouse or common-law partner, or other person or institution that is legally authorized to act on behalf of the individual can be the plan holder.
Contributions to an RDSP are not tax deductible and can be made until the end of the year in which the beneficiary turns 59. Contributions that are withdrawn are not included as income to the beneficiary when these are paid out of an RDSP. However, the Canada disability savings grant (grant), Canada disability savings bond (bond), investment income earned in the plan and proceeds from rollovers are included in the beneficiary’s income for tax purposes when these amounts are paid out of the RDSP.
The grant is an amount that the federal government pays into an RDSP. The federal government provides a matching grant of 300%, 200% or 100%, depending on the beneficiary’s adjusted family net income and the amount contributed. A beneficiary can be eligible for up to $3,500 in grants annually. Due to a carry-forward provision, up to $10,500 can be paid into the beneficiary’s RDSP in a given year. A total of $70,000 in grants can be paid into the RDSP over the beneficiary’s lifetime. A grant on contributions can be made until December 31 of the year in which the beneficiary turns 49.
The bond is an amount paid by the federal government into the RDSPs of beneficiaries with low and modest incomes. Depending upon family income, a beneficiary may be eligible for a bond of up to $1,000 annually. With the carry-forward provision, up to $11,000 in bonds can be paid into a beneficiary’s RDSP in a given year. The lifetime bond limit is $20,000. A bond can be paid into an RDSP if an application is made on or before the end of the year in which the beneficiary turns 49.
Links to DTC eligibility
An applicant who wishes to open an RDSP must first qualify for the DTC. A person who is deemed ineligible for the DTC is not permitted to open an RDSP account and does not have access to Canada disability savings grants and bonds.
Several years ago, Canadians and organizations representing persons with disabilities brought to our attention a serious concern related to the DTC gateway function. When applicants are accepted for the DTC, a decision is made about the duration of their eligibility. If they are approved for a temporary period only, they must file another application in order to continue qualifying for the DTC.
Our first annual report highlighted how problems can arise for beneficiaries who have already opened an RDSP account and are later deemed ineligible for the DTC. All or part of the grants and bonds that had been in the RDSP for fewer than 10 years had to be repaid to the federal government. The Committee pointed out that the loss of the DTC can be financially catastrophic for those individuals.
We were particularly concerned about persons with lifelong conditions that involve severe and prolonged impairment in physical and/or mental functions. If their functional capacity changes or improves as a result of a new medication or technical aid to the point where they are no longer markedly restricted, they are not eligible for the DTC. If their condition deteriorates, however, they may have difficulty re-establishing their DTC eligibility. In the meantime, they lost the only funds they had been able to save for future needs.
The Committee argued that individuals who received a federal benefit for which they were deemed eligible, in this case an RDSP grant and/or bond, should be able to keep those funds. We were pleased with the 2019 Budget announcement to eliminate the requirement to close an RDSP when an individual no longer qualifies for the DTC. The RDSP can now remain open and account holders do not have to return the invested amounts if they no longer qualify for the DTC.
It remains unclear, however, whether the RDSP grant and bond portions for which an RDSP holder might have been eligible will be paid retroactively. Committee members have requested, but have still not received, clarification on this question. We recommended:
That in light of the positive decision to eliminate the requirement to close an RDSP when a beneficiary no longer qualifies for the DTC, the federal government should pay retroactively the RDSP grant and bond portions for which an RDSP holder would have been eligible.
New issues
Our first two annual reports identified a range of RDSP-related concerns. The long list included the fact that RDSP rules should be simplified. They are so complex that there is often confusion about the rules even among the banks and financial institutions that administer these savings instruments.
Persons with an intellectual impairment or developmental disability must often subject themselves to guardianship before they can open an RDSP. This requirement has implications for other aspects of their lives. This issue is discussed more fully below.
There is a need for a national solution or pan-Canadian supported decision-making approach to banking. There likely are similar concerns regarding people with dementia and other related conditions. Who oversees the appropriate use of funds on behalf of the individual?
If an RDSP has been opened by parents and they die, the status of the RDSP is unclear. There are questions as to what the financial institutions do with these accounts if the beneficiary is deemed not contractually competent to manage the plan. Do they require a legally authorized financial representative to act on the person’s behalf?
In order to address these wide-ranging and emerging concerns, the Committee has urged the federal government to create an advisory table that would report to all three federal departments involved in the RDSP program. As noted, the CRA alone cannot make all the changes that are required to improve this program.
In our second annual report, we recommended:
That the federal government set up an advisory body, consisting of RDSP applicants and account holders, to resolve long-standing concerns and to address emerging issues with respect to the RDSP and its interface with the DTC. To help tackle complex issues such as legal capacity, the advisory body should include or consult regularly with selected organizations representing persons with disabilities.
The Committee has not, to date, received any response to this recommendation. We want to stress once again its importance. The RDSP has now reached maturity for many of the early contributors who opened accounts shortly after the program was introduced in 2008. Fifteen years later, it is essential that the federal government address the many challenges related to this program.
In the absence of an advisory body to review these issues, our Committee struck a Task Group to continue the RDSP conversation. The group produced a report, which discusses key legal challenges related to the DTC (see Appendix H). One of the major concerns is described below.
Legal authorization for opening an RDSP
The Income Tax Act sets out a definition of qualifying person in relation to an RDSP beneficiary. Qualifying family members can open, manage and make contributions to the RDSP on behalf of a person with an impairment in cognitive mental function. However, the current definition is not actually a form of supported decision-making and is a temporary measure, which is set to expire in December 2023.
Many family members are caught in a bind. On the one hand, they seek to ensure the future financial security of their relative. At the same, they end up restricting a person’s basic human rights when they need to formally place that individual under a substitute decision-making or guardianship order.
In fact, some families have decided to forego their own financial security so that their family member can retain more independence over their own lives. The family simply has made a decision not to open an RDSP.
This means that the intrusive RDSP eligibility criteria effectively exclude a substantial proportion of the population for whom this benefit is intended. Each year, a cohort of potential beneficiaries age out of eligibility for RDSP, potentially losing up to $90,000 in federal contributions.
Moreover, the competency requirement for RDSP beneficiaries contravenes the United Nations Convention on the Rights of Persons with Disabilities. Under Article 12, Canada agreed to recognize that persons with disabilities enjoy legal capacity on an equal basis with others in all aspects of life and to ensure that they can access support to exercise legal capacity.
Finally, individual financial security may be jeopardized when an RDSP plan holder, such as a parent, passes away and there is no other qualifying family member. Should this happen, the person would need to have a guardian appointed or leave their RDSP unmanaged indefinitely.
The federal government can address this set of related problems by extending beyond 2023, and then making permanent, the temporary measure in the Income Tax Act. The list of persons eligible to act as qualified family members can also be expanded to include any trusted friend or family member who is likely to survive the beneficiary’s parents. The proposed changes would mean that the contractual capacity requirement would no longer be a barrier to opening an RDSP.
The Committee recommends:
That the federal government:
- extend the temporary inclusion of “qualified family member” in the definition of “qualifying person” in s. 146.4(1) of the Income Tax Act beyond 2023 and broaden the list of persons defined as “qualified family members” to include siblings
- make the above-stated temporary measures permanent – i.e., all references to “qualified family members” in s. 146.4(1) of the Income Tax Act
- exercise its Peace, Order and Good Government power to create a national minimum-standard legislative framework to ensure that Canadians with disabilities are able to access the benefits of the RDSP through supported decision-making, regardless of the type or degree of their disability or their province or territory of residence
Next Steps
In addition to complex rules, it has come to our attention that there is low awareness among Canadians about the RDSP. There is a need for outreach and communication about this vital program.
At the same time, the RDSP legal and administrative apparatus needs a long-awaited overhaul. Fifteen years is a long time for a program to operate with no advisory body or built-in review.
All three federal departments responsible for the RDSP program need to work together on a suite of required reforms. Persons with disabilities should not be put in the position of having to choose between attaining financial security and retaining some measure of autonomy. Neither should their families face untenable requirements that compromise the independence and dignity of the individual.
Appendices
Appendix A: Disability Advisory Committee Terms of Reference
1. Mission statement
- To advise the Canada Revenue Agency (CRA) on interpreting and administering tax measures for Canadians living with disabilities in a fair, transparent and accessible way.
2. Mandate of the Committee
- To provide advice to the Minister of National Revenue and the Commissioner of the CRA on the administration and interpretation of laws and programs for disability-related tax measures administered by the CRA;
- To provide advice on how the needs and expectations of the disability community can be considered by the CRA as they interpret and administer disability-related tax measures. This may involve recommendations for information gathering and collaboration between the CRA and the disability community;
- To provide advice on how the CRA can increase:
- Overall awareness of tax measures for persons with disabilities; and
- Take-up of tax measures for persons with disabilities.
- To provide advice on how the CRA can best:
- engage persons with disabilities and their support communities; and
- deliver information, education and outreach initiatives about disability-related tax measures and important administrative changes to:
- persons with disabilities;
- those who support persons with disabilities;
- professionals who advise persons with disabilities;
- health practitioners; and
- not-for-profit agencies and various levels of government;
- To review and make recommendations for improvement to the CRA’s administrative practices in order to enhance the quality of the services and products the CRA provides to persons with disabilities;
- To provide the CRA with a formalized means of consulting with various stakeholders; and
- While legislative change is beyond the mandate of the Disability Advisory Committee and the role of the CRA, recommendations for legislative change to disability tax measures may be made by the Committee for consideration and will be forwarded to the Department of Finance Canada.
3. Composition
Membership on the Committee will be determined on the following basis:
- The Committee consists of a blend of service providers (e.g. health, tax professionals, lawyers, accountants), advocates of the disability community and persons with disabilities;
- The Committee will be composed of 12 members and 2 co-chairs, appointed for a term not to exceed 48 months (starting with the first meeting of their appointment);
- One of the Committee members will act as vice-chair, to support the private sector co-chair and provide activities at the discretion of co-chairs such as;
- help setting the agenda for the in-person meetings; and
- participate in discussions with co-chairs as to the progress of the Committee and the work that needs to be undertaken.
- The Minister and the Commissioner appoint the members and determine the length of their terms;
- In order to have some continuity of membership, during the first four years of the Committee, the members will be given different terms:
- Four (4) members will be appointed for 48 months;
- Four (4) members will be appointed for 36 months; and
- Four (4) members will be appointed for 24 months.
- Thereafter, members will be appointed for terms of 36 months.
- Should a member not be able to serve his or her full term of appointment, the Minister jointly with the Commissioner will then appoint a suitable individual to complete the remaining portion of the term of appointment created by that vacancy;
- Membership is voluntary and members will not be paid to attend meetings. However, reasonable travel and accommodation expenses to attend meetings will be reimbursed according to the CRA Travel Policy, and meetings will be held in accordance with section 9 (below); and
- Other federal departmental representatives (e.g. Department of Finance Canada, Employment and Social Development Canada) may be welcomed in the role of observers or resource people.
4. Role of Committee members
- The roles and responsibilities of Committee members include:
- Awareness of the needs and experiences of persons with disabilities to inform the Committee’s deliberations and recommendations to the CRA on its disability-related tax measures;
- Identifying topics for consideration or presentation to the CRA;
- Offering advice, comments and recommendations on CRA services, products, and administrative policies and other issues and initiatives that are presented to the Committee;
- Undertaking activities to inform its advice and recommendations to the CRA such as mechanisms for stake-holder engagement and collaboration (e.g. surveys, focus groups);
- Committee members have been selected to represent the views of their respective communities and associations. The members agree not to use the Committee as a means to advance their own personal interests or further the sole interests of the associations they represent;
- Committee members agree not to act as advocates to address the tax situations of specific taxpayers or to raise cases with the Committee that are before the courts; and
- Committee members are expected to participate in a collaborative and constructive manner that promotes tangible outcomes and upholds public confidence in the Committee’s mandate, advice, and recommendations. Members are asked to address any individual concerns through dialogue with the co-chairs and, as appropriate, the Committee as a whole.
- Committee members are not spokespersons for the CRA. Each member is a stakeholder, representing themselves as an expert or as an advocate of persons with disabilities;
- Any information developed in consultation with other groups or shared by Committee members will become part of the formal and public proceedings of the Committee upon consensus of the Committee; and
- Members may discuss consultative initiatives of the Committee with their communities and colleagues unless expressly advised that they should not do so for reasons of confidentiality.
5. Establishment of co-chairs
- The Assistant Commissioner, Assessment & Benefit Services Branch (ABSB) of the CRA, will serve as co-chair of the Committee alongside a co-chair from the private sector;
- The private sector co-chair must be a Committee member;
- The term of a private sector co-chair will be twenty-four months (starting with the first meeting of his/her appointment);
- After the initial appointment of a private sector co-chair by the Minister and the Commissioner for 24 months, the private sector co-chair can be renewed by the Minister and the Commissioner for a subsequent term of twenty-four months, or a new private sector co-chair can be appointed by the Minister and the Commissioner;
- Members of the Committee can be eligible for appointment as co-chair after serving a term of 24 months or more;
- Should the private sector co-chair not be able to serve his or her full term of appointment, an appointment will take place according to 5. b), c) d) and e); and
- The outgoing co-chair will have the opportunity to remain a member of the Committee for an additional 12 months to ensure continuity between the co-chairs. This could mean that the Committee will be composed of 13 members on some occasions.
6. Roles of co-chairs
- Ensure that the Committee adheres to its mandate and the members fulfill their roles;
- Develop meeting agendas in concert with the Committee’s mandate and roles;
- Facilitate meetings and lead the discussions, including during video or teleconferences;
- Ensure that all members are heard, engaged and respected in the work of the Committee;
- Report on the progress made by the Committee to the Minister and the Commissioner; and
- Serve as spokespersons for the Committee.
7. Responsibilities of the co-chair from the CRA
- To be the liaison between CRA and the Committee; and
- To provide secretariat services to the Committee which includes, but is not limited to providing the Committee with data necessary to informing their work and any recommendations such as:
- how the CRA currently liaises with disability stakeholder groups;
- how the CRA handles inquiries regarding disability;
- processes the CRA uses to decide on DTC eligibility;
- requirements of persons to maintain their DTC eligibility;
- rates of acceptance and rejection by activity; and
- appeal processes and data.
8. Responsibilities of the co-chair from the Committee
- To be the liaison between the 12 members of the Committee and the CRA in its secretariat function;
- To represent the views of the Committee as a whole; and
- To guide the Committee in its advisory function.
9. Meetings
- Upon initial formation, the Committee will meet three times per year. The frequency of meetings will be periodically re-examined to ensure best use of Committee members’ time;
- The meetings will be held in Ottawa at location(s) that are accessible to those participants who are persons with disabilities. Other methods of meeting may also be utilized in order to keep costs at a reasonable level, such as videoconferences, teleconferences or on-line consultation in lieu of face-to-face meetings, in accordance with section 3. g); and
- In order for a meeting to take place, a quorum is necessary and will be met when a minimum of 7 members are in attendance.
10. Topics of discussion
- The co-chairs are responsible for setting meeting agendas in consultation with Committee members. Any member of the Committee can submit relevant topics for discussion to the co-chairs;
- An agenda item presented for discussion or activity that is not aligned with the mandate and role of the Committee and/ or that does not meet with the consensus of the Committee will not be pursued;
- In the event of dissent arising about whether an agenda topic or activity is aligned with the mandate and role of the Committee, the co-chairs and/or the Minister and the Commissioner will have the authority to rectify the dissent;
- The Minister or the Commissioner may request the Committee discuss and analyze a specific topic; and
- The Committee can request information as defined in 7.b) necessary to informing a topic of discussion.
11. Reporting
- A record of meeting proceedings will be kept and submitted to the Minister and Commissioner as well as made publicly available;
- The Committee may report on a specific topic to the Minister and the Commissioner in the format of a letter sent to the Minister and the Commissioner indicating the summary of the findings and the recommendations of the Committee;
- In the event that the Minister or Commissioner requests the Committee to discuss and analyze a specific topic, the Committee will report on this discussion and analysis will be sent to the Minister and the Commissioner in the format of a letter indicating the summary of the findings and any attendant recommendations;
- At the end of each year (following three meetings per year), the Committee will report to the Minister and the Commissioner with a summary of all topics discussed as well as recommendations for all topics; and
- Meeting proceedings (a), specific reports (b) and annual reports (c) will be reviewed and approved upon consensus of Committee members.
The CRA will assist the Committee in ensuring that all meeting materials and Committee reports are fully accessible.
12. Secretariat
- The Committee co-chair is the Assistant Commissioner of the ABSB or as an alternate, the Director General of Benefit Programs Directorate; and
- The Assessment, Benefit, and Service Branch will provide secretariat services for the Committee, performing functions such as:
- Maintaining membership lists and coordinates of each member;
- Circulating agendas, minutes and documentation to Committee members;
- Organizing materials and all logistics for Committee meetings; and
- Supporting the co-Chairs in their roles and responsibilities communicating with the Commissioner, the Minister and other stakeholders.
Appendix B: List of Committee Members
The Committee is composed of voluntary members including persons with disabilities, health providers and professionals from a variety of fields, such as tax professionals and lawyers. The Committee is currently co-chaired by Sharon McCarry, Founder and Executive Director, La Fondation Place Coco, and by Gillian Pranke, Assistant Commissioner, Assessment, Benefit, and Service Branch, Canada Revenue Agency (CRA). Jonathan Lai serves as vice-chair.
This report came into formation under the leadership of the previous co-chairs, Dr. Karen R. Cohen, Chief Executive Officer, Canadian Psychological Association, and by Frank Vermaeten, previous Assistant Commissioner, Assessment, Benefit, and Service Branch, Canada Revenue Agency (CRA). Ms. Sherri Torjman, former co-chair of the Technical Advisory Committee (TAC) and vice-chair of the Committee, was retained on contract by the CRA to support the Committee in co-ordinating its activities and fulfilling its reporting obligations by producing this report.
The Committee’s work is independent and impartial. Mr. Vermaeten, as previous co-chair of the Committee, functioned as the liaison between the Committee and the CRA. Under Mr. Vermaeten’s leadership, the CRA assisted the Committee in its work, providing secretariat services as well as research and communications support.
The Committee members whose work produced this report are:
Dr. Karen R. Cohen, Co-Chair of the Committee, CEO, Canadian Psychological Association, residing in Ontario
Frank Vermaeten, Co-Chair of the Committee, Assistant Commissioner with the Canada Revenue Agency, residing in OntarioFootnote 1
Sherri Torjman, Vice-Chair of the Committee, former vice-president, Caledon Institute of Social Policy, residing in Ontario
Laurie Beachell, Bakerlaw, former National Coordinator Council of Canadians with Disabilities (CCD), residing in Manitoba
Gary Birch, Neil Squire Society, residing in British Columbia
Roberta Heale, Nurses Practitioner Association of Canada, residing in Ontario
Sharon McCarry, La Fondation Place Coco, residing in Quebec
Ray McGuire, British Columbia Aboriginal Network on Disability Society, residing in British Columbia (Resigned from the Committee on October 2021)
Marie Ryan, Goss Gilroy, residing in Newfoundland and Labrador (Resigned from the Committee on May 2022)
Brendon Pooran, PooranLaw Professional Corporation, residing in Ontario
Dr. Olaf Kraus de Camargo, McMaster University, residing in Ontario
Jonathan Lai, Autism Alliance of Canada, residing in Ontario
Dr. Marie-Hélène Chomienne, University of Ottawa, residing in Ontario
Janean Marshall, Educator at MI’kmaw Kina’matnewey and Saint Francis Xavier University, residing in Nova Scotia
Appendix C: Recommendations
- 1) First Annual Report Recommendations
- 2) Second Annual Report Recommendations
- 3) Third Annual Report Recommendations New
1) First Annual Report Recommendations
1
That in the determination of DTC eligibility, the Canada Revenue Agency ensure that the principle of parity guides its actions with respect to physical and mental functions including, but not limited to, the removal of multiple screens of eligibility for persons with impairment in mental functions.
2
That the Canada Revenue Agency amend the list of mental functions on Form T2201 as follows:
- attention;
- concentration;
- memory;
- judgment;
- perception of reality;
- problem solving;
- goal setting;
- regulation of behaviour and emotions
- (for example, mood disturbance or
- behavioural disorder);
- verbal and non-verbal comprehension; and
- learning.
3
That the Canada Revenue Agency replace on page 5 of Form T2201 the term “effects of the impairment” with the following:
“The effects of the individual’s impairment must restrict their activity (that is, walking, seeing, dressing, feeding, mental functions, eliminating, hearing, speaking or some combination thereof) all or substantially all of the time, even with therapy and the use of appropriate devices and medication.”
4
That the Canada Revenue Agency delete the reference to “social activities” on page 5 of Form T2201 due to the contradiction on page 3 of the form. Page 5 states that one is ineligible on the basis of social and recreational activity, while page 3 states that the inability to initiate and respond to social interactions makes one eligible, as does the inability to engage in common simple transactions.
5
That the Canada Revenue Agency change the question on page 5 of Form T2201 about the likelihood of improvement to ask health providers whether the individual’s illness or condition that is responsible for the impairment in function, such as walking or cognitive functions, is likely to improve, as in the following example:
“In thinking about the individual’s impairment, please consider whether the condition that causes the impairment (for example, blindness, paraplegia, schizophrenia or bipolar disorder) can be expected to last for a continuous period of at least 12 months.”
6
That the Canada Revenue Agency no longer interpret all or substantially all as 90% of the time and no longer interpret an inordinate amount of time as three times the amount of time it takes a person without the impairment.
7
That in the DTC assessment process, the Canada Revenue Agency employ the following definition to determine marked restriction in mental functions:
“The individual is considered markedly restricted in mental functions if, even with appropriate therapy, medication and devices (for example, memory and adaptive aids):
- all or substantially all the time, one of the following mental functions is impaired, meaning that there is an absence of a particular function or that the function takes an inordinate amount of time:
- attention;
- concentration;
- memory;
- judgment;
- perception of reality;
- problem solving;
- goal setting;
- regulation of behaviour and emotions (for example, mood disturbance or behavioural disorder);
- verbal and non-verbal comprehension; or
- learning; or
- they have an impairment in two or more of the functions listed above none of which would be considered a marked restriction all or substantially all the time individually but which, when taken together, create a marked restriction in mental functions all or substantially all the time; or
- they have one or more impairments in mental functions which are:
- intermittent; and/or
- unpredictable; and
- when present, constitute a marked restriction all or substantially all the time.”
8
That the Canada Revenue Agency remove specific references to activities in the T2201 section on mental functions and include examples of activities in the current Guide RC4064 to help health providers detail all the effects of the markedly restricted mental function(s), as in the following illustration:
“The individual is considered markedly restricted in mental functions if they have an impairment in one or more of the functions all or substantially all of the time or takes an inordinate amount of time to perform the functions, even with appropriate therapy, medication, and devices. The effects of the marked restriction in mental function(s) can include, but are not limited to, the following (this list is illustrative and not exhaustive):
- with impaired memory function, the individual cannot remember basic information or instructions such as address and phone number or recall material of importance and interest;
- with impaired perception, the individual cannot accurately interpret or react to their environment;
- with impaired learning or problem solving, the individual cannot follow directions to get from one place to another or cannot manage basic transactions like making change or getting money from a bank;
- with impaired comprehension, the individual cannot understand or follow simple requests;
- with impaired concentration, the individual cannot accomplish a range of activities necessary to living independently like paying bills or preparing meals;
- with impaired ability to regulate mood (for example, depression, anxiety) or behaviour, the individual cannot avoid the risk of harm to self and others or cannot initiate and respond to basic social interactions necessary to carrying out basic activities of everyday life; or
- with impaired judgment, the individual cannot live independently without support or supervision from others or take medication as prescribed.”
9
That the Canada Revenue Agency consider a child and an adult version of Form T2201, with eligibility criteria tailored as necessary.
10
That the Canada Revenue Agency revise the list of functions on Form T2201 to the following:
- vision;
- speaking;
- hearing;
- lower-extremity function (for example, walking);
- upper-extremity function (for example, arm and hand movement);
- eliminating;
- eating/feeding; and
- mental functions.
11
That the Canada Revenue Agency, in respect of the parity principle, create a list of examples of activities for each impaired function for inclusion in the current Guide RC4064 to help health providers detail all the effects of markedly restricted function(s), as in the following proposed guidelines (this list is illustrative and not exhaustive):
- with impaired lower-extremity function, the individual cannot walk;
- with impaired upper-extremity function, the individual cannot feed or dress themselves, or cannot attend to basic personal hygiene; or
- with impaired eating/feeding, the individual cannot swallow or eat food.
12
That the Canada Revenue Agency review the current eligibility criteria for hearing, which are out of date.
13
That the Canada Revenue Agency work in collaboration with the Department of Finance Canada to consult with relevant health providers and stakeholders before introducing any legislative changes to the Income Tax Act with respect to the definition of mental or physical functions.
14
That the Canada Revenue Agency replace the current eligibility criteria for life-sustaining therapies as set out in Form T2201 with the following:
Individuals who require life-sustaining therapies (LSTs) are eligible for the DTC because of the time required to administer these therapies. These are therapies that are lifelong and continuous, requiring close medical supervision. Without them, the individual could not survive or would face serious life-threatening challenges. Close medical supervision is defined as monitoring or visits, at least several times annually, with a health provider. These therapies include but are not necessarily limited to: intensive insulin therapy for type 1 diabetes; chest therapy for cystic fibrosis; renal dialysis for chronic and permanent renal failure; and medically prescribed formulas and foods for phenylketonuria (PKU).
15
That the Canada Revenue Agency:
- consider whether some conditions, such as a complete paraplegia or tetraplegia, schizophrenia or a permanent cognitive disorder with a MOCA below 16, should automatically qualify for the DTC in the way that blindness does. (MOCA is a mental status examination of cognitive functions used commonly to assess impairment that results from conditions such as dementia, head injury or stroke.); and
- examine the eligibility criteria employed in other federal and provincial/ territorial programs, such as the Ontario Disability Support Program and the programs for Canada Pension Plan disability benefits and, veterans disability pensions, to identify the conditions/diagnoses that establish automatic eligibility for those programs.
16
That the Canada Revenue Agency examine the new eligibility form being used for Canada Pension Plan disability benefits to identify areas in which there might be synergies regarding eligibility for the DTC, such as including the presenting condition or diagnosis as supplementary information to identifying functional limitations.
17
That the Canada Revenue Agency test or pilot various approaches that would remove the gatekeeper role from health providers. One such approach would be for community tax clinics to take on a screening or advisory function. Another would be to establish a Canada Revenue Agency call centre explicitly for this function.
18
That the client experience survey on the DTC and other disability tax measures to be carried out by the Canada Revenue Agency include a question as to whether the individual or recipient had any difficulty accessing a health provider for the purposes of completing Form T2201 and, if so, for which activity. Clients should also be invited to provide any additional comments on this question. Special attention should be paid in this survey to the needs and concerns of Indigenous Canadians.
19
That the Canada Revenue Agency develop a process for expanding the list of health providers with the appropriate expertise who can assess eligibility for the DTC.
20
That in the case of determining DTC eligibility for persons with impairment in mental functions, the Canada Revenue Agency include relevant specialized health providers, including, but not limited to, psychiatrists and psychologists, in the review process when applications are disallowed.
21
That the Canada Revenue Agency:
- copy to the applicant all clarification letters sent to the health provider;
- let the health provider know that all communication to a health provider about an applicant will be copied to the applicant and that any communication the health provider submits to Canada Revenue Agency will also be made available to the applicant;
- encourage the health provider to contact and consult the applicant as necessary when providing any clarification to the Canada Revenue Agency; and
- extend the time for a health provider to file a clarification letter with the Canada Revenue Agency from 45 to 60 days and note this timeline on the first page of the questionnaire.
22
That the Canada Revenue Agency:
- provide in notice of determination letters a relevant reason as to why a DTC application was denied;
- include in notice of determination letters a copy of the clarification letter and the health provider’s clarification response. This information is vital in case of an appeal; and
- move the consumer survey request to the bottom of the notice of determination letters.
23
That the Minister of National Revenue review the current appeals process with a view to creating a straightforward, transparent and informed process where the applicant has access to all relevant information (including the precise reason their application was denied) and documents (including copies of all information submitted by health providers that pertain to their application).
24
That the Canada Revenue Agency include a document (one-page, two-sided information sheet) entitled “Your Rights When a Notice of Determination Denies a Claim for the DTC” that would:
- explain the requirements, timelines and details for filing the following:
- review;
- notice of objection with the Appeals Branch; and
- notice of appeal with the Tax Court of Canada;
- inform taxpayers that other persons (that is, family members, friends or professional advisors) can act on their behalf by submitting Form T1013, Authorizing or Cancelling a Representative, or writing a letter;
- inform taxpayers that they have access to all documents in their files, including a copy of the follow-up questionnaire and any clarification letter completed by the health provider;
- inform taxpayers that they can contact the Canada Revenue Agency for a copy of Pamphlet, P148, Resolving your dispute: Objection and appeal rights under the Income Tax Act, if they do not have access to the Internet; and
- provide the correct contact information and mailing addresses for the submission of any required materials.
25
That the Canada Revenue Agency consult on a regular basis with selected community organizations to:
- ensure that all its communications and materials (including letters of correspondence with individuals) are easily accessible by persons with disabilities and are available in plain language. Organizations such as People First can assist with ensuring plain language; and
- determine whether its communications and materials are keeping pace with technological change and with the technologies in common use by communities of persons with disabilities.
26
That Canada Revenue Agency web content, which outlines disability tax measures, link to relevant provincial and territorial websites that identify disability-related provisions in those jurisdictions, as well as the range of federal and provincial/territorial disability measures that require DTC eligibility in order to qualify.
27
That the Canada Revenue Agency provide and make publicly available relevant data on the DTC, including number of applications, approvals, rejections, and appeals; durations of eligibility by function; and a demographic profile of current beneficiaries by age and gender.
28
That the Canada Revenue Agency provide an option for the electronic submission of Form T2201 and related materials that:
- is convenient and accessible for both taxpayers and tax preparers; and
- permits submission of those materials at the same time as, or after, the filing of an income tax and benefit return.
29
That the Canada Revenue Agency develop, in collaboration with the Disability Advisory Committee, a client experience survey that would align with the health provider survey, but be modified as appropriate to suit the needs and concerns of the target group comprising a representative sample of current and former DTC beneficiaries.
30
That the Canada Revenue Agency provide dedicated support to ensure call centre agents are accessible and have the expertise to answer enquiries related to the DTC form and eligibility.
31
That the Canada Revenue Agency, through the Community Volunteer Income Tax Program, which supports voluntary organizations to provide and train volunteers, run community tax clinics and raise awareness about the DTC. There should be a special focus on Indigenous communities.
32
That the Canada Revenue Agency revisit and restate the purpose of the DTC in order to reflect its multiple roles.
33
That the Minister of National Revenue work with the Minister of Families, Children and Social Development to ensure that individuals are able to keep all contributions they made to, and any and all grants and/or bonds they may have received for, their registered disability savings plan for periods during which they qualified for the DTC.
34
That, as a short-term measure, the federal government should ensure continued eligibility for related DTC-gateway programs, at least at the federal level, even if DTC eligibility has been revoked. This interim measure would allow for the development of secondary screening processes to determine whether individuals or households can continue to remain eligible for gateway-related services and supports.
35
That the Canada Revenue Agency, in collaboration with the Province of Quebec, determine a single eligibility process for the DTC in order to avoid separate eligibility at different levels of government.
36
That the Canada Revenue Agency cap the fee that consultants can charge to assist with an initial DTC application and act as expeditiously as possible to draft the regulations introducing this cap.
37
That the Canada Revenue Agency reimburse an applicant or provider at a reasonable rate in accordance with the provincially recommended fee for the time involved in responding to Canada Revenue Agency clarification letters in support of a DTC application or reassessment.
38
That the Minister of National Revenue work collaboratively with the Minister of Finance, Minister of Families, Children and Social Development, and the Minister of Sport and Persons with Disabilities to:
- identify ways of addressing the disproportionate poverty of Canadians with disabilities, or alternatively, that the Minister of National Revenue request the establishment of a parliamentary committee to address this issue and bring forward recommendations;
- transform, as a first step, the current DTC from a non-refundable credit into a refundable credit in order to recognize the non-itemizable costs incurred by lower-income Canadians with disabilities; and
- ensure that the poverty alleviation of Canadians with disabilities is a focus of all relevant federal-provincial/territorial ministers’ meetings and that there be no provincial/territorial clawback of any new or improved federal measures.
39
That the Canada Revenue Agency, in partnership with the Department of Finance Canada, Statistics Canada and the disability community, undertake a study of the current data needs regarding the DTC and identification of appropriate new ways of tracking needed DTC information, including the estimated number of Canadians who potentially would be eligible for the DTC but are unable to benefit because of its non-refundable status.
40
That the Canada Revenue Agency:
- raise awareness about the disability supports deduction, including special information sessions to inform disability organizations, post-secondary educational institutions and student networks, unions, employer organizations, training programs and the general public about the availability, purpose and provisions of this tax measure; and
- in collaboration with the disability community, review on an annual basis the list of allowable items within the disability supports deduction to ensure it keeps pace with technological updates and changes.
41
That the Canada Revenue Agency take steps to raise awareness among employers about any tax measures that provide incentives for hiring persons with disabilities and/or that help offset any of the costs of accommodation.
42
That the Canada Revenue Agency:
- amend the disability supports deduction to allow the deduction of any form of disability-related technical aid, equipment and service required for education, employment and participation in the community; and
- study and report on the implications of converting the current disability supports deduction from a deduction to a credit.
2) Second Annual Report Recommendations
Life-sustaining therapies
That the Canada Revenue Agency (CRA) replace the current eligibility criteria for life-sustaining therapies as set out in Form T2201 with the following:
Individuals who require life-sustaining therapies (LSTs) are eligible for the disability tax credit (DTC) because of the time required to administer these therapies. These are therapies that are life-long and continuous, requiring close medical supervision. Without them, the individual could not survive or would face serious life-threatening challenges. Close medical supervision is defined as monitoring or visits, at least several times annually, with a health provider. These therapies include, but are not necessarily limited to: intensive insulin therapy for type 1 diabetes; chest therapy for cystic fibrosis; renal dialysis for chronic and permanent renal failure; and medically prescribed formulas and foods for metabolic conditions that prevent the safe breakdown of proteins by the liver, including phenylketonuria (PKU) and maple syrup urine disease (MSUD).
Registered disability savings plans (RDSPs)
We recommend that:
In light of the decision to eliminate the requirement to close an RDSP when a beneficiary no longer qualifies for the DTC, the federal government should pay retroactively the RDSP grant and bond portions for which an RDSP holder might be eligible.
We recommend that:
The federal government set up an advisory body, consisting of RDSP applicants and account holders, to resolve long-standing concerns and to address emerging issues with respect to the RDSP and its interface with the DTC. To help address complex issues such as legal capacity, the advisory body should include or consult regularly with selected organizations representing persons with disabilities.
Indigenous issues
That the CRA develop an educational program for leaders, employees and committees in relation to Indigenous peoples, Indigenous disability issues, and funding and government initiatives to promote a better understanding of Indigenous systems in Canada and how the CRA and DTC interact with them.
That the CRA seek financial authority and obtain funding to support community organizations with strong ties to Indigenous peoples, to engage and assist individuals and communities in their efforts to understand and apply for the DTC and other benefits, once DTC eligibility has been confirmed.
That the CRA develop an assessment package, similar to the one used for the Canada Pension Plan application for disability benefits, which speaks to Indigenous peoples and can be:
- completed by the individual or an assessor, which considers how a person’s disability affects them “all, or substantially all, of the time” or an “inordinate amount of time”
- confirmed by a designated health care provider and attached to the main application
That the CRA, in consultation with Indigenous peoples and disability organizations, develop mechanisms for collecting data related to age, gender, type of disability similar to other DTC databases, while respecting the confidentiality of the individual and community. Any new DTC application form should include an option for applicants to identify as an Indigenous person, Métis, Inuit or member of a First Nation (status or non-status).
Work-related disability tax measures
That the CRA forward to the Department of Finance Canada for their consideration the following items to be added to the disability supports deduction list:
- ergonomic work chairs
- bed-positioning devices for work
- mobile computer cart for sit/stand work at home
- alternative input devices (keyboards/ mice)
- digital pens
- navigation devices for low vision
- memory or organizational aids to assist someone with a brain injury or problems with executive function
- trained and certified service animals to enable participation in education, training or work
That the CRA: (proposed change to Recommendation #40)
- raise awareness about the disability supports deduction, including special information sessions to inform disability organizations, post-secondary educational institutions and student networks, unions, employer organizations, training programs and the general public about the availability, purpose and provisions of this tax measure
- in collaboration with the disability community, inform the Department of Finance Canada of the need to review, on an annual basis, the list of allowable items within the disability supports deduction, to ensure it keeps pace with technological updates and changes
3) Third Annual Report Recommendations New
DTC Eligibility
That, in respect of the intent of the Convention on the Rights of Persons with Disabilities, the Department of Finance Canada and the CRA change the term ‘impairment’ to ‘limitation’ in all of its relevant legislation and administrative procedures and documents.
That neither the CRA nor the Department of Finance Canada decide which health provider can complete the form for which functions but rather let the licensed scope of practice of a health provider guide which functions they will assess on behalf of the DTC applicant.
That any licensed health provider, whose license is in good standing, be permitted to complete the T2201 for any area of function.
(modification of an earlier recommendation)
That the CRA replace the current eligibility criteria for life-sustaining therapies as set out in Form T2201 with the following:
Individuals who require life-sustaining therapies (LSTs) are eligible for the DTC because of the time required to administer these therapies. These are therapies that are life-long and continuous, requiring close medical supervision. Without them, the individual could not survive or would face serious life-threatening challenges. Close medical supervision is defined as monitoring or visits, at least several times annually, with a health provider. These therapies include but are not necessarily limited to: intensive insulin therapy for type 1 diabetes; chest therapy for cystic fibrosis; renal dialysis or chronic and permanent renal failure; intravenous feeding for certain genetic conditions and Crohn’s Disease; and foods for metabolic conditions that prevent the safe breakdown of proteins by the liver, including medically prescribed formulas and foods for phenylketonuria (PKU) and Maple Syrup Urine Disorder (MSUD).
Ongoing Committee Work
i. DTC review and appeals
That the CRA share the data it currently collects on the number of objections and appeals, the nature of appeals and the time taken to resolve appeals in order to determine which groups are experiencing challenges in this regard.
That the CRA make clear in its communications that DTC applicants who filed an objection or an appeal remain eligible for all DTC-related gateway benefits until such time as the appeal is resolved.
ii. DTC legal issues
That the Department of Finance Canada amend the Income Tax Act (ITA) and/or that the CRA amend its policy to allow a person to appoint a representative to support them with respect to the management of their tax affairs. This objective can be achieved by:
- adding “supported decision-maker” to the enumerated legal representatives in the definition of legal representatives in s. 248(1) then adding a new section to the ITA which sets out the procedure for appointing a supported/supporting decision-maker; or
- revising the policy applying to the appointment of an “authorized representative” such that it applies to people who may not meet the current capacity requirements to carry out this process.
That, as a broader and more long-term strategy, the federal government apply the Peace, Order and Good Government clause to encourage the creation of a national minimum-standard legislative framework for supported decision-making laws. While amending the Income Tax Act would address the issue of accessing CRA services, persons with disabilities face barriers accessing many other federal supports and services due to the federal government’s position that it must defer to provincial laws on legal capacity.
That the CRA encourage the Department of Finance to adopt its recommendation regarding the exemption of DTC beneficiaries from the capital gains on the sale of a home bequeathed to them through an inter vivos trust.
That the federal government:
- extend the temporary inclusion of “qualified family member” in the definition of “qualifying person” in s. 146.4(1) of the Income Tax Act beyond 2023 and broaden the list of persons defined as “qualified family members” to include siblings
- make the above-stated temporary measures permanent – i.e., all references to “qualified family members” in s. 146.4(1) of the Income Tax Act
- exercise its Peace, Order and Good Government power to create a national minimum-standard legislative framework to ensure that Canadians with disabilities are able to access the benefits of the RDSP through supported decision-making, regardless of the type or degree of their disability or their province or territory of residence
Appendix D: Description of Federal Measures for Persons with Disabilities
Disability tax credit
The disability tax credit (DTC) is a non-refundable tax credit that helps individuals with disabilities or their supporting individuals reduce the amount of income tax they may have to pay. To be eligible for the DTC, an individual must have a severe and prolonged impairment in physical or mental functions, as defined in the Income Tax Act, and has to be certified by one of the following medical practitioners:
- medical doctor;
- nurse practitioner;
- optometrist;
- audiologist;
- occupational therapist;
- physiotherapist;
- psychologist; or
- speech-language pathologist.
Eligibility is not based on a diagnosis, but rather on the effects of the impairment on the ability to perform the basic activities of daily living.
Once the individual with a disability is eligible for the DTC, they may claim the disability amount of $8,662 (for 2021). If the individual qualifies for the disability amount and was under 18 years of age at the end of the year, they may claim an additional supplement of up to $5,053 (for 2021).
A supporting individual or the spouse or common-law partner of the eligible individual with a disability may be able to claim all or part of an unused disability tax credit.
Registered disability savings plan
A registered disability savings plan (RDSP) is a savings plan intended to help parents and others save for the long term financial security of a person who is eligible for the disability tax credit (DTC).
Contributions to an RDSP are not tax deductible and can be made until the end of the year in which the beneficiary turns 59. Contributions that are withdrawn are not included as income to the beneficiary when they are paid out of an RDSP. However, the Canada disability savings grant (grant), the Canada disability savings bond (bond), investment income earned in the plan, and the proceeds from rollovers are included in the beneficiary's income for tax purposes when they are paid out of the RDSP.
The grant is an amount that the Government of Canada pays into an RDSP. The Government will pay a matching grant of 300%, 200%, or 100%, depending on the beneficiary’s adjusted family net income and the amount contributed. Up to $3,500 in matching grants can be paid into an RDSP in one year, and up to $70,000 over the beneficiary’s lifetime. A beneficiary’s RDSP can receive a grant on contributions made until December 31 of the year in which the beneficiary turns 49.
The bond is an amount paid by the Government of Canada directly into an RDSP. The Government will pay a bond of up to $1,000 a year to low-income Canadians with disabilities. No contributions have to be made to get the bond. The lifetime bond limit is $20,000. A bond can be paid into an RDSP if an application is made on or before the end of the year in which the beneficiary turns 49.
Amounts paid from a registered retirement savings plan or a registered retirement income fund upon the death of an annuitant
If an individual was a financially dependent child or grandchild of the deceased annuitant or member who depended on a annuitant or member because of an impairment in physical or mental functions, they may contribute to their registered retirement income fund (RRIF) any amounts they receive or are considered to have received from a deceased annuitant’s or member’s:
- registered retirement savings plan (RRSP);
- pooled registered pension plan (PRPP); or
- specified pension plan (SPP).
An individual can roll over the proceeds of a deceased annuitant’s or member’s RRIF, RRSP, registered pension plan, SPP or PRPP to the registered disability savings plan of a financially dependent child or grandchild who has an impairment in physical or mental functions.
Medical expense tax credit
The medical expense tax credit is a non-refundable tax credit for individuals who have sustained significant medical expenses for themselves or certain of their dependants.
These expenses include a wide range of products, procedures, and services, such as:
- medical supplies;
- dental care; and
- travel expenses.
An individual may claim the total of the eligible expenses minus the lesser of the following amounts:
- $2,421 (for 2021);
- or 3% of the individual’s or dependant’s net income for the year (in respect for whom the credit is claimed).
Certain medical expenses have to be certified by a medical practitioner. Medical practitioners include a wide range of individuals in the medical profession, such as doctors, pharmacists, and nurses.
Refundable medical expense supplement
The refundable medical expense supplement is a refundable tax credit available to working individuals with low incomes and high medical expenses. An individual may be able to claim this credit if all of the following conditions apply:
- They made a claim for medical expenses or for the disability supports deduction;
- They were resident in Canada throughout the year; and
- They were 18 years of age or older at the end of the year.
They must also meet the criteria related to income.
Disability supports deduction
The disability supports deduction provides tax relief for individual taxpayers who have paid for certain medical expenses to enable them to do one of the following:
- be employed or carry on a business (either alone or as an active partner)
- do research or similar work for which the taxpayer received a grant; or
- attend a designated educational institution or a secondary school at which the taxpayer is enrolled in an educational program
Only the individual with the disability can claim this deduction.
There is a list of the specific types of expenditures that will qualify for the disability supports deduction. In many cases, a medical practitioner must prescribe the particular device, equipment or service, or must certify that the individual requires the device, equipment or service because of their impairment.
Students with disabilities
Certain education-related benefits that require an individual to be a full-time student, such as the scholarship exemption, may be claimed by a part-time student if they meet one of the following criteria. The student:
- is eligible for the DTC for the year; or
- has an impairment in physical or mental functions, and a medical practitioner has certified in a letter that the impairment would not reasonably allow the student to be enrolled full-time.
Business expenses for employees with disabilities - related modifications
Business owners can deduct expenses they incur for eligible disability-related modifications made to a building in the year paid to them, instead of adding them to the capital cost of the building.
Eligible disability-related modifications include changes made to accommodate wheelchairs, such as:
- installing hand-activated power door openers
- installing interior and exterior ramps
- modifying a bathroom, an elevator, or a doorway
They can also deduct expenses paid to install or get the following disability-related devices and equipment:
- elevator car-position indicators (such as braille panels and audio indicators)
- visual fire-alarm indicators
- listening or telephone devices for people who have a hearing impairment
- disability-specific computer software and hardware attachments.
In addition, they may be able to deduct expenses for disability-specific computer software and hardware attachments.
Disability-related employment benefits
If a business owner is providing benefits or allowances to an employee who has a disability, such as transportation costs or attendant services, the benefits may not be taxable.
Reasonable transportation costs between an employee’s home and work location (including parking near that location) are not taxable if paid to them or for an employee to whom either of the following applies:
- is legally blind
- has a severe and prolonged mobility impairment, which markedly restricts the individual’s ability to perform a basic activity of daily living–generally, someone who is eligible to claim the disability tax credit
These transportation costs can include an allowance for taxis or specially designed public transit and parking that provide or subsidize for these employees.
Business owners may have employees with severe and prolonged mental or physical impairments. If the business owners are providing reasonable benefits for attendants to help these employees perform their duties of employment, these benefits are not taxable for the employee. The benefits can include readers for persons who are blind, signers for persons who are deaf, and coaches for persons who are intellectually impaired.
Payroll deductions
A disability-related employment benefit excluded from income is not a taxable benefit. Do not deduct Canada Pension Plan contributions, Employment Insurance premiums, or income tax.
Reduce the EI premium rate if providing employees with a short-term disability plan
Some employers provide a wage-loss replacement plan for short-term disability to their employees. If the plan meets certain standards established by the Employment Insurance Regulations, the employer’s EI premiums could be paid at a reduced rate (less than 1.4 times the employee’s premiums).
To benefit from a reduced employer premium rate, register with the EI Premium Reduction Program.
Appendix E: Disability Measures Linked to Disability Tax Credit Eligibility
- Disability tax credit (DTC) (being eligible for the DTC can open the door to other federal, provincial, or territorial programs)
- DTC child supplement
- Child disability benefit
- Medical expense tax credit
- Canada workers benefit
- Child care expenses deduction
- Students with disabilities
- Home Accessibility Tax Credit
- Home accessibility expenses
- Home buyers’ plan
- Home buyers’ amount
- Registered disability savings plan
- Qualified disability trust
- Disability-related employment benefits
Appendix F: Form T2201, Disability Tax Credit Certificate
English - PDF version
French - PDF version
Appendix G: Resources on Language and Disability
- Canadian Association of Broadcasters
- Guideline Diversity and Disability
- Text standards
- UBC Tool kit on inclusive language
- Audience and Diversity
- OCAD is part of Ontario research and Design hub
- No word for disability in AU
- Disability is a colonial construct U of Waterloo
Appendix H: Selected Legal IssuesFootnote 2
Context and Purpose
The Disability Advisory Committee’s subcommittee on the Registered Disability Savings Plan (the “Sub-Committee”) has been tasked with drafting an overview document to contextualize, explore gaps and suggest potential solutions to address the challenges faced by persons with disabilities with respect to certain products, services and benefits under the Income Tax Act (“ITA”), namely:
- Barriers to appointing a CRA representative to manage their tax affairs;
- Legal authorization for Registered Disability Savings Plans; and
- Trusts and the principal residence exemption rule.
Issue 1: CRA Legal Representative
Existing law
Currently, if a person with a mental disability is found to be incapable of managing property (i.e., their financial affairs), the Canada Revenue Agency (“CRA”) requires that another person be named as that person’s legal representative to manage tax matters on their behalf.
“Legal representative” is defined in section 248(1) of the Income Tax Act (the “ITA”) as follows:
legal representative of a taxpayer means a trustee in bankruptcy, an assignee, a liquidator, a curator, a receiver of any kind, a trustee, an heir, an administrator, anexecutor, a liquidator of a succession, a committee, or any other like person, administering, winding up, controlling or otherwise dealing in a representative or fiduciary capacity with the property that belongs or belonged to, or that is or was held for the benefit of, the taxpayer or the taxpayer’s estate. [emphasis added]
The above definition contains: (1) enumerated legal representatives and (2) residual legal representatives. On its website, the CRA states that a “a legal representative is an individual or corporation appointed by a legal document.”Footnote 3 The website then goes on to specify that a legal representative includes someone with a power of attorney, someone named in a representation agreement and a guardian.
Accessing CRA services
If a person is incapable of managing property, but needed to access or update their account information with the CRA, such as a change in address, or the person needed to file their income tax returns, they would not be permitted to deal with CRA directly and would need to be represented by:
- an attorney for property;
- a guardian for property; or
- a representative.
Attorneys for property and guardians for property are substitute decision-makers. All provinces and territories have similar substitute decision-making regimes in place that allow for a legal guardian to be appointed or a power of attorney to be granted. Appointing attorneys and guardians involve a formal legal process. Although guardianship is more invasive and costly than powers of attorney, both appointments result in the deprivation of autonomy of the person with a mental disability with respect to property matters. For people who make not meet the capacity requirements of appointing an attorney, some jurisdictions, provide for an alternative to guardians or attorneys which allows the person to be supported in making decisions (i.e., a Representative under British Columbia’s Representation Agreement Act).
In British Columbia, a “Representation Agreement” may be established for a person who requires support in managing their financial affairs. This supported decision-making approach is consistent with Article 12 of the Convention on the Rights of Persons with Disabilities (“CRPD”) which Canada ratified in 2010.
Nonetheless, creating a supported decision-making relationship requires the taxpayer with a mental disability to (1) live in a province with supported decision-making legislation and (2) meet the required capacity test (though the capacity test is less onerous than that for a power of attorney, it must still be met). Therefore, although CRA’s acknowledgment of supporting decision-makers as legal representatives is welcomed, the Agency must go further to accommodate persons with mental disabilities.
If persons with mental disabilities were permitted to appoint “authorized representatives” as persons without mental disabilities are, that could potentially bridge the gap. At present, taxpayers can appoint a family member, friend, lawyer, accountant, etc. as an authorized representative. The appointment process is quite informal. It involves the taxpayer submitting a form to CRA electronically. However, a taxpayer with a mental disability who has no attorney or guardian may not have sufficient mental capacity to complete and submit the authorized representative form. This often leads to family members contacting CRA. Unfortunately, many family members of persons with mental disabilities complain that when they contact CRA wishing to represent their family members with mental disabilities, they are advised that their options are limited to powers of attorney and guardianship.
Most often, particularly in provinces without supported decision-making legislation, where a person with a disability does not meet the legal threshold to grant a power of attorney, a trusted family member would likely have no choice but to be appointed as the person’s legal guardian in order to be recognized as a legal guardian for CRA purposes. This is problematic for the person as well as their representative because applying for legal guardianship is often an involved and complicated process, requiring a formal capacity assessment of the person, an application with the court, and a significant time and cost commitment. Moreover, a further consequence of appointing a legal guardian is that it removes any ability of the person to make decisions for themselves with respect to their property (and extends to matters that are beyond their engagement with CRA).
Not only is the lack of supported decision-making options in the ITA contrary to Article 12 of the CPRD, which recognizes that people with disabilities should have access to supports they require in exercising their legal capacity it may also be inconsistent with the spirit of the Accessible Canada Act (the “ACA”). The ACA requires federal government departments, including the CRA, to abide by accessibility standards with respect to persons with disabilities. Forthcoming regulations to the ACA will require CRA to meet certain service delivery standards, which include accessible customer service.
The CRA’s insistence on formally-appointed representatives (i.e., legal representatives) is also inconsistent with social assistance programs across the country, which usually allow for representatives to be named, without resorting to legal guardianship. For example, the Ontario Disability Support Program (“ODSP”) allows for a person to be appointed as a trustee to assist an ODSP recipient in the management of their income support if the ODSP is satisfied that the trustee will act in the best interests of the recipient, amongst other factors.
In January 2004, a CRA Technical Interpretation allowed for “next-of-kin” to qualify as a legal representative of a person with a disability, in accordance with the Ontario Disability Support Program Act. The CRA found that the next-of-kin had the power to “administer, wind up, control or otherwise deal in a representative or fiduciary capacity with the property” of the person with a disability, in accordance with the definition of legal representative in the ITA. This Technical Interpretation, however, has not been operationalized by the CRA .
Current gaps and limitations
- Limited representation for persons with mental disabilities: If the CRA determines that a legal representative is necessary, it requires that all tax-related activity, including making even the smallest of changes to their tax account such as a change of address, be carried out by a legal representative. Unless a person with a mental disability has the capacity to appoint an attorney or they live in a Canadian jurisdiction which allows them to appoint a representative (i.e., supported/supporting decision-maker) and they have the requisite capacity to do so, their only option would be to submit to legal guardianship. There is tremendous disproportionality between wanting to update an address with CRA and having to surrender one’s autonomy to do so. An informal means of appointing a representative is a cost and time-saving measure, which preserves a person’s autonomy as (1) the representative’s involvement in the individual’s affairs would be limited to tax matters, (2) the individual can direct the representative or confer their wishes and (3) the individual would retain the power to revoke the representative for any reason. Prohibiting individuals with mental disabilities from informally appointing a representative in like manner to individuals with capacity creates a barrier to accessing CRA services, which is contrary to the ACA, the CRPD and possibly the Canadian Charter of Rights and Freedoms (the “Charter”).
- Jurisdictional issues. The issue of legal capacity falls under the provincial power of property and civil rights at s. 92(13) of the Constitution. The federal government has maintained that it is for the provincial legislatures to conduct law reform to implement supported decision-making. However, federal supports and services are within the remit of the federal government, and it is their responsibility to ensure that such services are as equally accessible as possible to all Canadians, those with and without mental disabilities in all provinces. That responsibility derives not only from Article 12 of the CRPD but potentially from Section 15 of the Charter. Moreover, Canadian constitutional law has recognized that Parliament is permitted to legislate on issues within the provincial heads of power provided certain constitutional requirements are satisfied. Amending the ITA to give persons with mental disabilities greater access to CRA services is a federal aspect to legal capacity which is distinct from provincial aspects. Expanding CRA accessibility does not intrude on provincial authority to make rules on legal capacity with respect to provincial objectives. Therefore, an amendment to the ITA to permit persons with mental disabilities to appoint an “authorized representative”/supporting decision-maker would likely be constitutional.
Recommendations and solutions
- Amend the ITA and/or CRA policy to allow a person to appoint a representative to support them with respect to the management of their tax affairs. This can be achieved by:
- Adding “supported decision-maker” to the enumerated legal representatives in the definition of legal representatives in s. 248(1) then adding a new section to the ITA which sets out the procedure for appointing a supported/supporting decision-maker; or
- Revising the policy applying to the appointment of an “authorized representative” such that it applies to people who may not meet the current capacity requirements to carry out this process.
British Columbia’s Representation Agreement Act may be an appropriate precedent for CRA to include supported decision-making options for people who currently face barriers to engaging with CRA.
- Further, as a broader and more long-term strategy, Parliament apply the Peace, Order and Good Government (“POGG”) clause to encourage the creation of a national minimum-standard legislative framework for supported decision-making laws. While amending the ITA would address the issue of accessing CRA services, there are many federal supports and services which persons with disabilities face barriers in accessing due to the federal government’s general position that they must defer to their provincial laws on legal capacity.
Benefits and outcomes
- Promotes accessible service delivery.
- Giving people more choice, control over, and access to their own accounts and property is in line with this committee’s mandate.Footnote 4
- People will not lose the right to make their own decisions if/when they need to engage with CRA.
- Proven to be effective in other contexts and jurisdictions. Therefore, structure and safeguards already exist and could be applied to the CRA rules.
Issue 2: Legal Authorization for Opening an RDSP
Overview
Current RDSP legislation under the ITA disqualifies adults who have mental disabilities from being their own plan holders. An adult beneficiary of an RDSP can only become the plan holder if they are “contractually competent.” If they aren’t, only a legal guardian or “some other legally authorized person” could become the plan holder on behalf of an adult beneficiary. Recognizing that this requirement left many RDSPs without a plan holder, and given several provincial/territorial jurisdictions’ failure to implement support decision-making, the federal government introduced a temporary measure to the ITA in 2012 designating the parents or spouses of contractually “incompetent” beneficiaries as “qualifying family members” and eligible to become the plan holders of the RDSP.
Relevant legislation
Section 146.4(1) of the ITA:
qualifying person, in relation to a beneficiary of a disability savings plan, at any time, means
- if the beneficiary has not, at or before that time, attained the age of majority, an entity that is, at that time,
- a legal parent of the beneficiary,
- a guardian, tutor, curator or other individual who is legally authorized to act on behalf of the beneficiary, or
- a public department, agency or institution that is legally authorized to act on behalf of the beneficiary;
- if the beneficiary has, at or before that time, attained the age of majority and is not, at that time, contractually competent to enter into a disability savings plan, an entity that is, at that time, an entity described in subparagraph (a)(ii) or (iii); and
- other than for the purposes of subparagraph (4)(b)(iv), an individual who is a qualifying family member in relation to the beneficiary if
- at or before that time, the beneficiary has attained the age of majority and is not a beneficiary under a disability savings plan,
- at that time, no entity described in subparagraph (a)(ii) or (iii) is legally authorized to act on behalf of the beneficiary, and
- in the issuer’s opinion after reasonable inquiry, the beneficiary’s contractual competence to enter into a disability savings plan at that time is in doubt.
qualifying family member, in relation to a beneficiary of a disability savings plan, at any time, means an individual who, at that time, is
- a legal parent of the beneficiary; or
- a spouse or common-law partner of the beneficiary who is not living separate and apart from the beneficiary by reason of a breakdown of their marriage or common-law partnership (membre de la famille admissible)
Qualifying family members can open, manage and make contributions to, the RDSP on behalf of a person who has an intellectual disability. However, it is not a form of supported decision-making and is a temporary measure which is set to expire in December 2023.
Current gaps and limitations
- Sophie’s choice: For many family members, they are caught between their desire to assure the future financial security of their relative, and restricting basic rights to liberty, they know comes with formally placing their relative under a substitute decision-making or guardianship order. Some families are foregoing financial security so their loved one can retain more choice and independence over their own lives. This means that a considerable proportion of the population for which the RDSP was meant to benefit is currently unable to do so. As such, at the end of each year, a cohort of potential beneficiaries age out of eligibility for RDSP thereby losing out on up to $90,000 in federal contributions.
- “Contractually competent”: The contractual competency requirement for beneficiaries of RDSPs is contrary to Article 12 of the CRPD, which Canada has ratified. Under Article 12, Canada agreed to recognize that persons with disabilities enjoy legal capacity on an equal basis with others in all aspects of life and to take measures to ensure that they can access support to exercise legal capacity.
- Death of qualifying family member: The RDSP may be jeopardized when a plan holder of the RDSP, such as a parent, passes away and there is no other qualifying family member. Should this happen, the person would need to have a guardian appointed or leave their RDSP unmanaged indefinitely.
- Inability to open an RDSP. “Contractually incompetent” adult beneficiaries who have no living or willing qualified family members would be unable to open an RDSP in the first place.
Recommendations and solutions
- The federal government can extend the temporary inclusion of “qualified family member” in the definition of “qualifying person” at s. 146.4(1) of the ITA beyond 2023 and broaden the list of persons defined as “qualified family members” to include siblings. Permitting siblings to act as plan holders to RDSPs would be a prudent succession-planning measure, as siblings of a persons with mental disabilities are statistically expected to outlive their parents. Also, it could act as means of relieving an ailing parent of a person with a mental disability from having to continue to manage their RDSP.
- Make the above-stated temporary measures permanent – i.e. all references to “qualified family members” in s. 146.4(1) of the ITA.
- As suggested in the recommendations section at Issue 1 above, exercise the federal Peace, Order and Good Government power to create a national minimum-standard legislative framework to ensure Canadians with disabilities are able to access the benefits of the RDSP through supported decision- making, regardless of the type or degree of their disability or their province or territory of residence.
Benefits and impact
- The contractual capacity requirement would no longer be a barrier for people wanting to open an RDSP.
- The “qualifying family member” would enable, not restrict, the adult’s legal capacity.
- Having a national strategy will minimize barriers for people if they move out-of-province and will create a stronger framework for provincial governments and financial institutions.
Issue 3: Trusts and the Principal Residence Exemption
Overview
In 2016, the definition of “principal residence” was amended in s.54 of the ITA to limit eligibility for principal residence exemption (“PRE”) to certain categories of trusts, none of which included an inter vivos trust.
This means that if a principal residence was among the assets of an inter vivos trust and the beneficiary of the trust is a person with a disability, the trust could be liable for any capital gains upon the sale of the home. However, testamentary trusts (i.e., trusts arising upon the death of the testator), with beneficiaries who are eligible for the federal Disability Tax Credit (“DTC”), can claim the PRE.
In 2019, the Department of Finance recommended that the Minister of Finance amend the ITA to allow inter vivos trusts involving an eligible beneficiary with a disability to be able to claim the PRE. To date, no such action has been taken.
Current gaps and limitations
- Where an inter vivos trust holds a principal residence for beneficiary with a disability, the beneficiary is unable to benefit from the PRE.
Recommendations and solutions:
- The recommendation of the Assistant Deputy Minister – Legislative, Tax Policy Branch in a comfort letter dated September 4, 2019, be adopted. In that letter, the Assistant Deputy Minister agreed that inter vivos trusts with DTC-eligible beneficiaries ought to enjoy the same exemption as testamentary trusts. He undertook to recommend to the then Minister of Finance that the ITA be amended to permit trusts to designate a property as the principal residence provided all other designation requirements are fulfilled and the following conditions are satisfied:
- a beneficiary of the trust is an individual resident in Canada during the year who is eligible for the DTC;
- the beneficiary is a child, spouse, common-law partner, or former spouse or common-law partner of the settlor of the trust; and
- no person other than a beneficiary described above may, during the beneficiary’s lifetime, receive or otherwise obtain the use of any of the income or capital of the trust.
Benefits and impact
- The beneficiary would not face a barrier in benefiting from the PRE due to their disability.
Conclusion and Next Steps
People with disabilities should not be put in the position of having to choose between attaining financial security and retaining some measure of autonomy.
These recommendations put forward here would successfully remove the above-mentioned barriers that persons with disabilities regularly encounter when trying to access certain products, services and benefits under the ITA.
Appendix I: Canada Disability Benefit
Context
In the introduction to this third annual report, the Committee noted that our mandate is to propose improvements to disability tax measures.
Canadians with disabilities that are severe and prolonged typically face higher costs than persons without disabilities. That’s where disability tax measures come into play. They help recognize these additional costs by providing modest reductions in income tax that is owed to the government.
The income tax system recognizes two different types of disability-related costs: itemizable and non-itemizable costs.
Itemizable costs
The first category involves costs that can be clearly identified and for which proof of payment must be made available upon request. Examples of expenses that can be readily costed include:
- equipment that assists with breathing
- hearing or visual aids
- mobility devices
- special computer hardware and software
- behavioural assessment and intervention services
- attendant care workers
The primary tax measures in this first category are the medical expense tax credit (METC) and the disability supports deduction (DSD).
The METC helps offset the cost of designated health- and disability-related items. There is a long list of items that are permitted under this measure.
The METC can be claimed by all Canadians and there is no need to establish eligibility on the basis of disability in order to claim this credit. But because the METC is designed as a non-refundable tax credit, it is not helpful for Canadians with no taxable income.
Non-refundable tax credits can reduce income tax owing to zero. But no money is paid back to taxfilers if there is a negative balance after the tax credits for which they are eligible are applied against the amount of income tax they owe.
The disability supports deduction (DSD) allows individuals with an impairment in physical or mental functions to deduct the expenses that they paid in that tax year to enable them to work, go to school or conduct research for which a grant was received.
In contrast to the METC which is a tax credit, the DSD is a tax deduction. This means that the actual costs incurred for education, training and employment can be deducted directly from earned income. A deduction reduces the income base on which taxes must be paid.
Even though the DSD can bring substantial assistance to Canadians with disabilities, many people seem to be unaware of this measure and its take-up is limited. In 2022, the federal government will spend an estimated $3 million on the DSD compared to $1.35 billion in that year on the DTC.
In our earlier annual reports, the Committee expressed concern about this problem and recommended several ways to raise awareness about the DSD and improve its provisions.
Non-itemizable costs
The second category of costs involves disability-related goods and services that are not easily itemized. However, they are still very real and can be quite significant. Examples include:
- higher utility charges for heating, air conditioning or electricity
- additional travel involved in getting to an accessible store
- higher cost of items sold at the accessible store
- wear-and-tear of clothing items
The DTC provides some tax relief for these harder-to-itemize costs. Because it is a non-refundable credit, taxfilers must have a taxable income in order to get any benefit from this tax measure.
The disability tax measures described above – medical expense tax credit (METC), disability supports deduction (DSD) and disability tax credit (DTC) – are important forms of assistance to reduce disability costs. They all recognize that persons with disabilities often face greater hardship in meeting their basic needs than persons without disabilities.
However, these tax measures are not income security programs. These three tax measures are neither intended nor designed to help pay for basic needs, such as food, housing, clothing and transportation.
Not surprisingly, people who cannot afford the basic costs of daily living typically have difficulty paying for disability-related goods and services. Our Committee has expressed concern about this ability-to-pay issue.
In fact, as we noted in our previous work, Canadians with disabilities face disproportionately higher rates of poverty than those without disabilities. In our first annual report, Recommendation #38 proposed that the federal government take action to reduce poverty among persons with disabilities. We proposed:
That the Minister of National Revenue work collaboratively with the Minister of Finance, Minister of Families, Children and Social Development, and the Minister of Sport and Persons with Disabilities to:
- identify ways of addressing the disproportionate poverty of Canadians with disabilities, or alternatively, that the Minister of National Revenue request the establishment of a parliamentary committee to address this issue and bring forward recommendations;
- transform, as a first step, the current DTC from a non-refundable credit into a refundable credit in order to recognize the non-itemizable costs incurred by lower-income Canadians with disabilities; and
- ensure that the poverty alleviation of Canadians with disabilities is a focus of all relevant federal-provincial/territorial ministers’ meetings and that there be no provincial/territorial clawback of any new or improved federal measures.
Our Committee was pleased to see the announcement of a Disability Inclusion Action Plan in the 2020 Speech from the Throne. The Plan has several components:
- a new Canadian Disability Benefit (CDB) modelled after the Guaranteed Income Supplement (GIS) for seniors
- a robust employment strategy for Canadians with disabilities
- a better process to determine eligibility for government disability programs and benefits
The associated Disability Inclusion Action Plan spelled out five key objectives. The federal government intends to:
- improve the social and economic inclusion of persons with disabilities
- reduce poverty among persons with disabilities
- achieve the Accessible Canada Act goal of a barrier-free Canada by 2040
- develop a consistent approach to disability inclusion across the Government of Canada and make it easier for persons with disabilities to access federal programs and services, and
- foster a culture of disability inclusion
Our Committee is particularly interested in the new CDB because it could go a long way toward reducing the high rate of poverty among persons with disabilities in Canada. Technically, its design could have significant implications for the DTC.
Design of the new CDB
The federal government had indicated its intent to design the CDB as a supplement to existing programs. More specifically, the Throne Speech made reference to the Guaranteed Income Supplement (GIS) for older Canadians as a model for this new benefit.
An income supplement can be designed in several ways. A supplement can reduce poverty by guaranteeing a basic income level. Alternatively, it can be designed to reduce poverty by helping to offset additional costs that eligible individuals are deemed to incur.
In the first case, the supplement is a variable amount that bolsters income from existing programs and employment up to a designated level. This is the GIS model, which ensures an income guarantee for older Canadians.
In the second case, a supplement is a predetermined amount paid to all households that qualify, as in the Canada Child Benefit (CCB). The purpose of the CCB is to provide some financial assistance to lower- and modest-income families with children in recognition of the fact that these households incur higher costs than families without children.
The design of any supplement, whether it bolsters basic income or reduces household costs, always takes into account various sources of income that are currently available to the beneficiary. Employment earnings, benefits from income programs and/or private investment are typically counted as income. The value of tax credits is not included as income.
In the case of the CDB, the value of the Canada Pension Plan Disability Benefit, for example, would be considered income available to the applicant. However, the value of the DTC and other disability tax measures that help reduce taxes but do not pay a benefit are not counted as income.
The more difficult question with respect to the design of income supplements is whether eligibility and/or the amount of the benefit should be calculated on the basis of individual income or family income.
Most poverty advocates and members of the disability community prefer an individual income test. The latter is considered more respectful of the independence of the applicant. Their income alone is taken into account in determining eligibility and the associated amount of payment.
Poverty advocates also argue that governments should not assume in their program design that a given individual actually has access to the general household income. This is often the case for women who do not have complete or even partial access to the income earned by or available to their partner.
Governments, by contrast, prefer to design income supplements based on family income. The total cost of the measure is lower when benefits are calculated in this way. Governments can also argue that families typically develop household budgets and not individual budgets because basic expenditures, such as food, housing and utilities, are shared by all members of that household.
It is possible, however, to combine both methods in the design of an income supplement. The Canada Workers Benefit, for instance, determines initial eligibility and benefit levels on the basis of individual income. However, the amount of the supplement phases out according to family income, thereby taking into account other available sources of income.
The implications of the CDB for the DTC, in particular, will be shaped largely by this basic conceptual decision – whether the design of the new benefit provides an adequate income guarantee or whether it reduces the additional costs linked to severe and prolonged disability. These implications are discussed below.
It should be noted that another supplement, the Canada Workers Benefit, is a third model that could be used as the foundation for the new CDB. However, this income supplement is intended only for individuals with earnings from paid employment.
Because so many persons with disabilities have modest or no work earnings, the new CDB would have to supplement their income up to a designated level. In this case, the design would be a modified version of the minimum income guarantee.
Option #1: Minimum income guarantee
i. The design
The 2020 Throne Speech announced that the new CDB would be modelled on the Guaranteed Income Supplement for older Canadians. The GIS ensures a minimum income guarantee for all Canadians aged 65 and older.
In association with the Old Age Security program, the GIS closes the gap between current income from various sources and a designated amount deemed as a minimum for a decent standard of living.
In 2022, the GIS paid a maximum $968.86 per month or $11,626.32 a year to single, widowed or divorced pensioners. Benefit amounts vary by family type and income. When combined with the basic Old Age Security payment, maximum retirement benefits in 2022 are $1,617.53 a month or $19,410.36 a year.
The GIS supplements income from all other sources, including private pensions, RRSPs, investment income and earned income, up to a designated level. Older Canadians with no income from any other sources, such as the Canada Pension Plan, RRSPs or other private pension, receive the maximum income guarantee. The GIS declines in value as income from other sources increases.
The formula can be summed up as follows. The more money a person receives from various sources, the lower the value of their GIS. Once their income exceeds a designated level, they are deemed not to need the maximum amount from the government. They receive declining amounts until a certain income level, at which time the GIS ends entirely.
As noted, the GIS acts as a supplement to a variety of retirement income programs. Each of these programs has its own eligibility criteria, benefit levels and rules. The only qualifications for the GIS are age (65 and over) and income level.
If the new CDB were designed in this way, the current landscape of disability income programs would remain intact. These include the Canada Pension Plan Disability Benefit, private disability pension plans, Veterans’ Disability Benefits, provincial/territorial Workers’ Compensation and (presumably) provincial/territorial social assistance (also known as “welfare”). The current eligibility criteria for these programs, along with their associated benefits and rules, would stay in place.
ii. Implications for the DTC
Because the DTC is not an income program but rather a tax credit, the DTC would not be counted as income for the purposes of the CDB.
However, eligibility for the DTC could be used as a screen for qualifying for the CDB. The DTC can act as another entry point to the CDB in addition to the other disability income programs that could also play that role, as described earlier in this report.
The DTC had provided the eligibility screen for the COVID Disability Benefit that the federal government announced as one-time assistance in response to additional pandemic-related costs. After the announcement, the eligibility criteria for the new COVID Disability Benefit were expanded because the DTC screen alone was deemed too restrictive.
An eligibility problem for the new CDB would arise in the case of individuals who do not qualify for any of the above disability income programs or for the DTC. New eligibility criteria for the CDB would have to be developed.
In this case, it would make sense for the federal government to build on the current DTC eligibility criteria rather than start from scratch. Despite their complexity, the DTC requirements are noteworthy because they:
- have no work requirements so no applicant would be rejected on the basis of labour force participation
- are based not on condition (with the exception of blindness) but rather on functional impairment, which means they are closer to the social model of disability intended in the Convention on the Rights of Persons with Disabilities
- are open to persons with a range of disabilities because eligibility is not tied to a specific diagnosis or set of circumstances (e.g., disabilities that are acquired or those present at birth)
Finally, if the CDB were designed as a GIS-style income supplement, the DTC would still have a vital role in offsetting disability-related costs. As noted, it would also be one of several gatekeepers to the new program – basically an extension of the function it already plays.
It should be noted that the federal government could decide to dismantle the DTC and use its estimated $1.35 billion annual expenditure toward the CDB. However, that reform would remove all assistance with the cost of non-itemizable disability-related goods and services.
Moreover, individuals with higher earnings would not receive any assistance because their earnings might exceed the maximum income threshold for qualifying for the new benefit. Yet they still would incur disability-related costs.
The second type of supplement design could have greater implications for the DTC. Its role potentially could change substantially, as described below, if both the DTC and the new CDB effectively had the same purpose.
Option #2: Assistance with additional costs
i. The design
The second type of income supplement is a designated amount to help offset certain costs – in this case, disability-related goods and services. The Canada Child Benefit (CCB) is a prime example of this approach. It pays a maximum amount to all families with incomes that fall below a certain level and children under age 18.
The CCB is based on the assumption (and reality) that families with children face additional costs related to larger accommodation, food, clothing, school supplies, health and dental care, and recreational programs. The benefit recognizes that lower- and modest-income families typically face challenges paying these additional costs.
The CCB supplements the income of these households to help them pay child-related expenses. In 2022, the maximum annual CCB is $6,997 per child under age 6 and $5,903 per child ages 6 through 17. These amounts start to be reduced when adjusted family net income exceeds $32,797 (adjustment figures vary by family size).
The one-time COVID Disability Benefit was designed in the same way. Canadians with severe and prolonged disabilities incurred additional pandemic-related costs. These included, for example, extra personal protective equipment, food delivery and other shopping services, and private transportation to avoid public transit.
As noted, the COVID Disability Benefit was modified after its introduction because it was deemed far too restrictive in its coverage. As a one-time payment of $600, it was also considered to be very low. Unless the CDB is far more generous than that amount, it will do little to meet its intended purpose of reducing poverty among persons with disabilities.
ii. Implications for the DTC
In this design, the eligibility criteria for all current programs would remain in place. But a new screen would have to be developed for individuals who currently do not qualify under any existing disability program. As in the GIS design described above, the DTC provides a good foundation for developing these new eligibility criteria.
However, the implications for the future of the DTC could be greater if the new CDB is created as a benefit intended to offset disability-related costs. The DTC currently plays that role. That is its precise purpose. The federal government may well question whether two different measures – one delivered as an income supplement and the other as a tax credit – are required for this purpose.
Under this second type of design whose stated objective would be to reduce disability-related costs, the federal government may decide to dismantle the DTC and incorporate it within the new CDB. There are several advantages and disadvantages to this approach.
On the plus side of the equation, dismantling the DTC would free up an estimated $1.35 billion (in 2022) that could be applied to the new CDB. This approach would address the distributional inequities embedded in the design of the DTC. These have been noted for many years. Its non-refundable design means that low- and modest-income Canadians derive limited benefit from this tax measure. They have little or no income tax payable to reduce.
This inequity is unjust. Low- and modest-income Canadians often incur the same costs as high-income Canadians for the purchase of disability supports. Sometimes, they just make do without the required supports, limiting even more their participation in work and society.
Our Committee had proposed in Recommendation #38 of our first two annual reports that the federal government consider making the DTC a refundable tax credit. Refundable tax credits do more than reduce income taxes to zero. They actually pay to the individual the amount that exceeds zero after they calculate the difference between their income tax owing and the tax credits for which they are eligible.
On the negative side of the equation, eliminating the DTC and rolling it into the CDB would result in major losses for several key groups.
Because the GIS is already in place to cover older Canadians, the CDB likely will be directed toward persons of working age. An income supplement for those of working age only (18-64) means that Canadians aged 65 and over and families with children under 18 would be the primary ones to lose if the DTC were dismantled. These two groups currently comprise a substantial proportion of the overall DTC caseload.
In fact, 43.7% of DTC beneficiaries were over age 65 in 2019. Applicants under age 18 made up another substantial group at 16.9% in that year. Canadians between the ages of 18 and 64 together comprised only 39.4% of the total DTC caseload.
Until the Committee saw the actual figures, we had not appreciated that older Canadians represented such a large proportion of the DTC caseload. Younger and older people together comprise the majority (60.6%) of DTC cases. These two large groups would lose tax-related assistance if the DTC were removed.
It is not surprising that older Canadians make up a relatively large proportion of the DTC caseload. Some impairment in functional capacity is considered a normal part of aging. In fact, older Canadians will continue to be disproportionately represented as a proportion of the overall DTC caseload for two reasons:
- current DTC beneficiaries are aging into the program
- new beneficiaries will apply as a result of the aging of the population
Any move to dismantle the DTC undoubtedly would create problems if so many older Canadians were cut off from the DTC and the savings redirected toward a new disability benefit intended only for Canadians of working age. The government needs to consider how to handle the possible fallout it likely would face.
Our Committee has discussed whether there are better ways, other than the DTC, of meeting the needs of older Canadians. For example, we had considered possible increases to the age tax credit or some type of disability supports program, given the need for a variety of assistive devices. Of course, these options come with an associated cost that could be far greater than the DTC.
The impact on families with children under age 18 who have severe and prolonged disabilities would also have to be addressed. One possibility is to increase the value of the Child Disability Benefit, which is delivered only to families with low and modest incomes.
Unfortunately, the Committee has no information on the efficacy and reach of the current Child Disability Benefit. It is difficult to find any data on government websites regarding the caseload of this particular program and its associated costs.
There would still need to be some form of eligibility screen in place. Right now, the DTC acts as the gateway to the Child Disability Benefit. The new CDB eligibility criteria could be used in its place.
One option is to retain the DTC only for older Canadians and families with children under age 18 with severe and prolonged disabilities. Lower- and modest-income Canadians of working age would be covered by the CDB. But the latter could leave out higher-income individuals of working age who incur very high disability-related costs. (While the new CDB will likely be paid only to Canadians of working age, it will be available to all persons with disabilities regardless of employment status. The reference to “working age” does not equate with “at work” - though the latter is encouraged where possible.)
The option of retaining the DTC for certain age groups only adds complexity to the system of disability income and tax measures. But at least it tries to address the fact most of the current DTC beneficiaries potentially could lose their current tax assistance because of their younger or older age.
Finally, if the DTC is dismantled, a new gateway or entry point to other disability benefits and programs will need to be put in place. The challenges with which our Committee has been grappling will undoubtedly continue as the many complex eligibility issues will not be easily resolved just by moving the process to another government department or new administration.
Other Considerations
i. Disability supports
Any income supplement, whether in the form of an income guarantee as in Option #1 or cost offset as in Option #2, will never be sufficient to meet the needs of some individuals who incur very high disability-related costs. It is virtually impossible for any generally provided supplement to compensate for all the possible additional disability-related expenses a given individual may have to pay.
Nor can any income supplement ever be sufficiently individualized to meet a diverse range of needs. These must be must be tackled through a combination of measures that include:
- various forms of accessibility accommodation
- individualized funding
- tax-related assistance with costs
- the provision of goods and services
We recognize that provinces/territories and many not-for-profit organizations administer multiple programs that provide disability-related goods and services. But these programs are often restricted to certain forms of disability, such as paraplegia or blindness, or to selected types of equipment, such as wheelchairs, special eyeglasses or breathing equipment.
Several jurisdictions also operate financial programs that reduce the cost of disability-related items by paying a certain percentage of these costs. However, there is often a remaining portion that individuals must pay on their own. If the individual has no means to cover the remaining costs, then the program provides no benefit at all. All this to say: The system of disability supports in Canada is overly complex and seriously inadequate.
Some might argue that many higher-income Canadians are likely able to afford the additional costs of disability supports. However, this is not necessarily true. In many cases, individuals pay thousands of dollars a year for disability supports that enable their participation in the paid labour market or in society, more generally.
The wide-ranging problems related to the availability and affordability of disability supports have been documented in many reports over the years. There is minimal and generally haphazard assistance to help offset these costs. It is important to think carefully about the role that the DTC plays in this regard before restructuring or even dismantling this tax measure.
Others may argue, however, that a supplement which replaces the DTC and helps to reduce disability-related costs is a positive step. While a new CDB may exclude certain age groups, it would include low- and modest-income Canadians who previously had been ineligible for DTC-related tax assistance.
ii. Clawbacks
The introduction of any new income benefit always comes with the hazard of associated clawbacks. Other programs may try to reduce their benefits and related expenditures because recipients’ needs are deemed to be met in some other way. These programs may try to limit their caseloads or cut back on the payments they provide.
Clawbacks often end up defeating the purpose of newly-introduced benefits, whose objective is to ensure that recipients are better off. Safeguards would need to be introduced to prevent this unintended – but all too frequent – consequence.
iii. Work disincentives
The CDB must be designed so as not to discourage participation in the paid labour market. Several income programs, notably provincial and territorial social assistance, discourage paid work because of their heavy taxback of employment income. Their substantial recuperation of earned income comprises a significant component of the so-called “welfare wall.”
The CDB will likely be intended only for people of working age. Its challenge will be to ensure that it does not penalize labour force participation for those who are able to earn full or partial income through paid work. This consideration is particularly important for people whose disabilities may be severe but episodic where the inability to work all the time, combined with the welfare wall, may force a decision to not work at all.
The concern about not penalizing labour force participation arises particularly around the guaranteed income design set out in Option #1. The lessons from the GIS are instructive.
The GIS is generally considered a well-designed program that is highly regarded by Canadians. However, the main criticism has long been that its value reduces too steeply if a beneficiary has modest earnings or investment income. Each $2 of income over and above a minimum exemption reduces the GIS by $1. While this 50 percent “reduction rate” helps lower the overall cost of the program, it is seen as way too high from the perspective of work and savings.
In recognition of these concerns, the federal government eased the exemption on earned income. As of 2020, GIS recipients can earn up to $5,000 from employment or self-employment before their benefits are reduced. In addition, 50% of the next $10,000 of employment or self-employment earnings is also exempt.
The Convention on the Rights of Persons with Disabilities, to which Canada is a signatory, calls for the inclusion and participation of persons with disabilities. The design of government programs must respect – not contravene – this principle.
iv. Gateway role
Finally, if the DTC is subsumed by the CDB, then its vital role as gatekeeper to other disability benefits will have to be revisited. There has been discussion for years about a single-entry point for all federally-delivered disability programs, possibly through Employment and Skills Development Canada (ESDC) or Service Canada. The need for ease of access to disability programs has been made clear by the challenges Canadians face in applying for the DTC – which, in fact, gave rise to the appointment of our Committee.
Despite the myriad challenges associated with the DTC, it is important to recognize that this tax measure is currently the only federal disability program that employs impairment in functional capacity as its key eligibility criterion. Regardless of what actually happens to this tax measure in the coming years, its qualifying requirements will be relevant for any new disability benefit in future.
The DTC comes closer than any other federal program to the social model of disability advanced in the Convention on the Rights of Persons with Disabilities. Its main limitation in more completely actualizing the social model is its reliance on health providers to assess eligibility.
The reliance on health providers is particularly problematic because they are often not in the best position to evaluate function all or substantially all of the time. While some conditions, such as blindness or paraplegia, mean that a person cannot see or walk all or substantially all of the time, this is not true of many other severe disabilities. For example, someone with progressive dementia may be able to dress themselves sometimes but may not be able to reliably dress themselves all or substantially all of the time.
Any program or eligibility screen that moves away from a medical model of disability toward a functional model will face the same challenges with which our Committee has grappled. These include but are not limited to:
- assessment of impairment in mental function and/or episodic conditions
- possible expansion of the list of qualified health providers (and possibly beyond health providers) to complete the T2201 Form
- outreach to and access by Indigenous Peoples and other equity-deserving Canadians
These challenges will remain even if the DTC is restructured or eliminated. Moreover, as noted, any change to the DTC must consider how to replace the associated losses that many Canadians will experience in the face of any fundamental DTC reform.
Conclusion
Regardless of the design of the new CDB, we believe that continued support for our Committee will be necessary to provide equity of access to tax assistance and disability benefits. Whether the DTC remains intact or is subsumed by the CDB, there will still be a need for improved disability-related eligibility criteria, more fair and efficient administrative procedures, and more effective outreach to the disability community and Canadians, more generally.
On October 18, 2022, the federal bill responsible for the Canada Disability Benefit (Bill C-22) passed Second Reading in the House of Commons.
Appendix J: Factsheet – Indigenous Peoples
Appendix K: Updated Tables for the Disability Tax Credit Statistical Publication
Tables in PDF format
Statistics by number
- Table 1: Number of individuals with a DTC certificate by province/territory and restriction, 2020
- Table 2: Number of individuals with a DTC certificate by province/territory and age group, 2020
- Table 3: Number of individuals with a DTC certificate by province/territory and duration, 2020
- Table 4: Number of individuals with a DTC certificate by age group and restriction, 2020
- Table 5: Number of individuals with a DTC certificate by age group and duration, 2020
- Table 6: Number of individuals with a DTC certificate by gender and age group, 2020
- Table 7: Number of individuals with a DTC certificate by gender and marital status, 2020
- Table 8: Number of individuals with a DTC certificate by duration and restriction, 2020
- Table 9: Number of individuals with a DTC certificate by gender, age group, and restriction, 2020
- Table 10: Number of individuals with a DTC certificate by gender, age group, and marital status, 2020
- Table 11: Number of individuals with a DTC certificate by age group, Province/Territory and restriction, 2020
- Table 12: Number of DTC determinations by BADL, 2011-2020
- Table 13: Number of DTC claimants benefitting through a tax reduction by BADL, 2011-2020
- Table 14: Number of DTC utilization by BADL, 2011-2020
Statistics by percentage
- Table 1: Percentage of individuals with a DTC certificate by province/territory and restriction, 2020
- Table 2: Percentage of individuals with a DTC certificate by province/territory and age group, 2020
- Table 3: Percentage of individuals with a DTC certificate by province/territory and duration, 2020
- Table 4: Percentage of individuals with a DTC certificate by age group and restriction, 2020
- Table 5: Percentage of individuals with a DTC certificate by age group and duration, 2020
- Table 6: Percentage of individuals with a DTC certificate by gender and age group, 2020
- Table 7: Percentage of individuals with a DTC certificate by gender and marital status, 2020
- Table 8: Percentage of individuals with a DTC certificate by duration and restriction, 2020
- Table 9: Percentage of individuals with a DTC certificate by gender, age group, and restriction, 2020
- Table 10: Percentage of individuals with a DTC certificate by gender, age group, and marital status, 2020
- Table 11: Percentage of individuals with a DTC certificate by age group, Province/Territory and restriction, 2020
- Table 12: Percentage of DTC determinations by BADL, 2011-2020
- Table 13: Percentage of DTC claimants benefitting through a tax reduction by BADL, 2011-2020
- Table 14: Percentage of DTC utilization by BADL, 2011-2020
Tables in HTML format
- Individuals with a DTC certificate, 2020
- Table 1 – Province/territory and restriction
- Table 2 – Province/territory and age group
- Table 3 – Province/territory and duration
- Table 4 – Age group and restriction
- Table 5 – Age group and duration
- Table 6 – Gender and age group
- Table 7 – Gender and marital status
- Table 8 – Duration and restriction
- Table 9 – Gender, age group and restriction
- Table 10 – Gender, age group, and marital status
- Table 11 – Age group, province/territory and restriction
- Statistics by BADL, 2011-2020
Individuals with a DTC certificate, 2020
Table 1 – Province/territory and restriction
This table presents the number of individuals with an accepted DTC certificate by province or territory of residence and restriction in one or more BADLs as reported by a medical practitioner to the CRA. Individuals who report multiple restrictions on their DTC certificate are counted for each restriction, while the "Total Unique Certificates" column presents a count of unique eligible individuals for that province or territory. As such, this column will not add up to the sum of the previous columns.Footnote 5
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 1,010 | 12,870 | 2,530 | 8,950 | 2,120 | 2,240 | 6,110 | 3,100 | 4,360 | 2,750 | 31,670 |
| Prince Edward Island | 300 | 4,130 | 470 | 3,100 | 380 | 510 | 1,340 | 750 | 970 | 900 | 9,510 |
| Nova Scotia | 1,760 | 26,640 | 3,610 | 17,820 | 2,950 | 3,630 | 9,920 | 5,650 | 4,790 | 4,850 | 56,740 |
| New Brunswick | 1,470 | 17,660 | 3,890 | 14,160 | 3,230 | 3,270 | 7,510 | 4,570 | 3,850 | 3,220 | 41,800 |
| Quebec | 9,930 | 60,680 | 31,570 | 87,370 | 10,090 | 18,010 | 30,270 | 14,770 | 11,120 | 14,740 | 192,930 |
| Ontario | 22,570 | 260,840 | 60,400 | 219,750 | 30,620 | 53,050 | 119,590 | 63,020 | 34,710 | 46,420 | 570,660 |
| Manitoba | 2,420 | 38,100 | 5,240 | 27,170 | 3,520 | 4,900 | 13,660 | 6,840 | 4,720 | 5,690 | 79,180 |
| Saskatchewan | 1,700 | 18,310 | 3,530 | 14,730 | 2,100 | 3,090 | 6,930 | 4,470 | 3,720 | 3,610 | 42,180 |
| Alberta | 4,940 | 57,000 | 16,560 | 59,060 | 6,080 | 11,560 | 24,540 | 14,670 | 12,910 | 13,770 | 147,070 |
| British Columbia | 7,110 | 80,910 | 17,540 | 82,280 | 8,740 | 16,450 | 33,840 | 19,720 | 12,280 | 19,850 | 200,370 |
| Yukon | 50 | 320 | 160 | 470 | 30 | 80 | 160 | 110 | 90 | 100 | 1,050 |
| Northwest Territories | 40 | 360 | 110 | 380 | 50 | 90 | 160 | 120 | 90 | 120 | 1,020 |
| Nunavut | 30 | 130 | 90 | 140 | 50 | 70 | 90 | 40 | 30 | 30 | 380 |
| Outside Canada | 330 | 1,330 | 340 | 850 | 300 | 350 | 580 | 320 | 100 | 120 | 2,750 |
| Unspecified | 130 | 570 | 610 | 2,230 | 120 | 380 | 510 | 350 | 80 | 100 | 2,860 |
| Total | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 1.9% | 2.2% | 1.7% | 1.7% | 3.0% | 1.9% | 2.4% | 2.2% | 4.6% | 2.4% | 2.3% |
| Prince Edward Island | 0.6% | 0.7% | 0.3% | 0.6% | 0.5% | 0.4% | 0.5% | 0.5% | 1.0% | 0.8% | 0.7% |
| Nova Scotia | 3.3% | 4.6% | 2.5% | 3.3% | 4.2% | 3.1% | 3.9% | 4.1% | 5.1% | 4.2% | 4.1% |
| New Brunswick | 2.7% | 3.0% | 2.7% | 2.6% | 4.6% | 2.8% | 2.9% | 3.3% | 4.1% | 2.8% | 3.0% |
| Quebec | 18.5% | 10.5% | 21.5% | 16.2% | 14.3% | 15.3% | 11.9% | 10.7% | 11.9% | 12.7% | 14.0% |
| Ontario | 42.0% | 45.0% | 41.2% | 40.8% | 43.5% | 45.1% | 46.9% | 45.5% | 37.0% | 39.9% | 41.3% |
| Manitoba | 4.5% | 6.6% | 3.6% | 5.0% | 5.0% | 4.2% | 5.4% | 4.9% | 5.0% | 4.9% | 5.7% |
| Saskatchewan | 3.2% | 3.2% | 2.4% | 2.7% | 3.0% | 2.6% | 2.7% | 3.2% | 4.0% | 3.1% | 3.1% |
| Alberta | 9.2% | 9.8% | 11.3% | 11.0% | 8.6% | 9.8% | 9.6% | 10.6% | 13.8% | 11.8% | 10.7% |
| British Columbia | 13.2% | 14.0% | 12.0% | 15.3% | 12.4% | 14.0% | 13.3% | 14.2% | 13.1% | 17.1% | 14.5% |
| Yukon Territory | 0.1% | 0.1% | 0.1% | 0.1% | 0.0% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Northwest Territories | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Nunavut | 0.1% | 0.1% | 0.1% | 0.0% | 0.1% | 0.1% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% |
| Outside Canada | 0.6% | 0.2% | 0.2% | 0.0% | 0.4% | 0.3% | 0.2% | 0.2% | 0.1% | 0.1% | 0.2% |
| Unspecified | 0.2% | 0.1% | 0.4% | 0.4% | 0.2% | 0.3% | 0.2% | 0.2% | 0.1% | 0.1% | 0.2% |
| Total | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
Table 2 – Province/territory and age group
This table presents the number of individuals with an accepted DTC certificate broken down by province or territory of residence, and by age group.Footnote 6
| Province/ Territory |
18 and under | 19 to 24 | 25 to 34 | 35 to 44 | 45 to 54 | 55 to 64 | 65 and over | Age unavailable |
Total |
|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 3,810 | 1,140 | 1,690 | 2,140 | 3,820 | 6,760 | 12,300 | 0 | 31,670 |
| Prince Edward Island | 1,180 | 380 | 550 | 570 | 930 | 1,830 | 4,070 | 0 | 9,510 |
| Nova Scotia | 6,910 | 1,910 | 3,000 | 3,060 | 5,620 | 11,410 | 24,820 | 10 | 56,740 |
| New Brunswick | 5,700 | 1,480 | 2,090 | 2,580 | 4,330 | 8,110 | 17,510 | 0 | 41,800 |
| Quebec | 42,790 | 8,660 | 13,800 | 12,550 | 14,300 | 26,150 | 74,640 | 50 | 192,930 |
| Ontario | 89,580 | 21,300 | 33,770 | 31,170 | 44,370 | 84,920 | 265,480 | 90 | 570,660 |
| Manitoba | 10,870 | 2,840 | 4,270 | 4,170 | 6,200 | 12,360 | 38,470 | 10 | 79,180 |
| Saskatchewan | 6,880 | 1,720 | 2,660 | 2,630 | 3,350 | 6,400 | 18,540 | 10 | 42,180 |
| Alberta | 29,970 | 6,670 | 10,250 | 10,740 | 12,790 | 23,150 | 53,490 | 20 | 147,070 |
| British Columbia | 32,610 | 8,390 | 12,700 | 12,460 | 16,290 | 30,060 | 87,830 | 30 | 200,370 |
| Yukon | 240 | 50 | 110 | 90 | 110 | 190 | 270 | 0 | 1,050 |
| Northwest Territories | 210 | 50 | 80 | 90 | 90 | 180 | 330 | 0 | 1,020 |
| Nunavut | 110 | 40 | 40 | 40 | 50 | 60 | 50 | 0 | 380 |
| Outside Canada | 170 | 70 | 170 | 180 | 240 | 360 | 1,560 | 0 | 2,750 |
| Unspecified | 1,420 | 340 | 440 | 230 | 100 | 90 | 250 | 0 | 2,860 |
| Total | 232,450 | 55,020 | 85,620 | 82,700 | 112,580 | 212,020 | 599,590 | 210 | 1,380,180 |
| Province/ Territory |
18 and under | 19 to 24 | 25 to 34 | 35 to 44 | 45 to 54 | 55 to 64 | 65 and over | Age unavailable |
Total |
|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 12.0% | 3.6% | 5.3% | 6.8% | 12.1% | 21.3% | 38.8% | - | 100.0% |
| Prince Edward Island | 12.4% | 4.0% | 5.8% | 6.0% | 9.8% | 19.2% | 42.8% | - | 100.0% |
| Nova Scotia | 12.2% | 3.4% | 5.3% | 5.4% | 9.9% | 20.1% | 43.8% | 0.0% | 100.0% |
| New Brunswick | 13.6% | 3.5% | 5.0% | 6.2% | 10.4% | 19.4% | 41.9% | - | 100.0% |
| Quebec | 22.2% | 4.5% | 7.2% | 6.5% | 7.4% | 13.6% | 38.7% | 0.0% | 100.0% |
| Ontario | 15.7% | 3.7% | 5.9% | 5.5% | 7.8% | 14.9% | 46.5% | 0.0% | 100.0% |
| Manitoba | 13.7% | 3.6% | 5.4% | 5.3% | 7.8% | 15.6% | 48.6% | 0.0% | 100.0% |
| Saskatchewan | 16.3% | 4.1% | 6.3% | 6.2% | 7.9% | 15.2% | 44.0% | 0.0% | 100.0% |
| Alberta | 20.4% | 4.5% | 7.0% | 7.3% | 8.7% | 15.7% | 36.4% | 0.0% | 100.0% |
| British Columbia | 16.3% | 4.2% | 6.3% | 6.2% | 8.1% | 15.0% | 43.8% | 0.0% | 100.0% |
| Yukon Territory | 22.9% | 4.8% | 10.5% | 8.6% | 10.5% | 18.1% | 25.7% | - | 100.0% |
| Northwest Territories | 20.6% | 4.9% | 7.8% | 8.8% | 8.8% | 17.6% | 32.4% | - | 100.0% |
| Nunavut | 28.9% | 10.5% | 10.5% | 10.5% | 13.2% | 15.8% | 13.2% | - | 100.0% |
| Outside Canada | 6.2% | 2.5% | 6.2% | 6.5% | 9.1% | 12.7% | 56.4% | - | 100.0% |
| Unspecified | 48.8% | 12.1% | 15.7% | 8.2% | 3.6% | 3.2% | 8.9% | - | 100.0% |
| Total | 16.8% | 4.0% | 6.2% | 6.0% | 8.2% | 15.4% | 43.4% | 0.0% | 100.0% |
Table 3 – Province/territory and duration
This table presents the number of individuals with an accepted DTC certificate broken down by province or territory of residence, and by the deemed duration of their eligibility, defined as either indeterminate or temporaryFootnote 7
| Province/Territory | Indeterminate | Temporary | Total |
|---|---|---|---|
| Newfoundland and Labrador | 18,050 | 13,630 | 31,670 |
| Prince Edward Island | 6,010 | 3,510 | 9,510 |
| Nova Scotia | 33,130 | 23,600 | 56,740 |
| New Brunswick | 25,120 | 16,680 | 41,800 |
| Quebec | 139,110 | 53,820 | 192,930 |
| Ontario | 385,370 | 185,290 | 570,660 |
| Manitoba | 54,620 | 24,560 | 79,180 |
| Saskatchewan | 28,540 | 13,640 | 42,180 |
| Alberta | 91,810 | 55,260 | 147,070 |
| British Columbia | 128,980 | 71,390 | 200,370 |
| Yukon | 660 | 400 | 1,050 |
| Northwest Territories | 580 | 450 | 1,020 |
| Nunavut | 250 | 130 | 380 |
| Outside Canada | 2,470 | 290 | 2,750 |
| Unspecified | 1,590 | 1,270 | 2,860 |
| Total | 916,270 | 463,910 | 1,380,180 |
| Province/Territory | Indeterminate | Temporary | Total |
|---|---|---|---|
| Newfoundland and Labrador | 57.0% | 43.0% | 100.0% |
| Prince Edward Island | 63.2% | 36.9% | 100.0% |
| Nova Scotia | 58.4% | 41.6% | 100.0% |
| New Brunswick | 60.1% | 39.9% | 100.0% |
| Quebec | 72.1% | 27.9% | 100.0% |
| Ontario | 67.5% | 32.5% | 100.0% |
| Manitoba | 69.0% | 31.0% | 100.0% |
| Saskatchewan | 67.7% | 32.3% | 100.0% |
| Alberta | 62.4% | 37.6% | 100.0% |
| British Columbia | 64.4% | 35.6% | 100.0% |
| Yukon Territory | 62.9% | 38.1% | 100.0% |
| Northwest Territories | 56.9% | 44.1% | 100.0% |
| Nunavut | 65.8% | 34.2% | 100.0% |
| Outside Canada | 89.5% | 10.5% | 100.0% |
| Unspecified | 56.2% | 43.8% | 100.0% |
| Total | 66.4% | 33.6% | 100.0% |
Table 4 – Age group and restriction
This table presents the number of individuals with an accepted DTC certificate broken down by age group, and by restriction(s) in BADL as reported by a medical practitioner to the CRA. Individuals who report multiple restrictions on their DTC certificate are counted for each restriction, while the "Total Unique Certificates" column presents a count of unique eligible individuals for that age group. As such, this column will not add up to the sum of the previous columns. Footnote 8
| Age Group | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 18 and under | 2,630 | 18,760 | 70,650 | 168,530 | 6,340 | 24,510 | 32,730 | 22,380 | 16,870 | 17,880 | 232,450 |
| 19 to 24 | 1,380 | 7,420 | 11,630 | 41,190 | 2,550 | 6,680 | 9,720 | 6,690 | 4,870 | 1,900 | 55,020 |
| 25 to 34 | 3,560 | 16,490 | 15,790 | 54,920 | 5,020 | 10,200 | 14,240 | 10,460 | 8,780 | 3,370 | 85,620 |
| 35 to 44 | 3,840 | 21,980 | 8,370 | 38,510 | 4,960 | 6,900 | 11,550 | 8,710 | 9,090 | 6,960 | 82,700 |
| 45 to 54 | 4,670 | 41,790 | 7,160 | 36,840 | 5,830 | 7,210 | 17,130 | 10,990 | 11,380 | 13,550 | 112,580 |
| 55 to 64 | 7,490 | 105,200 | 9,540 | 50,350 | 9,470 | 12,880 | 36,840 | 18,020 | 16,330 | 26,380 | 212,020 |
| 65 and over | 30,190 | 368,080 | 23,480 | 148,060 | 36,220 | 49,240 | 132,940 | 61,210 | 26,490 | 46,220 | 599,590 |
| Age unavailable | 20 | 130 | 20 | 70 | 10 | 50 | 60 | 30 | 0 | 0 | 210 |
| Total | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Age Group | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 18 and under | 4.9% | 3.2% | 48.2% | 31.3% | 9.0% | 20.8% | 12.8% | 16.2% | 18.0% | 15.4% | 16.8% |
| 19 to 24 | 2.6% | 1.3% | 7.9% | 7.6% | 3.6% | 5.7% | 3.8% | 4.8% | 5.2% | 1.6% | 4.0% |
| 25 to 34 | 6.6% | 2.8% | 10.8% | 10.2% | 7.1% | 8.7% | 5.6% | 7.6% | 9.4% | 2.9% | 6.2% |
| 35 to 44 | 7.1% | 3.8% | 5.7% | 7.2% | 7.0% | 5.9% | 4.5% | 6.3% | 9.7% | 6.0% | 6.0% |
| 45 to 54 | 8.7% | 7.2% | 4.9% | 6.8% | 8.3% | 6.1% | 6.7% | 7.9% | 12.1% | 11.7% | 8.2% |
| 55 to 64 | 13.9% | 18.1% | 6.5% | 9.4% | 13.5% | 10.9% | 14.4% | 13.0% | 17.4% | 22.7% | 15.4% |
| 65 and over | 56.1% | 63.5% | 16.0% | 27.5% | 51.4% | 41.8% | 52.1% | 44.2% | 28.2% | 39.8% | 43.4% |
| Age unavailable |
0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | - | - | 0.0% |
| Total | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
Table 5 – Age group and duration
This table presents the number of individuals with an accepted DTC certificate broken down by age group, and by the deemed duration of eligibility as either indeterminate or temporary.Footnote 9
| Age Group | Indeterminate | Temporary | Total |
|---|---|---|---|
| 18 and under | 33,230 | 199,220 | 232,450 |
| 19 to 24 | 32,890 | 22,140 | 55,020 |
| 25 to 34 | 63,010 | 22,620 | 85,620 |
| 35 to 44 | 51,860 | 30,840 | 82,700 |
| 45 to 54 | 62,860 | 49,720 | 112,580 |
| 55 to 64 | 127,260 | 84,760 | 212,020 |
| 65 and over | 544,970 | 54,620 | 599,590 |
| Age unavailable | 210 | 0 | 210 |
| Total | 916,270 | 463,910 | 1,380,180 |
| Age Group | Indeterminate | Temporary | Total |
|---|---|---|---|
| 18 and under | 14.3% | 85.7% | 100.0% |
| 19 to 24 | 59.8% | 40.2% | 100.0% |
| 25 to 34 | 73.6% | 26.4% | 100.0% |
| 35 to 44 | 62.7% | 37.3% | 100.0% |
| 45 to 54 | 55.8% | 44.2% | 100.0% |
| 55 to 64 | 60.0% | 40.0% | 100.0% |
| 65 and over | 90.9% | 9.1% | 100.0% |
| Age unavailable | 100.0% | 0.0% | 100.0% |
| Total | 66.4% | 33.6% | 100.0% |
Table 6 – Gender and age group
This table presents the number of individuals with an accepted DTC certificate broken down by gender and age group.Footnote 10
| Gender | 18 and under | 19 to 24 | 25 to 34 | 35 to 44 | 45 to 54 | 55 to 64 | 65 and over | Age unavailable |
Total |
|---|---|---|---|---|---|---|---|---|---|
| Female | 71,830 | 20,440 | 35,080 | 38,680 | 57,730 | 109,100 | 337,320 | 10 | 670,190 |
| Male | 160,580 | 34,550 | 50,070 | 43,480 | 54,780 | 102,870 | 261,840 | 10 | 708,180 |
| Gender Diverse | 10 | 20 | 10 | 10 | 10 | 0 | 10 | 0 | 60 |
| Unknown | 20 | 20 | 470 | 530 | 60 | 40 | 410 | 200 | 1,750 |
| Total | 232,450 | 55,020 | 85,620 | 82,700 | 112,580 | 212,020 | 599,590 | 210 | 1,380,180 |
| Gender | 18 and under | 19 to 24 | 25 to 34 | 35 to 44 | 45 to 54 | 55 to 64 | 65 and over | Age unavailable |
Total |
|---|---|---|---|---|---|---|---|---|---|
| Female | 10.7% | 3.0% | 5.2% | 5.8% | 8.6% | 16.3% | 50.3% | 0.0% | 100.0% |
| Male | 22.7% | 4.9% | 7.1% | 6.1% | 7.7% | 14.5% | 37.0% | 0.0% | 100.0% |
| Gender Diverse | 16.7% | 33.3% | 16.7% | 16.7% | 16.7% | - | 16.7% | - | 100.0% |
| Unknown | 1.1% | 1.1% | 26.9% | 30.3% | 3.4% | 2.3% | 23.4% | 11.4% | 100.0% |
| Total | 16.8% | 4.0% | 6.2% | 6.0% | 8.2% | 15.4% | 43.4% | 0.0% | 100.0% |
Table 7 – Gender and marital status
This table presents the number of individuals with an accepted DTC certificate broken down by gender and marital status.Footnote 11
| Gender | Marital Status | Total |
|---|---|---|
| Female | Married | 221,980 |
| Male | Married | 263,870 |
| Gender Diverse | Married | 10 |
| Unknown | Married | 190 |
| Female | Not Married | 424,810 |
| Male | Not Married | 398,710 |
| Gender Diverse | Not Married | 50 |
| Unknown | Not Married | 340 |
| Female | Undeclared | 23,390 |
| Male | Undeclared | 45,610 |
| Gender Diverse | Undeclared | 0 |
| Unknown | Undeclared | 1,220 |
| Total | - | 1,380,180 |
| Gender | Marital Status | Total |
|---|---|---|
| Female | Married | 16.1% |
| Male | Married | 19.1% |
| Gender Diverse | Married | 0.0% |
| Unknown | Married | 0.0% |
| Female | Not Married | 30.8% |
| Male | Not Married | 28.9% |
| Gender Diverse | Not Married | 0.0% |
| Unknown | Not Married | 0.0% |
| Female | Undeclared | 1.7% |
| Male | Undeclared | 3.3% |
| Gender Diverse | Undeclared | - |
| Unknown | Undeclared | 0.1% |
| Total | - | 100.0% |
Table 8 – Duration and restriction
This table presents the number of individuals with an accepted DTC certificate broken down by restriction and by the deemed duration of eligibility as either indeterminate or temporary. Individuals who report multiple restrictions on their DTC certificate are counted for each restriction, while the "Total Unique Certificates" column presents a count of unique eligible individuals for that duration.Footnote 12
| Restriction | Indeterminate | Temporary | Total Unique Certificates |
|---|---|---|---|
| Vision | 52,860 | 910 | 53,770 |
| Walking | 455,560 | 124,290 | 579,860 |
| Speaking | 82,340 | 64,300 | 146,640 |
| Mental Functions | 323,010 | 215,450 | 538,460 |
| Hearing | 64,640 | 5,760 | 70,400 |
| Feeding | 92,890 | 24,780 | 117,670 |
| Dressing | 198,760 | 56,460 | 255,210 |
| Eliminating | 103,830 | 34,650 | 138,490 |
| Life-Sustaining Therapy | 55,270 | 38,550 | 93,820 |
| Cumulative | 53,340 | 62,920 | 116,260 |
| Total Unique Certificates | 916,270 | 463,910 | 1,380,180 |
| Restriction | Indeterminate | Temporary | Total Unique Certificates |
|---|---|---|---|
| Vision | 98.3% | 1.7% | 100.0% |
| Walking | 78.6% | 21.4% | 100.0% |
| Speaking | 56.2% | 43.8% | 100.0% |
| Mental Functions | 60.0% | 40.0% | 100.0% |
| Hearing | 91.8% | 8.2% | 100.0% |
| Feeding | 78.9% | 21.1% | 100.0% |
| Dressing | 77.9% | 22.1% | 100.0% |
| Eliminating | 75.0% | 25.0% | 100.0% |
| Life-Sustaining Therapy | 58.9% | 41.1% | 100.0% |
| Cumulative | 45.9% | 54.1% | 100.0% |
| Total Unique Certificates | 66.4% | 33.6% | 100.0% |
Table 9 – Gender, age group and restriction
This table presents the number of individuals with an accepted DTC certificate broken down by gender, age group and restriction. Individuals who report multiple restrictions on their DTC certificate are counted for each restriction, while the "Total Unique Certificates" column presents a count of unique eligible individuals for that gender, and age group.Footnote 13
Number of individuals with an accepted DTC certificate by age group
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 1,180 | 8,130 | 19,630 | 46,970 | 2,570 | 8,600 | 10,350 | 6,940 | 7,920 | 5,850 | 71,830 |
| Male | 1,450 | 10,630 | 51,010 | 121,530 | 3,760 | 15,910 | 22,380 | 15,430 | 8,950 | 12,040 | 160,580 |
| Gender Diverse | 0 | 0 | 0 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Unknown | 0 | 0 | 10 | 10 | 0 | 10 | 10 | 10 | 0 | 0 | 20 |
| Total (all age groups and gender) | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 600 | 3,330 | 3,910 | 14,210 | 1,080 | 2,690 | 3,730 | 2,630 | 2,280 | 810 | 20,440 |
| Male | 770 | 4,080 | 7,710 | 26,950 | 1,470 | 3,980 | 5,980 | 4,050 | 2,590 | 1,090 | 34,550 |
| Gender Diverse | 0 | 0 | 0 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 20 |
| Unknown | 0 | 10 | 10 | 10 | 0 | 10 | 10 | 10 | 0 | 0 | 20 |
| Total (all age groups and gender) | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 1,550 | 7,630 | 5,690 | 20,270 | 2,290 | 4,220 | 5,900 | 4,430 | 4,420 | 1,810 | 35,080 |
| Male | 1,970 | 8,670 | 9,990 | 34,380 | 2,690 | 5,880 | 8,220 | 5,950 | 4,350 | 1,550 | 50,070 |
| Gender Diverse | 0 | 0 | 0 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Unknown | 40 | 190 | 120 | 270 | 50 | 100 | 120 | 80 | 10 | 10 | 470 |
| Total (all age groups and gender) | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 1,680 | 10,970 | 3,400 | 15,900 | 2,480 | 3,110 | 5,460 | 4,240 | 4,440 | 4,280 | 38,680 |
| Male | 2,100 | 10,810 | 4,880 | 22,340 | 2,410 | 3,710 | 5,990 | 4,400 | 4,640 | 2,660 | 43,480 |
| Gender Diverse | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Unknown | 60 | 200 | 100 | 270 | 70 | 80 | 90 | 70 | 10 | 10 | 530 |
| Total (all age groups and gender) | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 2,120 | 22,180 | 3,100 | 16,900 | 3,060 | 3,600 | 8,950 | 5,940 | 5,320 | 8,600 | 57,730 |
| Male | 2,540 | 19,590 | 4,050 | 19,900 | 2,770 | 3,610 | 8,170 | 5,040 | 6,060 | 4,950 | 54,780 |
| Gender Diverse | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Unknown | 0 | 20 | 10 | 30 | 10 | 10 | 10 | 10 | 0 | 0 | 60 |
| Total (all age groups and gender) | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 3,500 | 55,330 | 4,120 | 24,520 | 4,690 | 6,550 | 19,420 | 9,960 | 7,320 | 15,470 | 109,100 |
| Male | 3,990 | 49,860 | 5,420 | 25,800 | 4,770 | 6,330 | 17,420 | 8,070 | 9,010 | 10,910 | 102,870 |
| Gender Diverse | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Unknown | 0 | 10 | 0 | 20 | 0 | 0 | 10 | 0 | 0 | 0 | 40 |
| Total (all age groups and gender) | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 17,600 | 212,530 | 11,190 | 88,040 | 17,130 | 29,260 | 77,720 | 35,150 | 11,400 | 26,280 | 337,320 |
| Male | 12,550 | 155,330 | 12,250 | 59,800 | 19,060 | 19,910 | 55,120 | 25,990 | 15,080 | 19,920 | 261,840 |
| Gender Diverse | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Unknown | 40 | 220 | 30 | 210 | 30 | 70 | 100 | 60 | 10 | 10 | 410 |
| Total (all age groups and gender) | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 0 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Male | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Gender Diverse | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Unknown | 20 | 120 | 20 | 60 | 10 | 50 | 60 | 30 | 0 | 0 | 200 |
| Total (all age groups and gender) | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
Percentage of individuals with an accepted DTC certificate by age group
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 2.2% | 1.4% | 13.4% | 8.7% | 3.7% | 7.3% | 4.1% | 5.0% | 8.4% | 5.0% | 5.2% |
| Male | 2.7% | 1.8% | 34.8% | 22.6% | 5.3% | 13.5% | 8.8% | 11.1% | 9.5% | 10.4% | 11.6% |
| Gender Diverse | - | - | - | 0.0% | - | - | - | - | - | - | 0.0% |
| Unknown | - | 0.0% | 0.0% | 0.0% | - | 0.0% | 0.0% | 0.0% | - | - | 0.0% |
| Total (all age groups and gender) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 1.1% | 0.6% | 2.7% | 2.6% | 1.5% | 2.3% | 1.5% | 1.9% | 2.4% | 0.7% | 1.5% |
| Male | 1.4% | 0.7% | 5.3% | 5.0% | 2.1% | 3.4% | 2.3% | 2.9% | 2.8% | 0.9% | 2.5% |
| Gender Diverse | - | - | - | 0.0% | - | - | - | - | - | - | 0.0% |
| Unknown | - | 0.0% | 0.0% | 0.0% | - | 0.0% | 0.0% | 0.0% | - | - | 0.0% |
| Total (all age groups and gender) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 2.9% | 1.3% | 3.9% | 3.8% | 3.3% | 3.6% | 2.3% | 3.2% | 4.7% | 1.6% | 2.5% |
| Male | 3.7% | 1.5% | 6.8% | 6.4% | 3.8% | 5.0% | 3.2% | 4.3% | 4.6% | 1.3% | 3.6% |
| Gender Diverse | - | - | - | 0.0% | - | - | - | - | - | - | 0.0% |
| Unknown | 0.1% | 0.0% | 0.1% | 0.1% | 0.1% | 0.1% | 0.0% | 0.1% | 0.0% | 0.0% | 0.0% |
| Total (all age groups and gender) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 3.1% | 1.9% | 2.3% | 3.0% | 3.5% | 2.6% | 2.1% | 3.1% | 4.7% | 3.7% | 2.8% |
| Male | 3.9% | 1.9% | 3.3% | 4.1% | 3.4% | 3.2% | 2.3% | 3.2% | 4.9% | 2.3% | 3.2% |
| Gender Diverse | - | - | - | - | - | - | - | - | - | - | 0.0% |
| Unknown | 0.1% | 0.0% | 0.1% | 0.1% | 0.1% | 0.1% | 0.0% | 0.1% | 0.0% | 0.0% | 0.0% |
| Total (all age groups and gender) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 3.9% | 3.8% | 2.1% | 3.1% | 4.3% | 3.1% | 3.5% | 4.3% | 5.7% | 7.4% | 4.2% |
| Male | 4.7% | 3.4% | 2.8% | 3.7% | 3.9% | 3.1% | 3.2% | 3.6% | 6.5% | 4.3% | 4.0% |
| Gender Diverse | - | - | - | - | - | - | - | - | - | - | 0.0% |
| Unknown | - | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | - | - | 0.0% |
| Total (all age groups and gender) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 6.5% | 9.5% | 2.8% | 4.6% | 6.7% | 5.6% | 7.6% | 7.2% | 7.8% | 13.3% | 7.9% |
| Male | 7.4% | 8.6% | 3.7% | 4.8% | 6.8% | 5.4% | 6.8% | 5.8% | 9.6% | 9.4% | 7.5% |
| Gender Diverse | - | - | - | - | - | - | - | - | - | - | - |
| Unknown | - | 0.0% | - | 0.0% | - | - | 0.0% | - | - | - | 0.0% |
| Total (all age groups and gender) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 32.7% | 36.7% | 7.6% | 16.4% | 24.3% | 24.9% | 30.5% | 25.4% | 12.2% | 22.6% | 24.4% |
| Male | 23.3% | 26.8% | 8.4% | 11.1% | 27.1% | 16.9% | 21.6% | 18.8% | 16.1% | 17.1% | 19.0% |
| Gender Diverse | - | - | - | - | - | - | - | - | - | - | 0.0% |
| Unknown | 0.1% | 0.0% | 0.0% | 0.0% | 0.0% | 0.1% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% |
| Total (all age groups and gender) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Gender | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | - | 0.0% | - | - | - | - | - | - | - | - | 0.0% |
| Male | - | - | - | - | - | - | - | - | - | - | 0.0% |
| Gender Diverse | - | - | - | - | - | - | - | - | - | - | - |
| Unknown | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | - | - | 0.0% |
| Total (all age groups and gender) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
Table 10 – Gender, age group, and marital status
This table presents the number of individuals with an accepted DTC certificate broken down by gender, age group and marital status.Footnote 14
Number individuals with an accepted DTC certificate by marital status
| Age group | Female | Male | Gender Diverse | Unknown | Total (Married) |
Total (all types of marital status) |
|
|---|---|---|---|---|---|---|---|
| 18 and under | 10 | 10 | 0 | 0 | 20 | 232,450 | |
| 19 to 24 | 570 | 360 | 0 | 0 | 930 | 55,020 | |
| 25 to 34 | 6,650 | 5,100 | 0 | 0 | 11,750 | 85,620 | |
| 35 to 44 | - | 14,530 | 12,300 | 0 | 0 | 26,840 | 82,700 |
| 45 to 54 | 27,690 | 22,750 | 0 | 0 | 50,440 | 112,580 | |
| 55 to 64 | 57,200 | 54,990 | 0 | 0 | 112,200 | 212,020 | |
| 65 and over | 115,330 | 168,360 | 0 | 60 | 283,740 | 599,590 | |
| Age unavailable | 0 | 0 | 0 | 120 | 130 | 210 | |
| Total | 221,980 | 263,870 | 10 | 190 | 486,050 | 1,380,180 |
| Age group | Female | Male | Gender Diverse | Unknown | Total (not married) |
Total (all types of marital status) |
|---|---|---|---|---|---|---|
| 18 and under | 53,960 | 122,460 | 10 | 0 | 176,430 | 232,450 |
| 19 to 24 | 17,830 | 30,910 | 10 | 0 | 48,750 | 55,020 |
| 25 to 34 | 26,840 | 42,520 | 10 | 10 | 69,380 | 85,620 |
| 35 to 44 | 23,650 | 30,410 | 0 | 10 | 54,070 | 82,700 |
| 45 to 54 | 29,870 | 31,790 | 0 | 20 | 61,680 | 112,580 |
| 55 to 64 | 51,680 | 47,670 | 0 | 20 | 99,360 | 212,020 |
| 65 and over | 220,980 | 92,960 | 10 | 220 | 314,160 | 599,590 |
| Age unavailable | 10 | 0 | 0 | 70 | 80 | 210 |
| Total | 424,810 | 398,710 | 50 | 340 | 823,910 | 1,380,180 |
| Age group | Female | Male | Gender Diverse | Unknown | Total | Total (all types of marital status) |
|---|---|---|---|---|---|---|
| 18 and under | 17,860 | 38,110 | 0 | 20 | 56,000 | 232,450 |
| 19 to 24 | 2,030 | 3,290 | 0 | 20 | 5,340 | 55,020 |
| 25 to 34 | 1,590 | 2,450 | 0 | 460 | 4,490 | 85,620 |
| 35 to 44 | 500 | 770 | 0 | 520 | 1,790 | 82,700 |
| 45 to 54 | 170 | 250 | 0 | 40 | 460 | 112,580 |
| 55 to 64 | 220 | 220 | 0 | 20 | 460 | 212,020 |
| 65 and over | 1,020 | 530 | 0 | 140 | 1,690 | 599,590 |
| Age unavailable | 0 | 0 | 0 | 10 | 10 | 210 |
| Total | 23,390 | 45,610 | 0 | 1,220 | 70,220 | 1,380,180 |
Percentage of individuals with an accepted DTC certificate by marital status
| Age group | Female | Male | Gender Diverse | Unknown | Total (Married) |
Total (all types of marital status) |
|---|---|---|---|---|---|---|
| 18 and under | 0.0% | 0.0% | - | - | 0.0% | 16.8% |
| 19 to 24 | 0.3% | 0.1% | - | - | 0.2% | 4.0% |
| 25 to 34 | 3.0% | 1.9% | - | - | 2.4% | 6.2% |
| 35 to 44 | 6.5% | 4.7% | - | - | 5.5% | 6.0% |
| 45 to 54 | 12.5% | 8.6% | - | - | 10.4% | 8.2% |
| 55 to 64 | 25.8% | 20.8% | - | - | 23.1% | 15.4% |
| 65 and over | 52.0% | 63.8% | - | 31.6% | 58.4% | 43.4% |
| Age unavailable |
- | - | - | 63.2% | 0.0% | 0.0% |
| Total | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Age group | Female | Male | Gender Diverse | Unknown | Total (not married) |
Total (all types of marital status) |
|---|---|---|---|---|---|---|
| 18 and under | 12.7% | 30.7% | 20.0% | - | 21.4% | 16.8% |
| 19 to 24 | 4.2% | 7.8% | 20.0% | - | 5.9% | 4.0% |
| 25 to 34 | 6.3% | 10.7% | 20.0% | 2.9% | 8.4% | 6.2% |
| 35 to 44 | 5.6% | 7.6% | - | 2.9% | 6.6% | 6.0% |
| 45 to 54 | 7.0% | 8.0% | - | 5.9% | 7.5% | 8.2% |
| 55 to 64 | 12.2% | 12.0% | - | 5.9% | 12.1% | 15.4% |
| 65 and over | 52.0% | 23.3% | 20.0% | 64.7% | 38.1% | 43.4% |
| Age unavailable |
0.0% | - | - | 20.6% | 0.0% | 0.0% |
| Total | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Age group | Female | Male | Gender Diverse | Unknown | Total | Total (all types of marital status) |
|---|---|---|---|---|---|---|
| 18 and under | 76.4% | 83.6% | - | 1.6% | 79.7% | 16.8% |
| 19 to 24 | 8.7% | 7.2% | - | 1.6% | 7.6% | 4.0% |
| 25 to 34 | 6.8% | 5.4% | - | 37.7% | 6.4% | 6.2% |
| 35 to 44 | 2.1% | 1.7% | - | 42.6% | 2.5% | 6.0% |
| 45 to 54 | 0.7% | 0.5% | - | 3.3% | 0.7% | 8.2% |
| 55 to 64 | 0.9% | 0.5% | - | 1.6% | 0.7% | 15.4% |
| 65 and over | 4.4% | 1.2% | - | 11.5% | 2.4% | 43.4% |
| Age unavailable |
- | - | - | 0.8% | 0.0% | 0.0% |
| Total | 100.0% | 100.0% | - | 100.0% | 100.0% | 100.0% |
Table 11 – Age group, province/territory and restriction
This table presents the number of individuals with an accepted DTC certificate broken down by age group, Province/Territory and restriction. Individuals who report multiple restrictions on their DTC certificate are counted for each restriction, while the "Total Unique Certificates" column presents a count of unique eligible individuals for that age group, and province or territory.Footnote 15
Number of individuals with an accepted DTC certificate by age group
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 50 | 280 | 940 | 2,860 | 110 | 370 | 510 | 320 | 400 | 200 | 3,810 |
| Prince Edward Island | 10 | 70 | 140 | 920 | 20 | 60 | 90 | 60 | 120 | 60 | 1,180 |
| Nova Scotia | 60 | 450 | 1,240 | 5,340 | 150 | 550 | 810 | 520 | 630 | 370 | 6,910 |
| New Brunswick | 70 | 450 | 1,710 | 4,450 | 140 | 540 | 900 | 700 | 420 | 330 | 5,700 |
| Quebec | 520 | 2,980 | 16,750 | 24,750 | 810 | 3,260 | 4,300 | 2,130 | 2,890 | 4,480 | 42,790 |
| Ontario | 1,000 | 8,300 | 28,400 | 68,630 | 3,170 | 11,960 | 16,320 | 11,810 | 6,240 | 6,180 | 89,580 |
| Manitoba | 100 | 740 | 2,410 | 8,450 | 260 | 720 | 940 | 840 | 700 | 590 | 10,870 |
| Saskatchewan | 90 | 660 | 1,500 | 4,690 | 230 | 680 | 850 | 600 | 720 | 500 | 6,880 |
| Alberta | 350 | 2,510 | 9,310 | 21,660 | 650 | 3,020 | 3,710 | 2,690 | 2,570 | 2,370 | 29,970 |
| British Columbia | 340 | 2,080 | 7,670 | 25,050 | 730 | 3,110 | 3,970 | 2,480 | 2,070 | 2,690 | 32,610 |
| Yukon | 10 | 20 | 50 | 130 | 10 | 20 | 30 | 20 | 20 | 20 | 210 |
| Northwest Territories | 0 | 20 | 90 | 170 | 0 | 20 | 20 | 20 | 20 | 20 | 240 |
| Nunavut | 10 | 30 | 50 | 60 | 10 | 30 | 30 | 20 | 10 | 10 | 110 |
| Missing | 30 | 150 | 340 | 1,240 | 40 | 170 | 200 | 140 | 40 | 60 | 1,420 |
| Outside Canada | 10 | 30 | 70 | 120 | 10 | 30 | 50 | 20 | 20 | 10 | 170 |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 20 | 130 | 210 | 780 | 60 | 120 | 180 | 120 | 190 | 30 | 1,140 |
| Prince Edward Island | 10 | 40 | 50 | 280 | 10 | 30 | 40 | 30 | 50 | 10 | 380 |
| Nova Scotia | 40 | 230 | 270 | 1,380 | 70 | 190 | 280 | 210 | 230 | 80 | 1,910 |
| New Brunswick | 40 | 200 | 280 | 1,020 | 70 | 180 | 230 | 180 | 210 | 50 | 1,480 |
| Quebec | 250 | 1,160 | 2,430 | 6,380 | 360 | 1,100 | 1,510 | 860 | 610 | 340 | 8,660 |
| Ontario | 580 | 3,070 | 4,760 | 15,910 | 1,120 | 2,850 | 4,260 | 2,900 | 1,960 | 720 | 21,300 |
| Manitoba | 60 | 320 | 450 | 2,240 | 150 | 270 | 410 | 320 | 170 | 60 | 2,840 |
| Saskatchewan | 40 | 290 | 330 | 1,210 | 80 | 180 | 310 | 240 | 180 | 60 | 1,720 |
| Alberta | 150 | 920 | 1,270 | 5,030 | 260 | 740 | 1,090 | 810 | 570 | 200 | 6,670 |
| British Columbia | 160 | 950 | 1,420 | 6,520 | 320 | 910 | 1,260 | 910 | 700 | 330 | 8,390 |
| Yukon | 0 | 10 | 10 | 40 | 0 | 10 | 10 | 10 | 0 | 0 | 50 |
| Northwest Territories | 0 | 10 | 10 | 40 | 0 | 10 | 10 | 0 | 0 | 0 | 50 |
| Nunavut | 0 | 10 | 20 | 20 | 10 | 10 | 10 | 10 | 0 | 0 | 40 |
| Missing | 20 | 60 | 90 | 300 | 20 | 50 | 80 | 60 | 10 | 0 | 340 |
| Outside Canada | 0 | 30 | 30 | 50 | 10 | 30 | 30 | 30 | 0 | 0 | 70 |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 50 | 400 | 270 | 860 | 90 | 200 | 310 | 260 | 350 | 50 | 1,690 |
| Prince Edward Island | 20 | 100 | 70 | 330 | 20 | 50 | 70 | 50 | 90 | 30 | 550 |
| Nova Scotia | 110 | 590 | 430 | 1,760 | 140 | 280 | 450 | 380 | 420 | 140 | 3,000 |
| New Brunswick | 80 | 420 | 350 | 1,240 | 130 | 250 | 360 | 330 | 280 | 70 | 2,090 |
| Quebec | 590 | 2,690 | 3,260 | 9,150 | 880 | 1,700 | 2,150 | 1,340 | 1,060 | 360 | 13,800 |
| Ontario | 1,450 | 6,620 | 6,610 | 22,100 | 2,060 | 4,350 | 6,230 | 4,400 | 3,370 | 1,240 | 33,770 |
| Manitoba | 160 | 740 | 550 | 2,720 | 240 | 390 | 590 | 460 | 390 | 190 | 4,270 |
| Saskatchewan | 120 | 610 | 420 | 1,490 | 170 | 320 | 480 | 390 | 350 | 110 | 2,660 |
| Alberta | 430 | 1,900 | 1,600 | 6,360 | 530 | 1,040 | 1,460 | 1,180 | 1,170 | 490 | 10,250 |
| British Columbia | 480 | 2,200 | 2,060 | 8,350 | 700 | 1,470 | 1,950 | 1,550 | 1,250 | 680 | 12,700 |
| Yukon | 0 | 20 | 10 | 50 | 0 | 10 | 10 | 10 | 10 | 10 | 80 |
| Northwest Territories | 0 | 20 | 20 | 80 | 0 | 10 | 20 | 10 | 10 | 0 | 110 |
| Nunavut | 0 | 10 | 10 | 20 | 0 | 10 | 10 | 10 | 0 | 0 | 40 |
| Missing | 30 | 120 | 110 | 330 | 30 | 80 | 110 | 80 | 20 | 10 | 440 |
| Outside Canada | 20 | 50 | 40 | 90 | 20 | 40 | 40 | 30 | 20 | 0 | 170 |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 90 | 620 | 210 | 740 | 140 | 180 | 340 | 260 | 440 | 160 | 2,140 |
| Prince Edward Island | 30 | 160 | 40 | 220 | 20 | 30 | 60 | 50 | 90 | 50 | 570 |
| Nova Scotia | 140 | 860 | 250 | 1,190 | 160 | 200 | 380 | 370 | 430 | 310 | 3,060 |
| New Brunswick | 120 | 700 | 210 | 1,090 | 150 | 180 | 340 | 330 | 330 | 220 | 2,580 |
| Quebec | 680 | 3,130 | 1,670 | 6,530 | 940 | 1,200 | 1,610 | 1,050 | 1,140 | 640 | 12,550 |
| Ontario | 1,530 | 8,560 | 3,440 | 14,920 | 1,880 | 2,800 | 4,840 | 3,370 | 3,150 | 2,530 | 31,170 |
| Manitoba | 150 | 1,160 | 280 | 1,900 | 180 | 280 | 500 | 370 | 470 | 340 | 4,170 |
| Saskatchewan | 140 | 760 | 230 | 1,090 | 160 | 190 | 370 | 310 | 360 | 210 | 2,630 |
| Alberta | 440 | 2,810 | 840 | 4,480 | 580 | 730 | 1,330 | 1,170 | 1,510 | 1,060 | 10,740 |
| British Columbia | 460 | 3,060 | 1,130 | 6,060 | 670 | 1,050 | 1,680 | 1,370 | 1,150 | 1,410 | 12,460 |
| Yukon | 0 | 20 | 10 | 40 | 0 | 10 | 10 | 10 | 10 | 10 | 90 |
| Northwest Territories | 10 | 20 | 10 | 50 | 0 | 10 | 20 | 10 | 10 | 0 | 90 |
| Nunavut | 0 | 10 | 10 | 20 | 0 | 0 | 10 | 0 | 10 | 0 | 40 |
| Missing | 20 | 70 | 40 | 140 | 20 | 20 | 30 | 20 | 0 | 0 | 230 |
| Outside Canada | 20 | 50 | 30 | 60 | 50 | 20 | 30 | 20 | 10 | 10 | 180 |
| - | - | - | - | - | - | - | - | - | - | - | - |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 130 | 1,410 | 210 | 850 | 220 | 230 | 680 | 370 | 680 | 420 | 3,820 |
| Prince Edward Island | 40 | 360 | 40 | 250 | 40 | 40 | 120 | 80 | 120 | 110 | 930 |
| Nova Scotia | 200 | 2,300 | 270 | 1,520 | 260 | 280 | 880 | 630 | 650 | 700 | 5,620 |
| New Brunswick | 160 | 1,630 | 260 | 1,210 | 270 | 280 | 660 | 490 | 610 | 480 | 4,330 |
| Quebec | 860 | 4,570 | 1,250 | 5,580 | 1,010 | 1,080 | 1,800 | 1,090 | 1,120 | 1,300 | 14,300 |
| Ontario | 1,890 | 17,300 | 3,010 | 14,930 | 2,280 | 3,000 | 7,380 | 4,370 | 4,110 | 5,180 | 44,370 |
| Manitoba | 190 | 2,390 | 280 | 1,900 | 270 | 310 | 930 | 560 | 640 | 680 | 6,200 |
| Saskatchewan | 160 | 1,260 | 230 | 930 | 160 | 210 | 480 | 390 | 470 | 390 | 3,350 |
| Alberta | 460 | 4,770 | 680 | 3,740 | 580 | 700 | 1,810 | 1,280 | 1,620 | 1,700 | 12,790 |
| British Columbia | 540 | 5,640 | 880 | 5,750 | 680 | 1,030 | 2,330 | 1,670 | 1,320 | 2,550 | 16,290 |
| Yukon | 0 | 30 | 0 | 20 | 10 | 10 | 10 | 10 | 10 | 10 | 90 |
| Northwest Territories | 10 | 40 | 0 | 30 | 10 | 10 | 20 | 10 | 10 | 10 | 110 |
| Nunavut | 0 | 10 | 0 | 10 | 10 | 0 | 10 | 0 | 10 | 0 | 50 |
| Missing | 10 | 20 | 10 | 70 | 0 | 10 | 10 | 0 | 0 | 0 | 100 |
| Outside Canada | 30 | 80 | 30 | 60 | 50 | 20 | 30 | 20 | 10 | 20 | 240 |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 180 | 3,210 | 240 | 960 | 390 | 310 | 1,280 | 580 | 1,010 | 870 | 6,760 |
| Prince Edward Island | 50 | 920 | 50 | 360 | 60 | 80 | 270 | 130 | 210 | 260 | 1,830 |
| Nova Scotia | 260 | 6,200 | 360 | 2,010 | 510 | 530 | 1,990 | 1,070 | 1,000 | 1,450 | 11,410 |
| New Brunswick | 240 | 4,160 | 380 | 1,570 | 530 | 520 | 1,450 | 760 | 810 | 890 | 8,110 |
| Quebec | 1,490 | 10,670 | 1,870 | 8,370 | 1,610 | 1,930 | 3,690 | 1,770 | 1,490 | 2,590 | 26,150 |
| Ontario | 3,080 | 44,410 | 3,890 | 20,050 | 3,640 | 5,310 | 16,240 | 7,320 | 5,790 | 10,510 | 84,920 |
| Manitoba | 330 | 6,610 | 380 | 2,590 | 520 | 610 | 2,170 | 930 | 940 | 1,270 | 12,360 |
| Saskatchewan | 210 | 3,220 | 260 | 1,280 | 250 | 350 | 1,010 | 620 | 650 | 810 | 6,400 |
| Alberta | 680 | 11,330 | 910 | 5,090 | 840 | 1,300 | 3,770 | 2,060 | 2,290 | 3,200 | 23,150 |
| British Columbia | 900 | 14,110 | 1,150 | 7,860 | 1,040 | 1,870 | 4,860 | 2,700 | 2,110 | 4,450 | 30,060 |
| Yukon | 10 | 80 | 10 | 30 | 10 | 20 | 30 | 20 | 20 | 30 | 180 |
| Northwest Territories | 10 | 70 | 10 | 30 | 10 | 10 | 30 | 20 | 20 | 30 | 190 |
| Nunavut | 0 | 30 | 0 | 10 | 10 | 10 | 10 | 0 | 0 | 10 | 60 |
| Missing | 0 | 20 | 10 | 50 | 0 | 10 | 10 | 0 | 0 | 10 | 90 |
| Outside Canada | 40 | 160 | 30 | 80 | 40 | 30 | 50 | 40 | 10 | 10 | 360 |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 490 | 6,810 | 450 | 1,910 | 1,120 | 820 | 2,810 | 1,190 | 1,300 | 1,020 | 12,300 |
| Prince Edward Island | 150 | 2,480 | 90 | 740 | 210 | 220 | 690 | 350 | 300 | 380 | 4,070 |
| Nova Scotia | 940 | 16,000 | 790 | 4,620 | 1,660 | 1,600 | 5,140 | 2,460 | 1,440 | 1,800 | 24,820 |
| New Brunswick | 760 | 10,110 | 710 | 3,590 | 1,940 | 1,320 | 3,560 | 1,780 | 1,190 | 1,170 | 17,510 |
| Quebec | 5,540 | 35,460 | 4,340 | 26,580 | 4,480 | 7,720 | 15,210 | 6,530 | 2,800 | 5,020 | 74,640 |
| Ontario | 13,020 | 172,530 | 10,290 | 63,190 | 16,450 | 22,760 | 64,280 | 28,820 | 10,100 | 20,060 | 265,480 |
| Manitoba | 1,430 | 26,130 | 890 | 7,370 | 1,890 | 2,330 | 8,130 | 3,350 | 1,420 | 2,570 | 38,470 |
| Saskatchewan | 940 | 11,520 | 570 | 4,040 | 1,050 | 1,160 | 3,440 | 1,920 | 1,000 | 1,540 | 18,540 |
| Alberta | 2,420 | 32,760 | 1,950 | 12,700 | 2,650 | 4,020 | 11,370 | 5,490 | 3,180 | 4,750 | 53,490 |
| British Columbia | 4,240 | 52,860 | 3,230 | 22,680 | 4,600 | 7,020 | 17,780 | 9,040 | 3,690 | 7,740 | 87,830 |
| Yukon | 20 | 190 | 10 | 60 | 20 | 20 | 60 | 40 | 20 | 40 | 330 |
| Northwest Territories | 20 | 150 | 20 | 60 | 10 | 20 | 60 | 30 | 10 | 30 | 270 |
| Nunavut | 10 | 30 | 10 | 10 | 10 | 0 | 10 | 0 | 0 | 10 | 50 |
| Missing | 30 | 140 | 20 | 110 | 20 | 50 | 80 | 30 | 0 | 10 | 250 |
| Outside Canada | 200 | 930 | 100 | 400 | 130 | 190 | 350 | 170 | 30 | 70 | 1,560 |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Prince Edward Island | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Nova Scotia | 0 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| New Brunswick | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Quebec | 10 | 20 | 10 | 20 | 0 | 10 | 10 | 10 | 0 | 0 | 50 |
| Ontario | 10 | 60 | 10 | 20 | 0 | 20 | 30 | 20 | 0 | 0 | 90 |
| Manitoba | 0 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Saskatchewan | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 10 |
| Alberta | 0 | 10 | 0 | 10 | 0 | 10 | 10 | 0 | 0 | 0 | 20 |
| British Columbia | 0 | 20 | 0 | 10 | 0 | 10 | 10 | 0 | 0 | 0 | 30 |
| Outside Canada | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 53,770 | 579,860 | 146,640 | 538,460 | 70,400 | 117,670 | 255,210 | 138,490 | 93,820 | 116,260 | 1,380,180 |
Percentage of individuals with an accepted DTC certificate by age group
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador |
1.9% | 1.5% | 1.3% | 1.7% | 1.7% | 1.5% | 1.6% | 1.4% | 2.4% | 1.1% | 1.6% |
| Prince Edward Island | 0.4% | 0.4% | 0.2% | 0.5% | 0.3% | 0.2% | 0.3% | 0.3% | 0.7% | 0.3% | 0.5% |
| Nova Scotia | 2.3% | 2.4% | 1.8% | 3.2% | 2.4% | 2.2% | 2.5% | 2.3% | 3.7% | 2.1% | 3.0% |
| New Brunswick | 2.6% | 2.4% | 2.4% | 2.6% | 2.2% | 2.2% | 2.7% | 3.1% | 2.5% | 1.8% | 2.5% |
| Quebec | 19.6% | 15.9% | 23.7% | 14.7% | 12.8% | 13.3% | 13.1% | 9.5% | 17.1% | 25.0% | 18.4% |
| Ontario | 37.7% | 44.2% | 40.2% | 40.7% | 50.0% | 48.7% | 49.9% | 52.8% | 37.0% | 34.5% | 38.5% |
| Manitoba | 3.8% | 3.9% | 3.4% | 5.0% | 4.1% | 2.9% | 2.9% | 3.8% | 4.1% | 3.3% | 4.7% |
| Saskatchewan | 3.4% | 3.5% | 2.1% | 2.8% | 3.6% | 2.8% | 2.6% | 2.7% | 4.3% | 2.8% | 3.0% |
| Alberta | 13.2% | 13.4% | 13.2% | 12.9% | 10.3% | 12.3% | 11.3% | 12.0% | 15.2% | 13.2% | 12.9% |
| British Columbia | 12.8% | 11.1% | 10.9% | 14.9% | 11.5% | 12.7% | 12.1% | 11.1% | 12.3% | 15.0% | 14.0% |
| Yukon | 0.4% | 0.1% | 0.1% | 0.1% | 0.2% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Northwest Territories |
- | 0.1% | 0.1% | 0.1% | - | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Nunavut | 0.4% | 0.2% | 0.1% | 0.0% | 0.2% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.0% |
| Unspecified | 1.1% | 0.8% | 0.5% | 0.7% | 0.6% | 0.7% | 0.6% | 0.6% | 0.2% | 0.3% | 0.6% |
| Outside Canada | 0.4% | 0.2% | 0.1% | 0.1% | 0.2% | 0.1% | 0.2% | 0.1% | 0.1% | 0.1% | 0.1% |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 1.5% | 1.7% | 1.8% | 1.9% | 2.4% | 1.8% | 1.9% | 1.8% | 3.9% | 1.6% | 2.1% |
| Prince Edward Island | 0.7% | 0.5% | 0.4% | 0.7% | 0.4% | 0.4% | 0.4% | 0.4% | 1.0% | 0.5% | 0.7% |
| Nova Scotia | 2.9% | 3.1% | 2.3% | 3.3% | 2.8% | 2.8% | 2.9% | 3.1% | 4.7% | 4.3% | 3.5% |
| New Brunswick | 2.9% | 2.7% | 2.4% | 2.5% | 2.8% | 2.7% | 2.4% | 2.7% | 4.3% | 2.7% | 2.7% |
| Quebec | 18.2% | 15.6% | 20.9% | 15.5% | 14.2% | 16.5% | 15.6% | 12.9% | 12.5% | 18.1% | 15.7% |
| Ontario | 42.3% | 41.3% | 40.9% | 38.6% | 44.1% | 42.7% | 43.9% | 43.3% | 40.2% | 38.3% | 38.7% |
| Manitoba | 4.4% | 4.3% | 3.9% | 5.4% | 5.9% | 4.0% | 4.2% | 4.8% | 3.5% | 3.2% | 5.2% |
| Saskatchewan | 2.9% | 3.9% | 2.8% | 2.9% | 3.1% | 2.7% | 3.2% | 3.6% | 3.7% | 3.2% | 3.1% |
| Alberta | 10.9% | 12.4% | 10.9% | 12.2% | 10.2% | 11.1% | 11.2% | 12.1% | 11.7% | 10.6% | 12.1% |
| British Columbia | 11.7% | 12.8% | 12.2% | 15.8% | 12.6% | 13.6% | 13.0% | 13.6% | 14.3% | 17.6% | 15.2% |
| Yukon | - | 0.1% | 0.1% | 0.1% | - | 0.1% | 0.1% | 0.1% | - | - | 0.1% |
| Northwest Territories | - | 0.1% | 0.1% | 0.1% | - | 0.1% | 0.1% | - | - | - | 0.1% |
| Nunavut | - | 0.1% | 0.2% | 0.0% | 0.4% | 0.1% | 0.1% | 0.1% | - | - | 0.1% |
| Unspecified | 1.5% | 0.8% | 0.8% | 0.7% | 0.4% | 0.7% | 0.8% | 0.9% | 0.2% | - | 0.6% |
| Outside Canada | - | 0.4% | 0.3% | 0.1% | 0.4% | 0.4% | 0.3% | 0.4% | - | - | 0.1% |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 1.4% | 2.4% | 1.7% | 1.6% | 1.8% | 2.0% | 2.2% | 2.5% | 4.0% | 1.5% | 2.0% |
| Prince Edward Island | 0.6% | 0.6% | 0.4% | 0.6% | 0.4% | 0.5% | 0.5% | 0.5% | 1.0% | 0.9% | 0.6% |
| Nova Scotia | 3.1% | 3.6% | 2.7% | 3.2% | 2.8% | 2.7% | 3.2% | 3.6% | 4.8% | 4.1% | 3.5% |
| New Brunswick | 2.3% | 2.5% | 2.2% | 2.3% | 2.6% | 2.5% | 2.5% | 3.1% | 3.2% | 2.1% | 2.4% |
| Quebec | 16.7% | 16.3% | 20.6% | 16.7% | 17.6% | 16.7% | 15.1% | 12.8% | 12.1% | 10.7% | 16.1% |
| Ontario | 41.0% | 40.1% | 41.8% | 40.2% | 41.1% | 42.6% | 43.8% | 42.0% | 38.3% | 36.7% | 39.4% |
| Manitoba | 4.5% | 4.5% | 3.5% | 5.0% | 4.8% | 3.8% | 4.1% | 4.4% | 4.4% | 5.6% | 5.0% |
| Saskatchewan | 3.4% | 3.7% | 2.7% | 2.7% | 3.4% | 3.1% | 4.1% | 3.7% | 4.0% | 3.3% | 3.1% |
| Alberta | 12.1% | 11.5% | 10.1% | 11.6% | 10.6% | 10.2% | 10.3% | 11.3% | 13.3% | 14.5% | 12.0% |
| British Columbia | 13.6% | 13.3% | 13.0% | 15.2% | 14.0% | 14.4% | 13.7% | 14.8% | 14.2% | 20.1% | 14.8% |
| Yukon | - | 0.1% | 0.1% | 0.1% | - | 0.1% | 0.1% | 0.1% | 0.1% | 0.3% | 0.1% |
| Northwest Territories | - | 0.1% | 0.1% | 0.1% | - | 0.1% | 0.1% | 0.1% | 0.1% | - | 0.1% |
| Nunavut | - | 0.1% | 0.1% | 0.0% | - | 0.1% | 0.1% | 0.1% | - | - | 0.0% |
| Unspecified | 0.8% | 0.7% | 0.7% | 0.6% | 0.6% | 0.8% | 0.8% | 0.8% | 0.2% | 0.3% | 0.5% |
| Outside Canada | 0.6% | 0.3% | 0.3% | 0.2% | 0.4% | 0.4% | 0.3% | 0.3% | 0.2% | - | 0.2% |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 2.3% | 2.8% | 2.5% | 1.9% | 2.8% | 2.6% | 2.9% | 3.0% | 4.8% | 2.3% | 2.6% |
| Prince Edward Island | 0.8% | 0.7% | 0.5% | 0.6% | 0.4% | 0.4% | 0.5% | 0.6% | 1.0% | 0.7% | 0.7% |
| Nova Scotia | 3.7% | 3.9% | 3.0% | 3.1% | 3.2% | 2.9% | 3.3% | 4.2% | 4.7% | 4.5% | 3.7% |
| New Brunswick | 3.1% | 3.2% | 2.5% | 2.8% | 3.0% | 2.6% | 2.9% | 3.8% | 3.6% | 3.2% | 3.1% |
| Quebec | 17.8% | 14.2% | 19.9% | 16.9% | 19.0% | 17.4% | 13.9% | 12.1% | 12.5% | 9.2% | 15.2% |
| Ontario | 39.9% | 38.9% | 41.0% | 38.7% | 38.0% | 40.6% | 41.9% | 38.7% | 34.6% | 36.4% | 37.7% |
| Manitoba | 3.9% | 5.3% | 3.3% | 4.9% | 3.6% | 4.1% | 4.3% | 4.2% | 5.2% | 4.9% | 5.0% |
| Saskatchewan | 3.7% | 3.5% | 2.7% | 2.8% | 3.2% | 2.8% | 3.2% | 3.6% | 4.0% | 3.0% | 3.2% |
| Alberta | 11.5% | 12.8% | 10.0% | 11.6% | 11.7% | 10.6% | 11.5% | 13.4% | 16.6% | 15.3% | 13.0% |
| British Columbia | 12.0% | 13.9% | 13.5% | 15.7% | 13.5% | 15.2% | 14.5% | 15.7% | 12.6% | 20.3% | 15.1% |
| Yukon | - | 0.1% | 0.1% | 0.1% | - | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Northwest Territories | 0.3% | 0.1% | 0.1% | 0.1% | - | 0.1% | 0.2% | 0.1% | 0.1% | - | 0.1% |
| Nunavut | - | 0.0% | 0.1% | 0.1% | - | - | 0.1% | - | 0.1% | - | 0.0% |
| Unspecified | 0.5% | 0.3% | 0.5% | 0.4% | 0.4% | 0.3% | 0.3% | 0.2% | - | - | 0.3% |
| Outside Canada | 0.5% | 0.2% | 0.4% | 0.2% | 1.0% | 0.3% | 0.3% | 0.2% | 0.1% | 0.1% | 0.2% |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 2.8% | 3.4% | 2.9% | 2.3% | 3.8% | 3.2% | 4.0% | 3.4% | 6.0% | 3.1% | 3.4% |
| Prince Edward Island | 0.9% | 0.9% | 0.6% | 0.7% | 0.7% | 0.6% | 0.7% | 0.7% | 1.1% | 0.8% | 0.8% |
| Nova Scotia | 4.3% | 5.5% | 3.8% | 4.1% | 4.4% | 3.9% | 5.1% | 5.7% | 5.7% | 5.2% | 5.0% |
| New Brunswick | 3.4% | 3.9% | 3.6% | 3.3% | 4.6% | 3.9% | 3.8% | 4.5% | 5.4% | 3.5% | 3.8% |
| Quebec | 18.4% | 10.9% | 17.5% | 15.1% | 17.3% | 15.0% | 10.5% | 9.9% | 9.8% | 9.6% | 12.7% |
| Ontario | 40.4% | 41.4% | 42.1% | 40.5% | 39.0% | 41.6% | 43.0% | 39.8% | 36.1% | 38.2% | 39.4% |
| Manitoba | 4.1% | 5.7% | 3.9% | 5.2% | 4.6% | 4.3% | 5.4% | 5.1% | 5.6% | 5.0% | 5.5% |
| Saskatchewan | 3.4% | 3.0% | 3.2% | 2.5% | 2.7% | 2.9% | 2.8% | 3.6% | 4.1% | 2.9% | 3.0% |
| Alberta | 9.8% | 11.4% | 9.5% | 10.1% | 9.9% | 9.7% | 10.6% | 11.7% | 14.2% | 12.5% | 11.4% |
| British Columbia | 11.5% | 13.5% | 12.3% | 15.6% | 11.6% | 14.3% | 13.6% | 15.2% | 11.6% | 18.8% | 14.5% |
| Yukon | - | 0.1% | - | 0.1% | 0.2% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Northwest Territories | 0.2% | 0.1% | - | 0.1% | 0.2% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Nunavut | - | 0.0% | - | 0.0% | 0.2% | - | 0.1% | - | 0.1% | - | 0.0% |
| Unspecified | 0.2% | 0.0% | 0.1% | 0.2% | - | 0.1% | 0.1% | - | - | - | 0.1% |
| Outside Canada | 0.6% | 0.2% | 0.4% | 0.2% | 0.9% | 0.3% | 0.2% | 0.2% | 0.1% | 0.1% | 0.2% |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 2.4% | 3.1% | 2.5% | 1.9% | 4.1% | 2.4% | 3.5% | 3.2% | 6.2% | 3.3% | 3.2% |
| Prince Edward Island | 0.7% | 0.9% | 0.5% | 0.7% | 0.6% | 0.6% | 0.7% | 0.7% | 1.3% | 1.0% | 0.9% |
| Nova Scotia | 3.5% | 5.9% | 3.8% | 4.0% | 5.4% | 4.1% | 5.4% | 5.9% | 6.1% | 5.5% | 5.4% |
| New Brunswick | 3.2% | 4.0% | 4.0% | 3.1% | 5.6% | 4.0% | 3.9% | 4.2% | 5.0% | 3.4% | 3.8% |
| Quebec | 19.9% | 10.1% | 19.6% | 16.6% | 17.0% | 15.0% | 10.0% | 9.8% | 9.1% | 9.8% | 12.3% |
| Ontario | 41.2% | 42.2% | 40.7% | 39.8% | 38.5% | 41.2% | 44.1% | 40.6% | 35.4% | 39.8% | 40.1% |
| Manitoba | 4.4% | 6.3% | 4.0% | 5.1% | 5.5% | 4.7% | 5.9% | 5.2% | 5.7% | 4.8% | 5.8% |
| Saskatchewan | 2.8% | 3.1% | 2.7% | 2.5% | 2.6% | 2.7% | 2.7% | 3.4% | 4.0% | 3.1% | 3.0% |
| Alberta | 9.1% | 10.8% | 9.5% | 10.1% | 8.9% | 10.1% | 10.2% | 11.4% | 14.0% | 12.1% | 10.9% |
| British Columbia | 12.0% | 13.4% | 12.0% | 15.6% | 11.0% | 14.5% | 13.2% | 15.0% | 12.9% | 16.9% | 14.2% |
| Yukon | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.2% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Northwest Territories | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% |
| Nunavut | - | 0.0% | - | 0.0% | 0.1% | 0.1% | 0.0% | - | - | 0.0% | 0.0% |
| Unspecified | - | 0.0% | 0.1% | 0.1% | - | 0.1% | 0.0% | - | - | 0.0% | 0.0% |
| Outside Canada | 0.5% | 0.2% | 0.3% | 0.2% | 0.4% | 0.2% | 0.1% | 0.2% | 0.1% | 0.0% | 0.2% |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | 1.6% | 1.9% | 1.9% | 1.3% | 3.1% | 1.7% | 2.1% | 1.9% | 4.9% | 2.2% | 2.1% |
| Prince Edward Island | 0.5% | 0.7% | 0.4% | 0.5% | 0.6% | 0.4% | 0.5% | 0.6% | 1.1% | 0.8% | 0.7% |
| Nova Scotia | 3.1% | 4.3% | 3.4% | 3.1% | 4.6% | 3.2% | 3.9% | 4.0% | 5.4% | 3.9% | 4.1% |
| New Brunswick | 2.5% | 2.7% | 3.0% | 2.4% | 5.4% | 2.7% | 2.7% | 2.9% | 4.5% | 2.5% | 2.9% |
| Quebec | 18.3% | 9.6% | 18.5% | 18.0% | 12.4% | 15.7% | 11.4% | 10.7% | 10.6% | 10.9% | 12.4% |
| Ontario | 43.1% | 46.9% | 43.8% | 42.7% | 12.4% | 46.2% | 48.3% | 47.1% | 38.1% | 43.4% | 44.3% |
| Manitoba | 4.7% | 7.1% | 3.8% | 5.0% | 5.2% | 4.7% | 6.1% | 5.5% | 5.4% | 5.6% | 6.4% |
| Saskatchewan | 3.1% | 3.1% | 2.4% | 2.7% | 2.9% | 2.4% | 2.6% | 3.1% | 3.8% | 3.3% | 3.1% |
| Alberta | 8.0% | 8.9% | 8.3% | 8.6% | 2.9% | 8.2% | 8.6% | 9.0% | 12.0% | 10.3% | 8.9% |
| British Columbia | 14.0% | 14.4% | 13.8% | 15.3% | 12.7% | 14.3% | 13.4% | 14.8% | 13.9% | 16.7% | 14.6% |
| Yukon | 0.1% | 0.1% | 0.0% | 0.0% | 0.1% | 0.0% | 0.0% | 0.1% | 0.1% | 0.1% | 0.1% |
| Northwest Territories | 0.1% | 0.0% | 0.1% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.1% | 0.0% |
| Nunavut | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | - | 0.0% | - | - | 0.0% | 0.0% |
| Unspecified | 0.1% | 0.0% | 0.1% | 0.1% | 0.1% | 0.1% | 0.1% | 0.0% | - | 0.0% | 0.0% |
| Outside Canada | 0.7% | 0.0% | 0.4% | 0.3% | 0.4% | 0.4% | 0.3% | 0.3% | 0.1% | 0.2% | 0.3% |
| Province/ Territory |
Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total Unique Certificates |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Newfoundland and Labrador | - | - | - | - | - | - | - | - | - | - | - |
| Prince Edward Island | - | - | - | - | - | - | - | - | - | - | - |
| Nova Scotia | - | 7.7% | - | - | - | - | - | - | - | - | 4.5% |
| New Brunswick | - | - | - | - | - | - | - | - | - | - | - |
| Quebec | 50.0% | 15.4% | 50.0% | 33.3% | - | 20.0% | 16.7% | 33.3% | - | - | 22.7% |
| Ontario | 50.0% | 46.2% | 50.0% | 33.3% | - | 40.0% | 50.0% | 66.7% | - | - | 40.9% |
| Manitoba | - | 7.7% | - | - | - | - | - | - | - | - | 4.5% |
| Saskatchewan | - | - | - | - | - | - | - | - | - | - | 4.5% |
| Alberta | - | 7.7% | - | 16.7% | - | 20.0% | 16.7% | - | - | - | 9.1% |
| British Columbia | - | 15.4% | - | 16.7% | - | 20.0% | 16.7% | - | - | - | 13.6% |
| Yukon | - | - | - | - | - | - | - | - | - | - | - |
| Northwest Territories | - | - | - | - | - | - | - | - | - | - | - |
| Nunavut | - | - | - | - | - | - | - | - | - | - | - |
| Unspecified | - | - | - | - | - | - | - | - | - | - | - |
| Outside Canada | - | - | - | - | - | - | - | - | - | - | - |
Statistics by BADL, 2011-2020
Table 12 – DTC determinations
This table presents the DTC determinations of individuals broken down by BADL. For individuals with a determination that contains both accepted and rejected restrictions, only the accepted restrictions are counted. Therefore, the rejected restrictions contained in accepted certificates are not counted. Caution should be exercised when interpreting the acceptance/rejection rate at the BADL level. Please refer to the "DTC determination" description in the "Description of DTC items" section of the explanatory notes for more information.Footnote 16
Number of DTC determintions by status
| Year | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020 | 3,760 | 86,080 | 18,640 | 78,840 | 6,420 | 17,310 | 38,690 | 23,070 | 18,060 | 24,900 | 315,770 | 203,370 |
| 2019 | 4,560 | 91,210 | 20,860 | 82,410 | 6,720 | 18,990 | 41,580 | 24,160 | 17,100 | 24,310 | 331,910 | 210,200 |
| 2018 | 4,930 | 90,920 | 20,500 | 79,270 | 6,920 | 19,430 | 41,520 | 24,690 | 18,480 | 23,540 | 330,200 | 205,890 |
| 2017 | 4,010 | 81,100 | 16,440 | 65,710 | 6,320 | 16,110 | 36,120 | 19,930 | 12,760 | 18,070 | 276,570 | 173,460 |
| 2016 | 4,460 | 91,620 | 18,430 | 75,460 | 7,650 | 19,080 | 42,360 | 22,740 | 13,060 | 21,490 | 316,350 | 195,360 |
| 2015 | 4,780 | 94,770 | 17,600 | 79,000 | 8,110 | 19,410 | 44,730 | 22,470 | 11,560 | 20,650 | 323,080 | 198,310 |
| 2014 | 5,370 | 91,230 | 18,160 | 76,600 | 8,510 | 20,740 | 44,450 | 22,490 | 10,910 | 18,860 | 317,300 | 190,030 |
| 2013 | 6,370 | 88,620 | 17,960 | 77,170 | 8,650 | 22,210 | 44,140 | 23,090 | 10,070 | 17,060 | 315,340 | 185,020 |
| 2012 | 5,670 | 86,230 | 17,750 | 71,740 | 8,290 | 20,450 | 42,260 | 21,630 | 10,430 | 14,840 | 299,300 | 183,310 |
| 2011 | 5,980 | 85,750 | 16,780 | 66,870 | 8,510 | 21,500 | 43,430 | 23,080 | 10,040 | 12,900 | 294,830 | 168,230 |
| Year | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020 | 430 | 2,400 | 710 | 8,600 | 720 | 520 | 830 | 920 | 1,340 | 1,380 | 17,830 | 16,870 |
| 2019 | 510 | 4,500 | 1,190 | 13,760 | 1,120 | 910 | 1,640 | 1,490 | 1,680 | 2,170 | 28,950 | 26,360 |
| 2018 | 540 | 5,850 | 1,780 | 17,340 | 1,350 | 1,140 | 2,150 | 2,090 | 1,790 | 2,410 | 36,440 | 32,680 |
| 2017 | 670 | 7,340 | 1,740 | 18,480 | 1,490 | 1,200 | 2,520 | 2,370 | 2,300 | 2,620 | 40,720 | 36,260 |
| 2016 | 650 | 5,480 | 1,130 | 13,480 | 1,100 | 850 | 1,760 | 1,490 | 1,720 | 2,110 | 29,780 | 27,610 |
| 2015 | 520 | 4,160 | 740 | 9,520 | 830 | 550 | 1,260 | 920 | 1,310 | 1,690 | 21,490 | 20,590 |
| 2014 | 540 | 5,360 | 620 | 8,920 | 760 | 580 | 1,460 | 1,090 | 1,240 | 1,450 | 22,030 | 20,870 |
| 2013 | 570 | 6,080 | 720 | 9,970 | 800 | 550 | 1,660 | 1,290 | 1,220 | 1,330 | 24,200 | 22,800 |
| 2012 | 460 | 6,150 | 690 | 10,050 | 780 | 520 | 1,640 | 1,210 | 1,310 | 1,250 | 24,060 | 22,580 |
| 2011 | 500 | 5,080 | 600 | 8,710 | 600 | 530 | 1,370 | 940 | 1,130 | 920 | 20,380 | 19,570 |
| Year | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020 | 4,190 | 88,480 | 19,350 | 87,440 | 7,140 | 17,820 | 39,520 | 23,990 | 19,400 | 26,280 | 333,600 | 220,240 |
| 2019 | 5,070 | 95,700 | 22,050 | 96,170 | 7,840 | 19,910 | 43,220 | 25,650 | 18,780 | 26,480 | 360,860 | 236,560 |
| 2018 | 5,470 | 96,770 | 22,280 | 96,610 | 8,270 | 20,570 | 43,680 | 26,780 | 20,270 | 25,950 | 366,640 | 238,570 |
| 2017 | 4,680 | 88,430 | 18,180 | 84,190 | 7,810 | 17,310 | 38,630 | 22,290 | 15,060 | 20,690 | 317,290 | 209,720 |
| 2016 | 5,110 | 97,100 | 19,560 | 88,940 | 8,760 | 19,940 | 44,120 | 24,220 | 14,780 | 23,600 | 346,130 | 222,970 |
| 2015 | 5,300 | 98,930 | 18,340 | 88,520 | 8,940 | 19,960 | 46,000 | 23,390 | 12,870 | 22,340 | 344,570 | 218,890 |
| 2014 | 5,900 | 96,590 | 18,790 | 85,520 | 9,270 | 21,310 | 45,910 | 23,580 | 12,150 | 20,310 | 339,330 | 210,900 |
| 2013 | 6,930 | 94,700 | 18,680 | 87,140 | 9,450 | 22,770 | 45,800 | 24,380 | 11,290 | 18,390 | 339,540 | 207,810 |
| 2012 | 6,130 | 92,390 | 18,440 | 81,800 | 9,070 | 20,970 | 43,900 | 22,840 | 11,740 | 16,090 | 323,360 | 205,890 |
| 2011 | 6,480 | 90,830 | 17,370 | 75,580 | 9,110 | 22,030 | 44,790 | 24,020 | 11,180 | 13,820 | 315,210 | 187,810 |
Percentage of DTC determintions by status
| Year | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020 | 89.7% | 97.3% | 96.3% | 90.2% | 89.9% | 97.1% | 97.9% | 96.2% | 93.1% | 94.7% | 94.7% |
| 2019 | 89.9% | 95.3% | 94.6% | 85.7% | 85.7% | 95.4% | 96.2% | 94.2% | 91.1% | 91.8% | 92.0% |
| 2018 | 90.1% | 94.0% | 92.0% | 82.1% | 83.7% | 94.5% | 95.1% | 92.2% | 91.2% | 90.7% | 90.1% |
| 2017 | 85.7% | 91.7% | 90.4% | 78.0% | 80.9% | 93.1% | 93.5% | 89.4% | 84.7% | 87.3% | 87.2% |
| 2016 | 87.3% | 94.4% | 94.2% | 84.8% | 87.3% | 95.7% | 96.0% | 93.9% | 88.4% | 91.1% | 91.4% |
| 2015 | 90.2% | 95.8% | 96.0% | 89.2% | 90.7% | 97.2% | 97.2% | 96.1% | 89.8% | 92.4% | 93.8% |
| 2014 | 91.0% | 94.5% | 96.6% | 89.6% | 91.8% | 97.3% | 96.8% | 95.4% | 89.8% | 92.9% | 93.5% |
| 2013 | 91.9% | 93.6% | 96.1% | 88.6% | 91.5% | 97.5% | 96.4% | 94.7% | 89.2% | 92.8% | 92.9% |
| 2012 | 92.5% | 93.3% | 96.3% | 87.7% | 91.4% | 97.5% | 96.3% | 94.7% | 88.8% | 92.2% | 92.6% |
| 2011 | 92.3% | 94.4% | 96.6% | 88.5% | 8.6% | 97.6% | 97.0% | 96.1% | 89.8% | 93.3% | 93.5% |
| Year | Vision | Walking | Speaking | Mental Functions |
Hearing | Feeding | Dressing | Eliminating | Life-Sustaining Therapy | Cumulative | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2020 | 10.3% | 2.7% | 3.7% | 9.8% | 10.1% | 2.9% | 2.1% | 3.8% | 6.9% | 5.3% | 5.3% |
| 2019 | 10.1% | 4.7% | 5.4% | 14.3% | 14.3% | 4.6% | 3.8% | 5.8% | 8.9% | 8.2% | 8.0% |
| 2018 | 9.9% | 6.0% | 8.0% | 17.9% | 16.3% | 5.5% | 4.9% | 7.8% | 8.8% | 9.3% | 9.9% |
| 2017 | 14.3% | 8.3% | 9.6% | 22.0% | 19.1% | 6.9% | 6.5% | 10.6% | 15.3% | 12.7% | 12.8% |
| 2016 | 12.7% | 5.6% | 5.8% | 15.2% | 12.6% | 9 4.3% | 4.0% | 6.2% | 11.6% | 8.9% | 8.6% |
| 2015 | 9.8% | 4.2% | 4.0% | 10.8% | 9.3% | 2.8% | 2.7% | 3.9% | 10.2% | 7.6% | 6.2% |
| 2014 | 9.2% | 5.5% | 3.3% | 10.4% | 8.2% | 2.7% | 3.2% | 4.6% | 10.2% | 7.1% | 6.5% |
| 2013 | 8.2% | 6.4% | 3.9% | 11.4% | 8.5% | 2.4% | 3.6% | 5.3% | 10.8% | 7.2% | 7.1% |
| 2012 | 7.5% | 6.7% | 3.7% | 12.3% | 8.6% | 2.5% | 3.7% | 5.3% | 11.2% | 7.8% | 7.4% |
| 2011 | 7.7% | 5.6% | 3.5% | 11.5% | 6.6% | 2.4% | 3.1% | 3.9% | 10.1% | 6.7% | 6.5% |
Table 13 – DTC claimants benefitting through a tax reduction
This table presents the number of DTC claimants benefitting through a tax reduction, broken down by BADL. The number of claimants benefitting through a tax reduction for each BADL is derived by multiplying both the total "Number of Claimants" by the share of accepted DTC determinations by BADL published in Table 11. For more information, please refer to the description of "Number of claimants benefitting through a tax reduction" in the "Description of DTC items" section of the explanatory notes.Footnote 17
| Basic activity of daily living (BADL) |
2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|
| Vision | 12,290 | 12,210 | 13,560 | 11,930 | 10,990 | 11,240 | 11,480 | 12,610 | 11,920 | 10,480 |
| Walking | 176,240 | 185,760 | 188,860 | 202,930 | 218,020 | 231,090 | 231,950 | 232,320 | 238,380 | 239,830 |
| Speaking | 34,480 | 38,230 | 38,280 | 40,400 | 40,500 | 46,490 | 47,030 | 52,380 | 54,530 | 51,930 |
| Mental Functions | 137,450 | 154,550 | 164,470 | 170,400 | 181,740 | 190,330 | 187,950 | 202,540 | 215,390 | 219,650 |
| Hearing | 17,490 | 17,870 | 18,430 | 18,920 | 18,650 | 19,310 | 18,070 | 17,670 | 17,560 | 17,890 |
| Feeding | 44,190 | 44,040 | 47,340 | 46,130 | 44,660 | 48,130 | 46,080 | 49,650 | 49,640 | 48,220 |
| Dressing | 89,260 | 91,040 | 94,060 | 98,880 | 102,910 | 106,850 | 103,310 | 106,100 | 108,670 | 107,800 |
| Eliminating | 47,440 | 46,600 | 49,210 | 50,020 | 51,690 | 57,350 | 57,000 | 63,090 | 63,140 | 64,270 |
| Life-Sustaining Therapy | 20,640 | 22,470 | 21,460 | 24,260 | 26,600 | 32,930 | 36,490 | 47,210 | 44,700 | 50,320 |
| Cumulative | 26,510 | 31,970 | 36,360 | 41,950 | 47,490 | 54,210 | 51,680 | 60,150 | 63,540 | 69,370 |
| Total | 605,980 | 644,740 | 672,030 | 705,840 | 743,250 | 797,930 | 791,040 | 843,720 | 867,470 | 879,760 |
| Basic activity of daily living (BADL) |
2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|
| Vision | 2.0% | 1.9% | 2.0% | 1.7% | 1.5% | 1.4% | 1.5% | 1.5% | 1.4% | 1.2% |
| Walking | 29.1% | 28.8% | 28.1% | 28.8% | 29.3% | 29.0% | 29.3% | 27.5% | 27.5% | 27.3% |
| Speaking | 5.7% | 5.9% | 5.7% | 5.7% | 5.4% | 5.8% | 5.9% | 6.2% | 6.3% | 5.9% |
| Mental Functions | 22.7% | 24.0% | 24.5% | 24.1% | 24.5% | 23.9% | 23.8% | 24.0% | 24.8% | 25.0% |
| Hearing | 2.9% | 2.8% | 2.7% | 2.7% | 2.5% | 2.4% | 2.3% | 2.1% | 2.0% | 2.0% |
| Feeding | 7.3% | 6.8% | 7.0% | 6.5% | 6.0% | 6.0% | 5.8% | 5.9% | 5.7% | 5.5% |
| Dressing | 14.7% | 14.1% | 14.0% | 14.0% | 13.8% | 13.4% | 13.1% | 12.6% | 12.5% | 12.3% |
| Eliminating | 7.8% | 7.2% | 7.3% | 7.1% | 7.0% | 7.2% | 7.2% | 7.5% | 7.3% | 7.3% |
| Life-Sustaining Therapy | 3.4% | 3.5% | 3.2% | 3.4% | 3.6% | 4.1% | 4.6% | 5.6% | 5.2% | 5.7% |
| Cumulative | 4.4% | 5.0% | 5.4% | 5.9% | 6.4% | 6.8% | 6.5% | 7.1% | 7.3% | 7.9% |
| Total | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
Table 14 – DTC utilization
This table presents the dollar amount of DTC utilized by claimants broken down by BADL. The total amount of DTC utilized for each BADL is derived by multiplying both the "Total Amount of DTC Utilized" by the share of accepted DTC determinations by BADL published in Table 11. For more information, please refer to the description of "Total Amount of DTC Utilized" in the "Description of DTC items" section of the explanatory notes. Footnote 18
DTC utilization by number
| Basic activity of daily living (BADL) |
2011 | 2012 | 2013 | 2014 | 2015 |
|---|---|---|---|---|---|
| Vision | 17,028,000 | 17,408,000 | 19,746,000 | 17,957,000 | 16,496,000 |
| Walking | 244,126,000 | 264,755,000 | 274,926,000 | 305,342,000 | 327,262,000 |
| Speaking | 47,759,000 | 54,481,000 | 55,725,000 | 60,787,000 | 60,786,000 |
| Mental Functions | 190,388,000 | 220,270,000 | 239,412,000 | 256,390,000 | 272,796,000 |
| Hearing | 24,228,000 | 25,464,000 | 26,828,000 | 28,471,000 | 27,988,000 |
| Feeding | 61,209,000 | 62,771,000 | 68,913,000 | 69,413,000 | 67,039,000 |
| Dressing | 123,636,000 | 129,757,000 | 136,920,000 | 148,783,000 | 154,473,000 |
| Eliminating | 65,710,000 | 66,412,000 | 71,631,000 | 75,270,000 | 77,596,000 |
| Life-Sustaining Therapy | 28,593,000 | 32,022,000 | 31,246,000 | 36,504,000 | 39,932,000 |
| Cumulative | 36,718,000 | 45,568,000 | 52,924,000 | 63,124,000 | 71,290,000 |
| Total | 839,396,000 | 918,909,000 | 978,271,000 | 1,062,041,000 | 1,115,658,000 |
| Basic activity of daily living (BADL) |
2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|
| Vision | 17,236,000 | 16,154,000 | 20,710,000 | 18,582,000 | 16,554,000 |
| Walking | 354,399,000 | 326,523,000 | 381,650,000 | 371,511,000 | 378,998,000 |
| Speaking | 71,290,000 | 66,210,000 | 86,040,000 | 84,977,000 | 82,065,000 |
| Mental Functions | 291,886,000 | 264,588,000 | 332,728,000 | 335,678,000 | 347,096,000 |
| Hearing | 29,607,000 | 25,439,000 | 29,026,000 | 27,372,000 | 28,278,000 |
| Feeding | 73,816,000 | 64,870,000 | 81,562,000 | 77,368,000 | 76,197,000 |
| Dressing | 163,862,000 | 145,430,000 | 174,297,000 | 169,367,000 | 170,347,000 |
| Eliminating | 87,954,000 | 80,235,000 | 103,641,000 | 98,402,000 | 101,565,000 |
| Life-Sustaining Therapy | 50,506,000 | 51,373,000 | 77,553,000 | 69,657,000 | 79,512,000 |
| Cumulative | 83,142,000 | 72,757,000 | 98,805,000 | 99,029,000 | 109,622,000 |
| Total | 1,223,697,000 | 1,113,580,000 | 1,386,012,000 | 1,351,943,000 | 1,390,235,000 |
DTC utilization by percentage
| Basic activity of daily living (BADL) |
2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|
| Vision | 2.0% | 1.9% | 2.0% | 1.7% | 1.5% | 1.4% | 1.5% | 1.5% | 1.4% | 1.2% |
| Walking | 29.1% | 28.8% | 28.1% | 28.8% | 29.3% | 29.0% | 29.3% | 27.5% | 27.5% | 27.3% |
| Speaking | 5.7% | 5.9% | 5.7% | 5.7% | 5.4% | 5.8% | 5.9% | 6.2% | 6.3% | 5.9% |
| Mental Functions | 22.7% | 24.0% | 24.5% | 24.1% | 24.5% | 23.9% | 23.8% | 24.0% | 24.8% | 25.0% |
| Hearing | 2.9% | 2.8% | 2.7% | 2.7% | 2.5% | 2.4% | 2.3% | 2.1% | 2.0% | 2.0% |
| Feeding | 7.3% | 6.8% | 7.0% | 6.5% | 6.0% | 6.0% | 5.8% | 5.9% | 5.7% | 5.5% |
| Dressing | 14.7% | 14.1% | 14.0% | 14.0% | 13.8% | 13.4% | 13.1% | 12.6% | 12.5% | 12.3% |
| Eliminating | 7.8% | 7.2% | 7.3% | 7.1% | 7.0% | 7.2% | 7.2% | 7.5% | 7.3% | 7.3% |
| Life-Sustaining Therapy | 3.4% | 3.5% | 3.2% | 3.4% | 3.6% | 4.1% | 4.6% | 5.6% | 5.2% | 5.7% |
| Cumulative | 4.4% | 5.0% | 5.4% | 5.9% | 6.4% | 6.8% | 6.5% | 7.1% | 7.3% | 7.9% |
| Total | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |