
Public Health Agency of Canada 2019–2020 Departmental Results Report
Complete a survey on your experience using this Departmental Results Report.

Download in PDF format
(2.23 MB, 72 pages)
Organization: Public Health Agency of Canada
Published: 2020-12-08
Table of contents
- Minister’s message
- Results at a glance
- Core Responsibilities - Results: what we achieved
- Analysis of trends in spending and human resources
- Additional Information
- Appendix: definitions
Minister’s message

As Minister of Health, I am pleased to present the 2019-20 Departmental Results Report for the Public Health Agency of Canada (PHAC). This report provides an overview of PHAC’s performance and achievements over the past fiscal year in support of the Government of Canada's commitment to protect the health and safety of all Canadians, as well as its contributions to global public health efforts.
The end of fiscal year 2019-20 was an unpredictable and unprecedented time. PHAC was instrumental in supporting Canada’s early COVID-19 global pandemic response and served as a trusted source of public health expertise and advice for Canadians and key players. Since January, PHAC has mobilized its resources to ensure the safe repatriation and quarantining of returning Canadians, activated the Health Portfolio Operations Centre to coordinate the Government of Canada’s public health response, supported the testing capacity of provincial and territorial laboratories and implemented screening and quarantine measures at the border. But COVID-19 remains a rapidly evolving global challenge. PHAC continues to work closely with provinces, territories, Indigenous Peoples, key stakeholders and industry to ensure Canadians and health care providers are equipped with the evidence-based information they need to protect themselves, their families, their communities and their businesses.
In addition to its work on Canada's COVID-19 response, PHAC had many achievements in other areas in 2019-20. Improving the physical and mental health of Canadians by promoting healthy lifestyles and relationships continued to be a focus for the Agency. In June 2019, PHAC also released Canada’s first national strategy on dementia - A Dementia Strategy for Canada: Together We Aspire - that establishes a vision for advancing dementia prevention, therapies, and the quality of life of people living with dementia and their caregivers.
As part of ongoing efforts to address the opioid-crisis and emerging drug threats, last year PHAC supported national efforts to increase the surveillance of opioid-related overdose deaths to strengthen our evidence-base, and launched the Supporting Pathways to Care for People Who Use Drugs program. This program is providing funding to projects that support sustainable system-level change to enhance pathways to care, reduce stigma and discrimination and break down barriers within the health system that prevent people who use drugs from seeking help.
As we learn to live with COVID-19 through the next phase of the pandemic, PHAC will continue to be front and centre – working to promote and protect the health and safety of Canadians, while articulating a vision for a future of public health building off lessons learned from COVID-19 and other recent public health events. I look forward to building on our important accomplishments in 2019-20 and working with partners across Canada as we continue our efforts to improve the health of Canadians.
The Honourable Patty Hajdu, P.C., M.P.
Minister of Health

Figure 1 - Text description
2019-20 COVID-19 RESPONSE BY THE NUMBERS
Supported the Federal Health Response
- $186 millions investment in Personal Protective Equipment – N-95 respirator masks, surgical masks, face shields, gowns, coveralls, nitrile gloves, vinyl gloves, hand sanitizer.
- 10-35% week over increase in correspondence and meetings with other federal government departments to coordinate policy responses.
Strengthened Border and Travel Measures
- 750 Canadians repatriated from China, Japan and the United States through PHAC’s collaboration with other government departments and provincial/local counterparts.
- 95% reduction of travelers arriving at Canada’s airports, ports and land orders due to PHAC’s travel health advisories and Emergency Orders.
- 3 large-scale federal quarantine operations to house and care for repatriated Canadians during their 14-day isolation period were established by PHAC in collaboration with other government departments.
Kept Canadians Informed
- 15.5 million nation-wide mail-outs distributed, starting in March 2020.
- 2 million daily visits to Canada.ca/coronavirus
- 34 media briefings and press conference held from January 20, 2020 – March 31, 2020.
- 28 bilateral and multilateral meetings led by PHAC with Canadian stakeholders from January 30, 2020 – March 31, 2020.
- 16 daily technical briefings with Parliamentarians hosted in March 2020, in partnership with over 15 other federal departments and agencies.
Provided leadership in Testing and Surveillance
- Over 2,000 samples processed by the National Microbiology Laboratory between January 27, 2020 and March 31, 2020 to support provincial and territorial COVID-19 testing.
- Approximately $50 million committed up until March 31, 2020 to support bulk purchasing of equipment and supplies to support testing efforts across Canada.
Results at a glance
| Total actual spending | Total actual full-time equivalents |
|---|---|
| $892,605,607 |
2,296 |
Over the past fiscal year, PHAC continued to promote and protect the health and safety of Canadians by taking further action on long-standing public health priorities and responding to COVID-19. PHAC remained focused on supporting the Minister of Health’s mandate letter commitments and government-wide priorities like Gender-based Analysis Plus (GBA+) and experimentation.
With the onset of COVID-19 in January 2020, PHAC led the federal public health role for Canada’s pandemic response to protect the health and safety of Canadians. Specifically, PHAC:
- Mobilized staff to support the federal health response, activated the Health Portfolio Operations Centre in January 2020, and activated regional emergency coordinating centres to manage local issues and stakeholder engagement.
- Activated the Federal/Provincial/Territorial Public Health Response Plan for Biological Events to ensure a coordinated public health response across Canada.
- Implemented new and enhanced quarantine and border measures in collaboration with federal, provincial, territorial and international partners to mitigate the importation risk of COVID-19 such as training and mobilizing screening and quarantine officers at Canada’s major airports.
- Established Designated Quarantine Sites in seven locations across the country, and developed necessary protocols, contracts and partnerships, and planned and operationalized the quarantining of repatriated Canadian travellers in Trenton and Cornwall.
- Developed Canada’s first diagnostic tool for the virus that causes COVID-19.
- Provided laboratory leadership and services to public health labs across Canada, including confirmatory testing for all presumed positive samples during the early days of Canada’s response, quality assurance guidance for testing accuracy, and in-depth analysis of difficult to diagnose specimens.
- Supported critical COVID-19 response efforts in the areas of surveillance and risk assessment including: daily scans of COVID-19 scientific publications and rapid review summaries on issues such as pregnancy, infants, high-risk populations and co-morbidities; the development of public health measures guidance through consultation with the provinces and territories, as well as targeted stakeholder groups; and led early planning and coordination of an interdepartmental medical countermeasures action plan.
- Took swift and extensive communication actions to inform Canadians of the risks related to COVID-19 and measures they could take to protect their health and safety.
- Engaged with key stakeholders across various sectors to ensure common messaging and understanding on COVID-19 risks and mitigations in differing workplaces.
In addition to its focus on the COVID-19 response, PHAC also achieved the following key results under its three Core Responsibilities and Internal Services in 2019-20:
Health Promotion and Chronic Disease Prevention
- Continued to support the Minister of Health’s mandate letter commitment to work collaboratively with provinces, territories, families and stakeholders toward the creation of a national autism strategy. In recognition of the broad scope of issues at play, which include both health as well as social and economic aspects, PHAC established a federal inter-departmental committee to facilitate a whole of government approach. The committee has been meeting on a regular basis since February 2020 to discuss the key elements of a broad engagement framework and to discuss current and ongoing federal initiatives to support individuals living with autism spectrum disorder.
- Supported the implementation of the Indigenous Early Learning and Child Care Framework that supports self-determination, improved service delivery and advances reconciliation for First Nations, Inuit and Métis Peoples. PHAC worked closely with the National Aboriginal Head Start Council (the Indigenous-led governance body for the Aboriginal Head Start in Urban and Northern Communities program), the National Expert Working Group on First Nations Early Learning and Child Care, and Inuit partners to advance their priorities and shared objectives.
- Developed resources for health professional organizations and their members designed to mitigate and prevent substance use stigma within the health system, using such means as compassionate, non-stigmatizing language and evidence-based initiatives to address systemic stigma.
- Funded three Indigenous organizations: Manitoba Métis Foundation Inc., the First Nations Health and Social Secretariat of Manitoba and the National Native Addictions Partnership Foundation (also known as Thunderbird) to address evidence gaps in Indigenous health through programming aimed at improving evidence of the health impacts of problematic use of opioids in Indigenous communities. Organizations have since conducted community consultations, developed research plans, and have started to conduct collaborative research with Indigenous communities.
Infectious Disease Prevention and Control
- Supported provinces and territories to improve vaccination acceptance and uptake and further protected Canadians by investing in projects through the Immunization Partnership Fund.
- Released Accelerating our response: Government of Canada five-year action plan on sexually transmitted and blood-borne infections on July 17, 2019, to advance the work of the Pan-Canadian Sexually Transmitted and Blood-borne Infections (STBBI) Framework and reduce the public health impacts of STBBI in Canada.
- Continued to engage partners and stakeholders across the One Health spectrum to ensure their needs and priorities are reflected in the Pan-Canadian Action Plan on Antimicrobial Resistance (PCAP). Efforts are ongoing to identify opportunities to work collaboratively with provinces, territories and other stakeholders to move forward in priority areas.
Health Security
- Responded to 14 domestic requests for assistance to investigate and manage disease outbreaks and mobilized resources to support Ebola response efforts, coordinated by the World Health Organization.
- Launched the Analytical Approach to Biosafety and Biosecurity, an online policy toolkit created to help other countries strengthen their policies and oversight frameworks for pathogen biosafety and biosecurity.
Internal Services
- Implemented an Accessible and Inclusive Meeting Space pilot project to raise awareness of and reduce workplace barriers to persons with disabilities through state of the art design elements including technology, lighting, signage and furniture.
- Provided Canadians with timely and relevant public health information on a range of topics, including Lyme disease, vaccination, problematic substance use and stigma.
Operating Context
COVID-19 has shown that PHAC operates in a complex, interconnected, and evolving environment with a central mandate to keep Canadians healthy and safe from emerging threats.
While the majority of Canadians are experiencing good health and living longer, certain key populations and regions (e.g., low-income families, children, Indigenous Peoples, people living in northern, remote and isolated areas, the elderly, LGBTQ2+ and racialized communities) continue to experience increased risks of poor health outcomes. The COVID-19 outbreak reminds us that there is increased risk among these populations. Canada also continues to face persistent public health challenges including the increased burden from chronic diseases (e.g., diabetes), the re-emergence of Vaccine-Preventable Diseases (e.g., measles), the rise in sexually transmitted infections, the threat of drug-resistant organisms, as well as harms and deaths associated with the problematic use of alcohol and other substances such as opioids.
Given the dynamic and evolving nature of public health events, PHAC must continue to have the capacity to prevent, prepare for and respond quickly to public health events and emergencies. Increasingly, public health events tend to be complex, with far-reaching causes and consequences, and have undefined timelines, potentially requiring urgent action and a long-term response, as evidenced by the COVID-19 pandemic and Canada’s ongoing opioid crisis. PHAC will adapt its resources (such as human resources, skill sets), tools, processes, and partnerships to maintain the capacity to rapidly and effectively prevent, detect, and respond to emerging global and domestic public health events. The ability to proactively recognize key risks to health and contributing factors, and to be prepared with the appropriate resources and supports to respond effectively, may greatly affect the ability of PHAC’s programs to achieve results for Canadians.
Timely and reliable data and knowledge are essential for developing sound policies, ensuring effective programming that delivers results to Canadians, delivering accurate information to Canadians, and supporting overall government priorities (e.g., GBA+ and Gender Inclusive Services, Sustainable Development Goals, and experimentation). Consequently, strengthening surveillance, collection, and access to national data supports evidence-based decision-making.
While the current response to COVID-19 has been focused on immediate crisis measures and re-opening segments of the economy and society in the shorter term, the pandemic will have long-lasting impacts that will shape policy measures for many years. Building a more resilient public health system will need to be part of a broader and coordinated set of longer-term government initiatives. The multi-jurisdictional nature of public health also creates a diverse collaboration, coordination and engagement environment. Public health is a shared responsibility in Canada, with coordination between the federal, provincial, territorial and municipal governments. PHAC must work collaboratively with all levels of government, stakeholders, and partners nationally and internationally to set and achieve public health goals and targets. By improving our understanding of the priorities, activities, and concerns of partners and stakeholders, PHAC will be better able to adapt its programs (including those supported through grants and contributions) to respond to the diverse public health needs across Canada. PHAC’s commitment to accountability, openness, and results will help promote important multi-sectoral collaborations and the solutions needed to help improve the health of Canadians.
For more information on PHAC’s results achieved, see the “Results: what we achieved” section of this report.
Core Responsibilities - Results: what we achieved
1. Health Promotion and Chronic Disease Prevention
Description
Promote the health and well-being of Canadians of all ages by supporting community-based projects which address the root causes of health inequalities and the common risk and protective factors that are important to preventing chronic disease, and conduct public health research and surveillance.
Results
Under this core responsibility, PHAC is focused on advancing the following departmental results:
- Canadians have improved physical and mental health.
- Canadians have improved health behaviours.
- Chronic diseases are prevented.
To make progress towards achieving these results, PHAC focused its 2019-20 health promotion and chronic disease prevention efforts on key initiatives and activities that effectively delivered on the Minister’s mandate letter commitments. These commitments related to the opioid crisis and mental health, addressing the rapid rise in youth vaping, planning for the creation of a national autism strategy, preventing and reducing substance related harms, keeping cannabis away from children, and integrating Sex and Gender-based Analysis Plus (SGBA+)Footnote 1 considerations in program design and delivery.
The early effects of the COVID-19 pandemic on funded projects were evident at the end of the fiscal year with many recipient organizations experiencing difficulty carrying out planned activities. Furthermore, several recipient organizations showed early signs of facing financial challenges during this time of economic slowdown. In many cases, adaptations were required to research and evaluation protocols as projects were compelled to pivot to alternate online delivery methods. Funded community organizations have responded with creative and innovative approaches and are working to adjust activities to better support those who are most vulnerable during the COVID-19 pandemic.
Result 1.1 Canadians have improved physical and mental health
Addressing health-related impacts of family violence and gender-based violence
Recognizing that family violence and gender-based violence can have serious and lasting negative impacts on both physical and mental health, PHAC invested over $14 million for 52 projects to prevent violence and support survivors. Through the Supporting the Health of Survivors of Family Violence Investment, PHAC provided continued support to 20 projects aimed at addressing the health needs of survivors of family violence. These projects reached youth (including street-involved youth), survivors of sex trafficking, young mothers, racialized people, Indigenous Peoples, LGBTQ2+ individuals, rural communities, persons with disabilities, and newcomers to Canada. As part of the Preventing Gender-Based Violence: The Health Perspective Investment, which is part of Canada’s Strategy to Prevent and Address Gender-Based Violence, PHAC supported 32 projects focusing on preventing teen dating violence and child maltreatment. Projects supported through these investments helped prevent gender-based violence by teaching youth about respect, consent and healthy relationships. For example, the WiseGuyz project, led by the University of Calgary with the Centre for Sexuality, helped teach adolescent boys about positive gender norms and healthy forms of masculinity. Projects also supported survivors of family violence to rebuild their physical and mental health. For example, the Bounce Back League project, led by Boys and Girls Clubs of Canada, offered a trauma-informed sport curriculum, which led to improvements in well-being and sense of belonging for participating youth.
DID YOU KNOW?
The Evaluation of the Supporting the Health of Survivors of Family Violence Program 2015-16 to 2018-19, published in November 2019, found that survivors of family violence are participating in the interventions offered by funded projects and that professionals are accessing information shared through the program. The evaluation also found evidence to demonstrate that projects have increased knowledge and skills, or changed the behaviours and practices of survivors and professionals.
In addition to reaching children, youth and families, these investments also helped equip service providers to prevent and respond to family and gender-based violence. For example, OUTSaskatoon undertook an initiative to help educators and health and social service providers better support LGBTQ2+ people who have experienced gender-based violence.
To expand the evidence-base in the field of violence prevention and response, PHAC also supported mechanisms for collaboration and knowledge mobilization. The Family Violence Knowledge Hub and the Youth Dating Violence Community of Practice hosted meetings and webinars and produced bulletins and web content to facilitate learning, shared problem solving, and knowledge exchange among funded projects and the broader community of service providers, researchers and policy makers across Canada. Collectively, these projects delivered programming directly to over 11,000 participants and professionals in 2019-20, and reached over 700,000 researchers, policy makers and service providers through knowledge products and events. These investments helped build knowledge, enhance practice, and promote skills and abilities to prevent violence and its health impacts. PHAC also continuously supported projects toward achieving results by providing ongoing advice and guidance, and facilitating mentoring and exchange among projects.
Improving the mental health and psychological well-being of Canadians
In 2019-20, PHAC continued to support key initiatives aimed at improving the mental health and psychological well-being of Canadians. For example, in early 2020 PHAC released Canada’s first Federal Framework on Post-traumatic Stress Disorder in support of its efforts to increase national awareness and enhance the diagnosis, treatment and management of post-traumatic stress disorder (PTSD). The content was informed by a national conference on PTSD held in April 2019 and with the direct involvement of stakeholders and partners, including those with lived experience.
In addition, PHAC continued to support Crisis Services Canada, which provides 24/7 suicide prevention support to people across Canada, resulting in more than 31,000 interactions in 2019-20. Through Budget 2019, which announced an investment of $25 million over 5 years, and $5 million per year ongoing, PHAC will support the expansion of the pan-Canadian suicide prevention service, so that Canadians have access to the support they need, in both English and French, via voice, text and online chat.
In 2019-20, the Mental Health Promotion Innovation Fund (MHP-IF) provided funding to 20 innovative projects across Canada to test and deliver interventions that help children, youth and their primary caregivers to achieve positive mental health. The funding supports priority groups susceptible to mental health inequities, such as: First Nations, Inuit and Métis, LGBTQ2+, newcomers and refugees. In their first phase of funding, these projects are working to develop and test innovative methods to reach these key populations. This includes the use of innovative technology and approaches, distance delivery of programming, and culturally appropriate land-based and arts-based programming. Knowledge and evidence gained from the evaluation of each community-based intervention is intended to enhance Canadian public health policy and practice, and is being supported by a Knowledge Development and Exchange (KDE) Hub.
Ensuring that Canadians affected by autism spectrum disorder (ASD) have the information and resources they need to lead a successful and healthy life remained a priority for PHAC as it began foundational work related to plans for a national autism strategy. In 2019-20, with support from Employment and Social Development Canada, PHAC worked to develop an interdepartmental and cross-government approach to collaboration and planned for the creation of the national autism strategy. As part of this work, PHAC also continued to fund community-based projects through the Autism Spectrum Disorder (ASD) Strategic Fund, and supported the creation of the Autism and Intellectual Disabilities Knowledge Exchange Network (AIDE) Canada. Important results achieved in 2019-20 include the launch of the AIDE Canada website, which provides a suite of bilingual resources and tools for individuals living with ASD and intellectual disability. For example, the Sensory Processing Differences toolkit provides Canadians living with ASD an introduction to the eight sensory systems, questions to help determine an individual’s most impacted sensory systems, and offers health improvement and daily living strategies to try at home.
Promoting Health Equity: The Mental Health of Black Canadians Fund
Recognizing that Black Canadians face significant social and economic challenges that have negative implications for their mental health, in 2019-20 PHAC provided over $1 million in funding for 16 projects through the Promoting Health Equity: Mental Health of Black Canadians (MHBC) Fund, to support culturally focused programs and interventions that address mental health and its determinants for Black Canadians.
For example, PHAC funded the Kaleo Productions project to help eliminate stigma and educate on the realities of mental health among Black, African and Caribbean members of Black churches in the Greater Toronto Area. The project developed a documentary film, monologue video and pamphlet, and delivered five community engagement sessions and a youth workshop. In total, 450 people were reached through project activities, including 225 Black youth.
Health Promotion for Children and Youth and Maternal Child Health
In 2019-20, PHAC also continued to support a range of initiatives aimed at improving the health and healthy development of children in Canada, with a focus on vulnerable populations and low-income families. PHAC’s long-standing Community Action Plan for Children program, Aboriginal Head Start in Urban and Northern Communities Program (AHSUNC) and Canada Prenatal Nutrition Program (CPNP) continued to support 592 community organizations to provide essential stigma-free and culturally-inclusive programming, knowledge translation and counselling supports to vulnerable children (ages 0-6) and families, reaching 280,000 participants across the country. In addition, PHAC supported the implementation of the Indigenous Early Learning and Child Care Framework for Inuit, Métis and First Nations for children living off-reserve in urban and northern areas through investments in 134 AHSUNC sites so that all Indigenous children have the opportunity to experience culturally rooted early learning and child care programming of a high quality.
PHAC also launched a new program in 2019-20 called the Healthy Early Years program, aimed at improving access to early childhood health and development programming in Official Language Minority Communities (OLMCs), including the development of new resources and training. This new contribution program supported 46 projects in 2019-20 and implemented a range of locally-tailored activities to support parents and young children through prenatal, pregnancy and postpartum care guidance, parenting skills, healthy eating guidance, and mental health promotion support.
In addition to the funding of community-level organizations, PHAC supported a range of knowledge translation, policy and guidance work. This work included the release of a new Family-Centered Maternal and Newborn Care National Guidelines chapter, entitled “Care during Pregnancy”. Significant advancements were also made in work with health experts to develop a new Joint Statement on Traumatic Head Injury due to Child Maltreatment, a revised Joint Statement on Safe Sleep, two new breastfeeding promotion and guidance booklets, and a new guide on healthy pregnancy. PHAC also continued to provide funding to the Breastfeeding Committee for Canada to lead a national Baby-Friendly Initiative Quality Improvement Collaborative project across Canada. This project is being implemented with 15 healthcare organizations at 26 hospital sites, helping to ensure they have practices and standards in place to be breastfeeding-friendly.
Result 1.2 Canadians have improved health behaviours.
Preventing and reducing harms related to substance use
In 2019-20, PHAC continued to work with partners and stakeholders to support the prevention and reduction of substance-related harms, particularly among priority populations. While the Government of Canada has implemented a wide range of actions to address the opioid crisis, significant gaps exist in our ability to comprehensively understand and mobilize interventions that work, particularly in relation to pathways to care that meet people where they are at, from prevention to harm reduction to treatment, and health care more broadly. In 2019-20, Supporting Pathways to Care for People Who Use Drugs launched and will provide $3.6 million to projects that catalyze system-level change with enduring impact to enhance pathways to care and reduce barriers within the health system for people who use drugs. PHAC has also worked to publish tools and resources for health professionals to reduce substance use stigma in the public health system. By working with multi-sectoral partners, the national surveillance system on the opioid crisis was expanded. Quarterly reports on opioid-related deaths and overdoses based on data from the national surveillance system were viewed 69,445 times in 2019-20 by 45,980 unique visitors. In addition, foundational work was completed to support the future capture of additional substances such as methamphetamines and alcohol.
In 2019-20, PHAC worked with dental professionals and regulatory organizations to encourage dentists to support a reduction of opioid and antibiotic prescriptions in dentistry. The Health Canada Opioid Response and PHAC Antimicrobial Resistance (AMR) teams gathered relevant data and research to inform Government of Canada policy and guidelines that were rapidly disseminated to oral health stakeholders in Canada for implementation in dental education, regulation and professional practice. PHAC also participated in the National Antibiotic Awareness Week with members of the Chief Public Health Officer (CPHO) Health Professional Forum, to raise awareness on the dangers of overprescribing antibiotics.
Informing Canadians about Public Health Issues
PHAC continued to work in close collaboration with Health Canada to respond to the opioid crisis. Resources were produced and reviewed by the CPHO Health Professional Forum to reduce stigma in the Canadian health system and to guide health professional organizations to communicate about substance use in non-stigmatizing ways. This work included launching the third wave of the advertising campaign, featuring ads on television, social media and the internet.
The Know More public awareness tour wrapped up in August 2019. Since 2018, the tour has engaged 144,114 youth and young adults across Canada on the facts surrounding the opioid crises and health risk associated with problematic opioid use. Between April 1, 2019, and March 31, 2020, 19,520 young people visited the tour through summer events and festivals, and 33,988 students at 140 high schools and 30 post-secondary institutions engaged in the tour. This campaign was complemented by online content, including the In Plain Sight audio series profiling experiences of those affected by opioids, as well as partnerships with organizations across the country, including the Canadian Association of Fairs and Exhibitions, Canadian Aboriginal Aids Network and Canada’s Building Trades Unions.
The CPHO 2019 Annual Report Addressing Stigma: Towards a More Inclusive Health System also focused on how different populations experience poorer health with an emphasis on stigma as a driver of health inequalities.
Construction Industry Tobacco Cessation Project - Build Smoke Free
In 2019-20, to address the high smoking rate among young men in construction trades – which is double the national average – PHAC supported the Construction Industry Tobacco Cessation Project - Build Smoke Free. This project is delivering individualized smoking cessation supports to workers on construction sites across the country. Since its inception, 240 construction workers across six sites in Ontario joined the program to make a quit attempt. Preliminary results collected among spring 2019 and fall 2019 cohorts are indicating positive outcomes. At the six-month follow-ups, respectively 88% and 76% of the participants self-declared increased knowledge about ways to quit smoking and about the benefits of quitting smoking cigarettes. Nicotine dependence and smoking behaviour were significantly reduced at six-month follow-up when compared with the baseline, as the proportion of current smokers decreased from 93% to 68%. While smoking culture on worksites was considered a barrier to cessation by all interview participants, it was noted that a quitting culture has emerged on intervention sites, where employees are talking about quitting and supporting one another through words of encouragement or not smoking around each other.
ParticipACTION - Let’s Get Moving
PHAC also continued to support public education and awareness activities related to increasing physical activity for all Canadians, while focusing on reaching groups that experience health inequalities related to physical activity. Physical inactivity and sedentary behaviour levels remain high, especially among children and youth. In Canada, at least four in five adults do not meet the Canadian Physical Activity Guidelines. Through a Budget 2018 commitment, PHAC is supporting ParticipACTION to implement a national public education campaign and increase daily physical activity among Canadians with the Let’s Get Moving initiative.
Launched in 2019, the ParticipACTION app, gives participants free access to information, motivational nudges and content to help overcome barriers to physical activity and track activity associated with participation in community events. To date, the ParticipACTION app has reached 108,830 users including 42% of them using it regularly.
The ParticipACTION annual Community Better Challenge awards grants to organizations across Canada to promote physical activity in their communities. Between May and June 2019, almost 4 million individuals participated in the Community Better Challenge. A total of 1,450 organizations hosted events and tracked physical activity for participants registered in the Challenge. Participants who registered on the app and took part in the Challenge increased their weekly moderate to vigorous physical activity minutes from 114 to 200 minutes per week from May to June. They were more likely to meet the physical activity guidelines and were less likely to spend sedentary time after the Challenge compared to before.
Result 1.3 Chronic diseases are prevented.
Chronic disease surveillance
The Canadian Chronic Disease Surveillance System (CCDSS) is a collaborative network of provincial and territorial surveillance systems supported by PHAC that generates estimates and trends for more than 20 chronic diseases. 2019 celebrates twenty years of investment by the federal government in chronic disease surveillance through the CCDSS and publications were produced demonstrating how the CCDSS has evolved over time. As part of this, diabetes trends in Canada over 20 years were showcased in an interactive data blog, a peer-reviewed paper and an infographic, highlighting national statistics, risk factors and complications, and the changes of the rates of diabetes in Canada using the CCDSS. The CCDSS also released its first national estimates and trends for schizophrenia. In recognition of this, PHAC published its first Schizophrenia in Canada infographic as well as an interactive Data Blog on the Public Health Infobase.
Supporting healthy aging and improving the quality of life of those impacted by dementia
The release of Canada’s first national dementia strategy: A Dementia Strategy For Canada: Together We Aspire, highlights the Government’s commitment to create “a Canada in which all people living with dementia and caregivers are valued and supported, quality of life is optimized, and dementia is prevented, well understood, and effectively treated.” The national dementia strategy sets out this vision and identifies common principles and national objectives to help guide actions by all levels of government, non-governmental organizations, communities, families and individuals. In June 2019, the first annual Report to Parliament on the strategy was released. This report highlighted the extensive engagement that informed development of the strategy, and emphasized the Government of Canada’s ongoing commitment to identify areas for further collaboration with federal, provincial and territorial governments and key dementia stakeholders.
The Dementia Strategic Fund provides $40 million over 5 years, starting in 2019-20, to support the implementation of key elements of the national strategy. In January 2020, PHAC launched the first open solicitation for funding focused on awareness raising under the Dementia Strategic Fund. To improve the availability of data that informs implementation of the national dementia strategy, The Dementia Strategic Fund supported two public opinion research projects. The first project surveyed about 4,200 Canadians to create a nationally representative baseline of general awareness as well as measuring knowledge about risk reduction, attitudes about seeking and sharing information about a dementia diagnosis, views on the abilities of people living with dementia, and experiences with providing care. It also provides insights into differences in knowledge and attitudes across regions and demographic groups. The second project, intended to inform development of a national social marketing campaign, provides an in-depth assessment of the awareness, knowledge, attitudes, and behaviours of the Canadian population surrounding dementia, including prevention and stigma. In addition, PHAC completed an environmental scan of existing dementia guidance to inform priority-setting for subsequent work.
In 2019-20, PHAC’s Dementia Community Investment also launched its first 17 projects across eight provinces and territories, with $1.6 million in funding. These community-based projects develop, test and scale up knowledge and resources to optimize the well-being of people living with dementia and family/friend caregivers and increase knowledge about dementia. Funded projects reached 337 family/friend caregivers and 187 people living with dementia. For example, a project led by the Native Women’s Association of Canada is working to develop a culturally-informed toolkit that aims to address the challenges and social isolation that can be associated with caregiving in rural and remote Indigenous communities and contribute to a growing knowledge base of culturally safe and trauma-informed dementia education.
To improve our understanding of dementia, PHAC also collected and analyzed the latest dementia data from the CCDSS. In 2019-20, data from CCDSS was used to report results on the state of dementia in Canada through a variety of products including the Canadian Chronic Disease Indicators, the Canadian Chronic Disease Surveillance System data tool, and the updated infographic Dementia in Canada. These results support policy, program and related healthcare planning and delivery.
Further, PHAC supports innovation in the aging and brain health sector by funding the Centre for Aging and Brain Health Innovation (CABHI). In 2019-20, CABHI received $10 million from PHAC that supported innovation and experimentation as part of a larger $42 million investment over five years. In 2019-20, CABHI supported the launch of 301 projects. Of particular note, 172 new products, processes, and services were introduced into practice or brought to market, and 313 products, practices, or services were evaluated. Furthermore, a recent evaluation found that in its first four years of operation, CABHI achieved notable success by supporting stakeholders in various ways, such as being able to access test environments, facilities, resources, or data.
Implementation of the Healthy Seniors Pilot Project (HSPP)
The Healthy Seniors Pilot Project (HSPP) is a $75 million three-year agreement with the province of New Brunswick, funded by PHAC. The HSPP supports a range of applied research initiatives to examine how governments, in partnership with the community and private sectors, can better support seniors in their homes, communities and care facilities. One such project aims to engage seniors in proactively monitoring their health status and risk factors with the use of a new digital health platform and support from health-care professionals. The longer-term goal is to discover trends in health data using predictive analytics, which could allow seniors to stay healthier in their own homes while reducing hospitalizations.
Falls prevention among seniors
To help reduce the incidence of falls amongst older adults, PHAC supported the development of the Pan-Canadian Seniors’ Fall Prevention Network Project aimed at promoting education, knowledge sharing and collaboration among stakeholders. The activities from the network project have improved connectivity and engagement among leaders in fall prevention (the Seniors’ Fall Prevention Network), raised public awareness of the risk factors that contribute to older adults’ falls and how to prevent them, and created a central hub of resources for individuals and health professionals. The project also identified future opportunities that could address gaps in seniors’ fall prevention.
Healthy Living and Chronic Disease Prevention – Multi-sectoral Partnerships (MSP) program
Between 2013-14 and 2019-20, the Healthy Living and Chronic Disease Prevention – Multi-sectoral Partnerships (MSP) program funded 60 health promotion and chronic disease prevention projects promoting public health related multi-sectoral partnerships across Canada to support projects that address common risk factors (e.g., physical inactivity, unhealthy eating and tobacco use) associated with major chronic diseases such as cancer, diabetes and cardiovascular disease. These projects received a total investment from PHAC of $141 million and an additional $111 million leveraged in non-government funding.
In 2019-20, there were 41 active projects at approximately 105 sites nationwide, involving 250 partner organizations from multiple sectors including health, recreation, social, industry, entertainment and technology. Funding for projects through the MSP program was retooled in 2019-20 to better reflect lessons-learned from recent years and to fully realize its aim of supporting innovative approaches, promoting interventions proven effective and reaching populations in greater needs. The Audit of the Multi-Sectoral Partnerships Program to Promote Healthy Living and Prevent Chronic Disease at the Public Health Agency of Canada published in February 2020 found that the program is noted as a leader among those within the Government of Canada who use experimental program design and apply innovative funding models. The reach of projects funded by the MSP program varies based on the different kinds of community-based interventions that are funded. For example, the ParticipACTION media campaign reached approximately 6 million people, and the Community Better Challenge reached almost 4 million. In addition, more direct interventions reached approximately 300,000 participants such as the Community Food Centres Canada’s FoodFit program, which helps low-income Canadians make healthy eating and physical activity behaviour changes.
WHAT’S NEW?
In 2019-20, PHAC announced 12 multi-sectoral partnerships to Canadians.
- University of Toronto - All Together Now!
- Vivo for Healthier Generations Society – Vivo Play Project
- LMC Healthcare – Diabetes Prevention Program
- Recreation PEI go!ForIT project!
- Canadian Cancer Society Construction Industry Tobacco Cessation Project
- Canadian Society for Exercise Physiology Development of the Canadian 24-Hour Movement Guidelines for Adults and Older Adults
- Fondation Tremplin Santé’s Shape Up program
- University of Alberta's Housing for Health project
- FitSpirit's Physical Activity and Healthy Lifestyles for Teen Girls
- Dalhousie University – UpLift
- Alliance Wellness and Rehabilitation Inc.– Healthy Kids Initiative
- Western University – Hockey Fans in Training
- Simon Fraser University – RADIUS Health Promotion Lab
A Common Vision for Increasing Physical Activity and Reducing Sedentary Living in Canada: Let’s Get Moving (Common Vision)
In 2019-20, PHAC continued to support and promote early action on A Common Vision for Increasing Physical Activity and Reducing Sedentary Living in Canada: Let’s Get Moving (Common Vision). The aim is to leverage action on this policy framework to support Canadians and communities to move more and sit less. Through PHAC leadership, in December 2019 the Federal/Provincial/Territorial Physical Activity and Recreation Committee announced six non-governmental Champions to support the areas of focus within the Common Vision. These Champions are responsible for developing and implementing action-oriented plans over two to three years to advance their respective area of focus, in collaboration with non-governmental partners that represent diverse communities. In 2019-20, these projects received a total investment from PHAC of $1.2 million with work in the early stages of development.
Oral Health
In 2019-20, PHAC commissioned a comprehensive evidence-based review with the University of Alberta to update webpage content on Seniors Oral Health. This online content serves as a national reference resource for other federal departments as well as provincial and territorial program developers.
PHAC also commissioned a Canadian Agency for Drugs and Technologies in Health Health Technology Assessment on community water fluoridation (CWF) – a universal, safe and cost-effective way to prevent tooth decay – to support evidence-based decision-making in communities. The report has become a national reference resource for CWF policy and responses to related queries from the public. It is also used by federal, provincial and territorial partners, other federal departments, and oral health stakeholders within Canada and internationally.
Innovation and Experimentation
Guided by the principles of experimentation and innovation, the Healthy Living and Chronic Disease Prevention – Multi-sectoral Partnerships (MSP) program aims to discover, validate and promote effective approaches to improve the health of Canadians. Every proposed project is required to demonstrate how it will stretch beyond traditional approaches in order to utilize new and/or different implementation and/or measurement methodologies.
Innovative approaches may relate to intervention delivery (e.g., healthy living-dedicated apps); to the way participants are supported (e.g., using vouchers or prescriptions as incentives to encourage the adoption of healthy behaviours); to recruitment methods (e.g., using social media); or for need identification (e.g., the development of a walkability index to target intervention where potential impact is greater). PHAC also began pilots for several new funding models. For example, the Base Plus Premium Payment funding model uses a payment structure that provides a financial mechanism to directly link performance and premium payments to measureable changes in health outcomes for project participants. Premium payments to funding recipients are applied to predetermined targets as measured by statistically and clinically significant changes in the health of participants, such as cardiorespiratory fitness or quality of life. In 2019-20, there were three active projects featuring this model: Western University (Hockey Fans in Training), Alliance Wellness and Rehabilitation Inc. (Healthy Kids Initiative), LMC Healthcare (Canadian Diabetes Prevention Program). Projects began implementation in 2018-19, and while measurement is underway, it is too early to determine results.
As part of the Promoting Health Equity: Mental Health of Black Canadians (MHBC) Fund, PHAC engaged Black community stakeholders through the Mental Health of Black Canadians Working Group, to identify the most pressing needs related to mental health and its determinants for Black Canadians. The MHBC engagement model has been viewed by Working Group members and other federal government departments as a positive and innovative approach to collaboration with Black communities, and it has increased credibility and legitimacy with Black communities and set the stage for sharing knowledge with broader communities of Black Canadians and organizations.
In 2019-20, PHAC continued to test the feasibility of using artificial intelligence technology to detect suicide ideation using Twitter data. Approximately 140,000 English tweets were collected retrospectively for a one-year period (January 2018 to December 2018) based on key words, including potential risk factors. Initial results suggest that this could be a promising complementary data source for suicide surveillance, however, there are limitations to PHAC’s ability to conduct trend analysis given the available data. PHAC will continue exploring novel ways of obtaining more timely data collection solutions for suicide surveillance.
Sex and Gender-based Analysis Plus
SGBA+ is incorporated into the design of all programming within the health promotion and chronic disease prevention programs of PHAC.
Suicide rates are disproportionately high among men and boys in Canada. Evidence also suggests that men and boys are less likely to reach out for crisis support when needed. Therefore, organizations applying to administer the pan-Canadian suicide prevention service were asked to describe how they would use a SGBA+ to inform project activities, including outreach to priority populations, service delivery, data collection, performance measurement and evaluation.
SGBA+ has also enhanced analyses to tease out the differential impact of the opioid crisis among diverse population groups and informed subsequent decision-making. For example, the EQUIP Health Care team (Equip Primary Healthcare for Equity) at the University of British Columbia will enhance and tailor all existing EQUIP content to include SGBA+ content on stigma, discrimination and inequity related to substance use for vulnerable or marginalized population groups including women experiencing violence, Indigenous People and those living in poverty.
PHAC’s ASD Strategic Fund supports community-based projects to address a broad range of issues including mental health, sexuality, and employment that incorporate consideration of gender as well as other identity factors such as age, education, language, geography, culture and income in the development of their program activities. For example, the Healthy Relationships, Sexuality and Autism (HRSA) project led by Autism Nova Scotia delivers a curriculum built using critical pedagogy that reflects the lived experiences of learners and marginalized communities including, but not limited to: LGBTQ2+ groups, Indigenous Peoples, new immigrants, racialized people, and people with disabilities. This SGBA+ foundation resulted in language, resources, and modules that reflect the diversity of the learners in HRSA.
Maternal and child health knowledge translation and policy work are implemented with a view to the range of needs of diverse groups of women and families, with a particular focus on those facing health inequalities, and consideration of the impact and applicability of the programs and materials. For example, Community Action Program for Children (CAPC) and Canada Prenatal Nutrition Program (CPNP) projects are tailored to local and individual needs, with projects aiming to be culturally safe, stigma-free and welcoming to gender diversity, while actively removing barriers to facilitate participation. Training and knowledge translation resources aimed at encouraging best practices are regularly shared and delivered amongst funded projects.
The AHSUNC program early learning opportunities were augmented with holistic support for culturally isolated, vulnerable participant families living off-reserve or away from their home communities. These supports improve inclusion and access to necessary resources and guidance in navigating issues of food insecurity, mental health, housing, health services, safety and skills training.
Initiatives funded through the Dementia Strategic Fund integrated SGBA+ considerations throughout their solicitations, including screening questions asked as part of the Letter of Intent stage. Projects funded through the Dementia Community Investment integrated the consideration of SGBA+ into their proposals and are expected to report on these considerations in their annual reporting to PHAC.
| Departmental ResultsFootnote a | Departmental Result Indicators | Target | Date to achieve target | Actual results | ||
|---|---|---|---|---|---|---|
| 2019-20 | 2018-19 | 2017-18 | ||||
| Canadians have improved physical and mental health | % of low-income children in very good or excellent healthFootnote b | 80% | Mar. 31, 2020 | Data expected in Fall 2020 | Data expected in Fall 2020 | Data expected in Fall 2020 |
| % of population who have high psychological well-beingFootnote c | 75% | Mar.31, 2020 | 75% (CCHS 2019) |
75% (CCHS 2015) |
75% (CCHS 2015) |
|
| Canadians have improved health behaviours | % increase in average minutes/day of physical activity among adultsFootnote d | 20% (30 min/day) |
Mar. 31, 2025 | Data expected in Fall 2020 | 4%Footnote * 26 min/day (CHMS 2016-17) |
-4%Footnote * 24 min/day (CHMS 2014-15) |
| % increase in average minutes/day of physical activity among children/youthFootnote d | 10% (64 min/day) |
Mar. 31, 2025 | Data expected in Fall 2020 | 9%Footnote * 63 min/day (CHMS 2016-17) |
-2%Footnote * 57 min/day (CHMS 2014-15) |
|
| Chronic diseases are prevented | % increase in years lived in good health by seniors | 4% (HALE at age 65 = 17.0 years) |
Mar. 31, 2022 | 1% 15 years (Statistics Canada, 2010 – 2012 to 2015 – 2017)Footnote e |
1%Footnote * 16.6 years (CCDSS 2013–14 to 2015–16) |
1%Footnote * 16.6 years (CCDSS 2012–13 to 2014–15) |
| Rate of new diabetes cases among CanadiansFootnote f | 6.2 Cases per 1,000 age 1 and older |
Mar. 31, 2020 | 6.2 cases per 1,000 age 1 and olderFootnote * (CCDSS 2016-17) |
6.1 cases per 1,000 age 1 and olderFootnote * (CCDSS 2015-16) |
6.1 cases per 1,000 age 1 and olderFootnote * (CCDSS 2014-15) |
|
| % of adults who are obeseFootnote g | 28% | Mar. 31, 2020 | Data expected in Fall 2020 | 27%Footnote * (CHMS 2016-17) |
28% (CHMS 2014-15) |
|
| % of children and youth who are obeseFootnote g | 13% | Mar. 31, 2020 | Data expected Fall in 2020 | 11%Footnote * (CHMS 2016-17) |
13% (CHMS 2014-15) |
|
|
||||||
| 2019–20 Main Estimates |
2019–20 Planned spending |
2019–20 Total authorities available for use |
2019–20 Actual spending (authorities used) |
2019–20 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 257,822,279 | 257,822,279 | 278,546,895 | 273,405,685 | 15,583,406 |
Authorities available for use increased during the fiscal year mainly due to funding approved for Gender-Based Violence after the 2019-20 Departmental Plan was published, and included new funding received for the Collective Bargaining Agreements, National Dementia Strategy, Suicide Prevention, Pan-Canadian Suicide Prevention, and Strategy to prevent Overdose Deaths – Opioids.
Actual spending varied from planned spending primarily due to the new funding received.
| 2019–20 Planned full-time equivalents |
2019–20 Actual full-time equivalents |
2019–20 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 484 | 524 | 40 |
Financial, human resources and performance information for PHAC’s Program Inventory is available in the GC InfoBase.
2. Infectious Disease Prevention and Control
Description
Protect Canadians from infectious diseases (e.g., Human Immunodeficiency Virus [HIV], E. Coli, measles) by predicting, detecting, assessing, and responding to outbreaks and new threats; and contribute to the prevention, control, and reduction of the spread of infectious disease among Canadians.
Result
Under this Core Responsibility PHAC is focused on advancing the following Departmental Results:
- Infectious diseases are prevented and controlled.
- Infectious disease outbreaks and threats are prepared for and responded to effectively.
To make progress towards achieving these results, PHAC focused its 2019-20 efforts on key initiatives and activities that provide Canadians and public health stakeholders with the science, data, information, and resources to prevent infectious diseases and reduce harms when these diseases occur. PHAC’s collaboration with domestic and international partners advanced public health solutions to complex threats, such as antimicrobial resistance, climate change, and data management.
As of January 2020, the global outbreak of COVID-19 required a redirection of PHAC resources to support pandemic response efforts. As part of PHAC’s efforts to respond to the pandemic, the Agency played a central leadership role, working with federal, provincial and territorial partners to contain the spread of COVID-19, including through enhanced surveillance, testing, guidance, and public health measures.
Protecting Canadians from serious vaccine-preventable diseases depends on maximizing vaccination uptake. Promoting uptake of all recommended vaccines remained a high priority in the context of concerns about the impact of vaccine hesitancy on coverage rates. Additionally and in response to increasing rates of sexually transmitted and blood-borne infections, an Action Plan was implemented to reduce these incidences by improving access to testing, treatment, care and support. Whether addressing ongoing infectious disease priorities or immediate outbreaks, PHAC continued to focus on providing the latest data, evidence and scientific information required to respond to infectious diseases.
Result 2.1: Infectious diseases are prevented and controlled.
Vaccinations
Vaccinations are one of the most effective public health strategies for protecting populations against infectious disease threats. PHAC continued collaborating with provincial and territorial governments, academia, and professional associations to maximize the impact of vaccination programs.
In 2019–20, PHAC continued to support initiatives aimed at improving vaccination access and uptake by investing over $4.1 million in 17 capacity-building projects through the Immunization Partnership Fund. These projects, which include CANVax and Kids Boost Immunity (KBI), provide evidence-based information to address vaccine hesitancy and increase vaccination knowledge. These programs build the capacity of health care professionals in developing and delivering effective vaccination programs and services that can lead youth in becoming lifelong advocates for vaccination. Since the launch of CANVax in 2018, there have been steady increases in the number of downloads, with overall users at over 17,450 and site visits at 10,185. In 2019-20, there were 1,924 downloads, an increase from 1,066 downloads in the previous year. There was also an increase in users by almost 7,150 and site visit sessions by 12,500 in the previous year.
Since the launch of KBI in 2018, there have been 350 schools registered across Canada, with 2019-20 seeing an increase of 190 schools over the previous year. In 2019-20, 12,040 students used the platform, an increase of over 4,430 from the previous year. Additionally, almost 1.6 million questions were asked, an increase of about 860,000 over 2018-19. Responses to these questions were designed to raise student literacy about the importance of vaccination, COVID-19, and how to avoid misinformation around health topics.
Further, in 2019-20, PHAC also addressed recommendations to ensure timely availability of programmatic information on immunization for provincial/territorial use, as outlined in the Evaluation of Immunization and Respiratory Infectious Disease Activities at PHAC, and supported the National Advisory Committee on Immunization’s expanded mandate to support provincial and territorial vaccination program decisions and improve vaccine access for all Canadians. This included the Advisory Committee Statements on seasonal influenza vaccines and meningococcal B vaccines, which was one of the first national vaccine guidelines to include economic evidence to support vaccine program decisions. Recognizing the potential impact of seasonal influenza, along with COVID-19, on health care system capacity, PHAC supported provinces and territories in procuring additional flu vaccines for the 2020-21 flu season.
Informing Canadians about Public Health Issues
From April to June 2019, PHAC launched Phase 3 of the Childhood Vaccination multimedia advertising campaign comprised of television, social media, search engine marketing, web banners and mobile ads to reach vaccine-hesitant parents and soon-to-be parents. A total of 92,970 unique visitors and 143,860 page views were registered during Phase 3, compared to 40,514 unique visitors and 48,502 page views in Phase 1. In addition, social media had average reach of 4,000 views per post. A post-campaign survey found that 70% of respondents who saw the advertising took action, such as talking with others about vaccination or getting their child vaccinated. The CPHO also participated in a panel discussion with stakeholders on vaccine misinformation that was live-streamed by the Public Policy Forum and shared on the Healthy Canadians Facebook account, that reached over 7,500,000 Canadians.
Antimicrobial Resistance (AMR)
The growing resistance of bacteria to antibiotic drugs is a global public health threat. PHAC coordinated multi-sectoral efforts under a “One Health” approach to combat this challenge. In 2019-20, PHAC worked with federal, provincial and territorial partners and stakeholders in health, animal health as well as the agriculture and agri-food sector to finalize the Pan-Canadian Action Plan on Antimicrobial Resistance and Antimicrobial Use (Action Plan on AMR), including Indigenous Services Canada and the National Collaborating Centre for Aboriginal Health.
When complete, the Action Plan on AMR will provide a blueprint for mounting an effective Canadian response to the threat of AMR through individual actions and the collaboration of Federal/Provincial/Territorial governments, Indigenous partners, and many other stakeholders. PHAC also combatted antibiotic resistance across Canada by engaging national professional and regulatory dental organisations to increase awareness of other options in prescribing antibiotics in dentistry.
Informing Canadians about Public Health Issues
The CPHO’s 2019 spotlight report Preserving Antibiotics Now and Into the Future highlights how unnecessary antibiotic use contributes to antibiotic resistance, why unnecessary use sometimes happens, and what we can do about it. The report was supported by a coordinated communications effort along with the Canadian Food Inspection Agency and Agriculture and Agri-Food Canada. The CPHO Health Professional Forum encouraged its members to participate in the 2019 Antibiotic Awareness Week activities, by amplifying and engaging with social media messages targeted at both the public and antibiotic prescribers and providers, from the National Collaborating Centre for Infectious Diseases and the Public Health Agency of Canada.
Sexually transmitted and blood-borne infections (STBBI)
Prevention, detection, and treatment of STBBI are domestic and global priorities, and Canada is a part of global efforts to eliminate these infections by 2030. In accordance with the Pan-Canadian STBBI Framework for Action, PHAC continued work with federal partners to develop and implement an Action Plan to guide the Government of Canada’s future actions and investments toward eliminating HIV and STBBI. In 2019-20, PHAC released Accelerating our response: Government of Canada five-year action plan on sexually transmitted and blood-borne infections. The Action Plan takes a whole-of-government approach, outlining key federal priorities across ten departments to reduce the public health impacts of STBBI in Canada and advance the work of the Pan-Canadian STBBI Framework from 2019 to 2024. Included in these priorities is commitment to move toward truth and reconciliation with First Nations, Inuit, and Métis Peoples, dismantling stigma and discrimination, and community innovation.
PHAC also initiated the development of domestic STBBI indicators and targets to support the measurement of progress against the goals of the Pan-Canadian STBBI Framework for Action, including stigma, incidence of infection, and access to testing, treatment and ongoing care and support. These indicators, in collaboration with provincial and territorial governments, First Nations, Inuit and Métis partners, and individuals with lived experience, will be appropriate, feasible and measurable.
In support of its commitment to building partnerships and facilitating dialogue on STBBI, in 2019-20 PHAC convened a national discussion on gaps and opportunities for STBBI testing as a mechanism to link to prevention and treatment approaches. In partnership with the Centre for REACH 3.0 and the National Collaborating Centre for Infectious Diseases, the meeting brought together community-based and Indigenous-led organizations, researchers, clinicians, industry, federal and provincial government policy and laboratory representatives. This resulted in a better understanding across sectors of considerations that will need to be addressed to facilitate the implementation of new testing technologies as they progressively receive regulatory approval for use in Canada.
Further, PHAC supported a workshop with 15 organizations seeking to reduce Human Immunodeficiency Virus (HIV) and other STBBI-related stigma, funded under the HIV and Hepatitis C Community Action Fund. This facilitated the sharing of best practices and lessons learned among organizations, and led to the creation of a national Community of Practice on stigma supported by the Centre for REACH 3.0, which now includes 175 members, representing 59 different organizations.
Work also continued in 2019-20 to support the development and dissemination of STBBI-related tools and resources. For example, PHAC developed a series of resources targeting primary health care providers to promote more STBBI testing in order to encourage the greater offer of the treatments pre-exposure prophylaxis and post-exposure prophylaxis and to prevent new infections. This will improve understanding of the scientific evidence supporting the Undetectable = Untransmittable campaign.Footnote 2 This work was augmented by the development of targeted products promoted by front-line service providers for greater awareness of HIV, Hepatitis C, and STI. These resources were shared with national and regional STBBI organizations and promoted widely on social media during a two-week period around World AIDS Day (December 1, 2019). In total, they received 1,785 page views and 675 downloads from external traffic sources during this time. The landing page had a 30% increase in views compared to the previous year and the social media posts received almost 401,375 views, a 238% increase from previous year.
PHAC also distributed new knowledge products, including 20,000 factsheets on the prevention of congenital syphilis among women of childbearing years through 431 community organizations that provide prenatal support to women across Canada, and an e-booklet for youth about STIs, which received 2,030 page views and over 130 downloads in a two-month period following its release. A series of video testimonials featuring people living with HIV were also developed to promote the Undetectable = Untransmittable message. These videos were viewed over 3,440 times in the eight weeks after they were released and shared with global audiences through the Prevention Access Campaign.
Climate Change and Infectious Diseases
Climate change will likely drive an increase in infectious diseases transmitted by, for example, mosquitoes and ticks in Canada. PHAC played a public health role in prevention and detection, and coordinated national responses to inform Canadians about risks and protective measures. In 2019-20, PHAC provided Canadians with information and tools on the prevention and detection of Lyme disease through an education and awareness campaign to help Canadians take action to reduce the health risks associated with this disease. These initiatives provided science and evidence-based information to increase Lyme disease knowledge and support and inform healthy decisions.
Informing Canadians about Public Health Issues
As part of PHAC’s Lyme disease public awareness campaign:
- Over 180,000 products, including posters and handouts, were distributed to provinces, Non-Governmental Organizations, and stakeholders, and were distributed across Canada, including at 25 national parks. An interpreter’s guide was also developed for Parks Canada employees and updated messaging on tick bite prevention was integrated into the Parks Canada mobile application.
- In collaboration with Indigenous Services Canada (ISC), resources were adapted to include design changes to better represent the Indigenous population, resulting in a total of 42,000 wallet cards, posters, pamphlets, and postcards distributed by ISC to Indigenous community partners. Photos and graphic elements were adapted to reflect Indigenous culture and feedback received from the Assembly of First Nations and ISC.
- A digital advertising campaign run during tick season featured messaging focussed on simple actions Canadians can take to protect themselves against Lyme disease. Ads appeared in Facebook sponsored posts, web banner ads on The Weather Network/Météomédia, and family-related sections of CTV news, Sympatico, Canal Vie, etc. The ads allowed high awareness in relevant digital spaces at low-cost, registering 6.8 million impressions.
- The interactive Children’s Travelling Tick ExhibitFootnote 3 was on display at 18 locations in 15 cities across three provinces over the summer months.
- PHAC staff educated over 3,000 Scouts and leaders about Lyme disease and tick bite prevention at the 2019 Scouts Pacific Jamboree in British Columbia. A tailored booth featured a giant 3D tick and real specimens in resin blocks, pull-up banners, tick resources, and a quiz helped youth learn more about ticks and how to prevent tick bites.
- A collaboration with the Canadian Association of Fairs and Exhibitions (CAFE), an organization that oversees 100 fairs and exhibitions across Canada, saw the distribution of Lyme disease awareness resources to their members for display at their exhibitions. In addition, a free quarter page insert on tick bite prevention messages was published in CAFE’s quarterly Canadian Fair News magazine.
In 2019-20, PHAC also supported the implementation of the Pan-Canadian Framework on Clean Growth and Climate Change via PHAC’s Infectious Disease and Climate Change Program through education and awareness, surveillance and monitoring, enhanced laboratory diagnostics, and risk intelligence to better inform and protect Canadians from infectious diseases resulting from climate change across Canada. This work included continuing to build adaptation capacity through the Infectious Disease and Climate Change Fund (IDCC Fund), which invested nearly $2.5 million in seven new projects and the expansion of 4 existing projects. These projects helped build tools and resources to equip health professionals, communities, and Canadians to protect themselves from climate-driven infectious diseases. Funding recipients included:
- The Canadian Public Health Association, which funds the creation of a national forum for knowledge exchange, capacity building and collaboration to address infectious diseases and climate change.
- The Windsor-Essex County Health Unit, which was funded to explore the presence of invasive mosquito species in Leamington, Ontario.
- The First Nations Health Authority project, which funds the British Columbia First Nations Health Authority to undertake work for safe and secure harvesting of marine foods in the context of climate change.
The following four projects from this fund were also completed:
- The Canadian Association of Schools of Nursing released Guidelines for Undergraduate Nursing Education on Climate-Driven Vector-Borne Diseases.
- Centre for Effective Practice launched a new clinical tool and complementary patient handout on Early Lyme Disease Management in Primary Care.
- Institut national de santé publique du Québec developed and delivered ‘train-the-trainer’ training for parks workers on tick identification, collection and Lyme disease prevention.The Northern Ontario School of Medicine (Lakehead University) released competencies and simulation scenarios to help equip resident physicians, and other multi-sectoral health and non-health professional learners with knowledge and skills to support individuals and communities in the prevention and control of extreme weather events-related zoonotic, food- and water-borne infectious diseases.
Knowledge dissemination and outreach events for current IDCC Fund projects in 2019-20 included: 28 media coverage activities; establishment of over 88 multi-sectoral partnerships and/or collaborations; dissemination of nearly 150 knowledge products (e.g. manuals, training materials, videos, website, social media posts, posters); and a total of 109 knowledge exchange events (e.g. presentations, webinars, workshops, committee meetings) attended with an estimated total reach of 8,500 people.
In 2019-20, PHAC also:
- Engaged with the Métis National Council and Governing Members to advance work on health and climate change as part of the Métis' dedicated funding. Projects led by the Métis Nation will be implemented in 2020-21.
- Launched a new multidisciplinary webinar series, “Zoonoses and Adaptation in a Changing World” to increase awareness and knowledge, and establish a dialogue among the zoonosesFootnote 4 and climate change adaptation communities in Canada. Across two webinars, almost 700 individuals registered from academia and clinical practice, as well as from federal, provincial, territorial and municipal governments. A post-event survey indicated approximately 90% of participants agreed the webinars increased their subject knowledge, and the majority of participants believed they could apply some of the strategies and tools discussed to their own work.
Result 2.2: Infectious disease outbreaks and threats are prepared for and responded to effectively.
Rapid and accurate detection of infectious diseases and their causes is a core public health function. During an outbreak, public health stakeholders require the tools, expertise, and protocols to rapidly respond to, and contain, infectious disease from spreading. PHAC focused on making sure that these resources were available to facilitate early detection of outbreaks, as well as delivering a coordinated, timely, and effective response. This was particularly critical in early 2020, with the global outbreak of COVID-19.
COVID-19 Pandemic Response
The emergence of COVID-19, a novel coronavirus first detected in Wuhan, China, triggered an Agency-wide mobilization in pandemic preparedness and response. PHAC’s infectious disease programs immediately focused on risk assessment, early detection, diagnostic test development and the development of guidance on public health measures and infection prevention and control to prevent importation and community transmission of the infection. All these functions were implemented in collaboration with provincial and territorial public health authorities under a coordinated governance structure, the F/P/T Special Advisory Committee on COVID-19, that facilitated effective decision-making and deployment of early actions.
Risk assessment is the foundation for effective preparedness and response. PHAC’s team of epidemiologists conducted regular risk assessments to support public health planning.
Anticipating the risk from international travel in introducing SARS-CoV-2 (virus causing COVID-19) into Canada, the development of digital solutions was initiated to facilitate information collection, sharing and use to support public health action as follows:
- Collaboration with the Canada Border Services Agency on the development of the ArriveCan mobile application, which allows travellers returning to Canada to input their 14-day isolation or quarantine information quickly, easily and securely upon arrival.
- Release of a digital web form to collect traveller contact information on all travellers entering Canada to facilitate local health authorities to contact travellers who may have been exposed to COVID-19 on a flight and trace contacts.
Understanding COVID-19 transmission depends on tracking data over time to identify the characteristics of the disease and associated risk factors. PHAC provided the leadership to standardize data collection by ensuring the establishment of a national surveillance case definition that was adopted by all provinces and territories and formed the foundation for reliable tracking of COVID-19 in Canada. Making data available to the public is a priority. Work was initiated on Situational Awareness Dashboards, to provide online data visualizations of the current state of COVID-19 across the country (e.g., graphs on cases by province and trends over time).
PHAC’s National Microbiology Laboratory (NML) is Canada’s premier laboratory for detecting microbial threats and coordinating country-wide responses to infectious disease threats, working in partnership with provincial public health laboratories. Our laboratory scientists developed Canada’s first diagnostic test for SARS-CoV-2, which was then used to confirm Canada’s first case of COVID-19 on January 27, 2020. As response efforts continued after the initial case, the NML’s specialized laboratory science capacity was utilized to conduct confirmatory testing for all presumed positive samples across Canada. This work informed the NML’s development and communication of quality assurance standards to enable laboratories across the country to conduct accurate and reliable testing. In instances where specimens were difficult to diagnose, the NML’s scientific capacity was applied to resolve these cases.
Global shortages in COVID-19 testing supplies presented significant challenges to Canada’s testing capacity with direct implications for timely diagnosis of COVID-19 and contact tracing. The NML led a coordinated response, working with provincial laboratories, industry, and Public Services and Procurement Canada to plan for and procure testing equipment and supplies in support of provincial/territorial testing strategies. This included bulk purchasing of testing supplies as well as advancing innovation to achieve made-in-Canada solutions to testing supply shortages, working with Innovation, Science and Economic Development Canada. A collaboration with LuminUltra, a Canadian biotechnology company, was established to manufacture testing reagent according to a protocol developed by scientists at the NML. By filling this gap, the Government of Canada facilitated the delivery of testing across the country.
Under the Government of Canada’s repatriation initiatives to bring Canadians stranded abroad back to Canada, the laboratory testing services of the NML were deployed via a mobile laboratory team to Cornwall and the Canadian Forces Base in Trenton. On site, real-time diagnostics were provided to support detection of infection for those quarantined for 14 days on their return to Canada.
The NML’s role in developing animal models of SARS-COV-2 infection is essential to testing new therapeutics and vaccines. Working in collaboration with industry and academia, NML scientists brought their expertise in virology and genomics to bear in initiating a COVID-19 program of research to answer important questions. Seventeen research projects were initiated in the January-March timeframe to:
- Develop animal models to support pre-clinical studies of therapeutics and vaccines.
- Investigate the effectiveness of methods to inactivate the virus (e.g., sunlight exposure, gamma radiation).
- Evaluate medical mask disinfection protocols.
- Evaluate the length of survival of SARS-CoV-2 on surfaces commonly found in healthcare facilities.
- Develop vaccine candidates and monoclonal antibodies.
- Validate serological test assays.
In order to evaluate the evidence available for possible intermediary animal host(s) of COVID-19 emergence in humans in China, and possible human-to-animal transmission that could then lead to the creation of a possible animal reservoir going forward (thus posing a risk of animal-to-human zoonotic transmission in the future), a variety of activities were conducted from early January to late March 2020. For example, scientific assessment of possible zoonotic origin of virus and evidence of infection in animals, and rapid risk assessments were conducted including human and companion animals.
PHAC’s specialists in infection and prevention and control mounted a dedicated effort to develop evidence-based guidance on infection prevention and control in acute care settings. This expertise was also deployed to Cornwall and Trenton to lead and support quarantine requirements in support of the safe return of repatriated Canadians. With the occurrence of outbreaks in specific populations, PHAC experts provided training and evaluation of institutional preparedness with respect to infection prevention and control standards and procedures. Specifically, working with federal partners, PHAC assisted in ensuring the COVID-19 preparedness of federal correctional facilities across Canada in order to prevent infection among inmates and staff. A collaboration with Service Canada/Employment and Social Development Canada evaluated best practices for preventing COVID-19 infection among Temporary Foreign Workers on agricultural sites in Ontario.
To aid in developing critical early guidance and communications regarding the pandemic and the spread of COVID-19, PHAC’s Public Health Measures team collaborated with expert advisory groups, consisting of members from across Canada specializing in pandemic preparedness, infectious diseases and public health, to produce initial tools and resources to inform Canadians:
- Five initial guidance documents were developed to assist public health professionals in controlling outbreaks in Canada, focused on mitigating the spread of COVID-19 in communities, public health management of cases and contacts, guidance for schools and childcare programs, and guidance for providers of people experiencing homelessness.
- Eleven communications products were disseminated to inform and educate Canadians about the new virus, including what they can do to protect themselves, their families, and communities (e.g., Vulnerable Populations and COVID-19; Be Prepared; Know the Difference: Self Monitoring, Self-Isolation, Isolation).
- Two risk assessment tools were created to provide a framework for assessing risks related to gatherings/events, and outline public health measures to mitigate risks as well for workplaces/businesses.
Accomplishments during the last quarter of the 2019-20 fiscal year set the foundation for a sustained COVID-19 response that evolved based on emerging scientific evidence and on the epidemiology of the infection across the country.
Scientific Leadership and Laboratory Capacity
PHAC continued to provide national laboratory capacity, as well as provide science leadership and services to test for new pathogens of national and international concern.
In 2019-20, PHAC also provided guidance and worked with provincial public health laboratories to transition to a national approach to genomics-based testing methods for infectious diseases, specifically:
- The Canadian Public Health Laboratory Network undertook a systematic assessment of federal and provincial public health laboratory capacity to start the process of identifying barriers and future needs in order to develop a nation-wide vision on the usage of innovative diagnostic technologies.
- PulseNet Canada detected a significant reduction in Salmonella Enteritidis, a major cause of foodborne illness, in 2019-20. The successful implementation of Whole Genome Sequencing in previous years was instrumental for improved identification and tracing capacity for this pathogen.
- Over $1.2 million was invested to upgrade hardware and software for Integrated Rapid Infectious Disease Analysis (IRIDA), a web application for the storage, management, analysis, sharing, and reporting of public health genomic data and accompanying metadata, to increase its storage capacity, improve data handling capabilities, enhance security, and enable external modifications.
- In the past year, PHAC’s National Microbiology Laboratory processed approximately 7.5 million system queries related to genomics and bioinformatics analysis underpinning a range of research, diagnostic, and outbreak detection and response activities. These improvements will allow partners to customize IRIDA for their genomic data needs while also improving efficiency for various components of the application itself.
PHAC also established the virtual Innovative Diagnostics Program starting with addressing gaps in HIV/tuberculosis (TB) diagnostic testing in priority areas where commercial tests are unavailable (e.g., vulnerable and remote populations) by:
- Improving testing capacity for TB in remote regions by providing targeted TB screening clinics in two Inuit communities, Cape Dorset, Nunavut and Kangiqsualujjuaq, Quebec. These clinics deployed expertise, training and diagnostic services for the communities to address immediate needs and prevent future outbreaks.
- Continuing to expand Dried Blood Spot testing capacity to provide a more reliable and efficient testing option for remote regions. National Microbiology Laboratory scientists provided training and testing services across seven provinces for HIV, human papillomavirus (HPV), Hepatitis C, and syphilis.
As part of its ongoing work to enhance the diagnosis of infectious diseases, PHAC brought together experts to develop an international consensus on the use of next generation sequencing for HIV drug resistance. Specifically, building on the internationally recognized ‘Winnipeg Consensus’ guidelines for HIV drug resistance data processing, PHAC scientists continued to work with domestic and international partners to identify challenges and share best practices in the field of HIV drug resistance testing, surveillance, and analysis.
Tuberculosis (TB)
- TB continued to affect individuals, families and communities. In particular, Indigenous Peoples and foreign-born Canadians remained at increased risk for this disease. PHAC undertook a number of initiatives aimed at reducing rates of TB in at risk populations. In 2019-20, PHAC conducted national surveillance of active TB disease and drug resistance to monitor progress towards TB elimination. As part of this work, PHAC:
- Reported on TB drug resistance trends across Canada to inform policy and practice, reaching an audience of more than 5,000 individuals with an interest in public health.
- Supported the work of Inuit Tapiriit Kanatami and partners to eliminate TB in Inuit Nunangat by 2030 by providing customized datasets on the incidence of active TB disease in the four Inuit regions.
- Continued to work collaboratively with provincial and territorial ministries of health to monitor TB trends at the national level.
PHAC also worked with Immigration, Refugees and Citizenship Canada (IRCC) to initiate and implement a change in policy to enhance testing for latent TB infection (LTBI) among at-risk migrants in partnership with selected provinces. Specifically, PHAC worked with IRCC to implement a highly targeted screening initiative for LTBI, aimed at increasing the number of migrants being referred for follow up in Canada upon arrival.
In 2019-20, PHAC also invested over $500,000 to support two community-based initiatives aimed at increasing awareness about, and reducing stigma related to, TB among at-risk newcomers to Canada in order to proactively facilitate access to diagnosis and treatment. These projects reached over 2,500 individuals through the dissemination of materials aimed at increasing awareness about TB (including local resources) and diminishing stigma. As part of these initiatives, funding recipients:
- Provided training to more than 50 community service professionals on culturally appropriate methods to engage newcomers to Canada on TB prevention.
- Engaged diverse groups of community members from different ethno-cultural backgrounds, age groups, and gender identities in two provinces (Ontario and British Columbia) to obtain their input and perspective on TB awareness and stigma. This helped identify knowledge gaps, stigma surrounding testing for TB, and barriers to treatment in communities of newcomers to Canada from countries with high rates of TB.
- Created culturally appropriate and linguistically accessible information resources for newcomers and their families at risk for developing active TB disease, including knowledge translation tools and educational materials aimed at reducing stigma, improving access to TB services, and building awareness among health care providers and their clients.
Foodborne Illness
In 2019-20, PHAC continued to support investigations of food outbreaks and the analysis of foodborne illness trends aimed at improving food safety. PHAC maintained timely detection and response to foodborne illness outbreaks based on laboratory testing, data, and analysis. This included the assessment of 312 events, leading and supporting multi-jurisdictional outbreaks, completing 21 post-outbreak debrief items, facilitating training, developing 24 knowledge transfer products, and presenting to over 600 stakeholders, including federal, provincial, territorial and local public health partners, industry, and academia. PHAC also:
- Supported the assessment and response to 20 national outbreak investigations through the National Enteric Surveillance Program (NESP), which collects and analyzes weekly enteric disease data from all provincial public health microbiology laboratories to support outbreak detection and response.
- Enhanced the ability for the detection, targeted investigation, response, and control measures of a potential source of illness. Through the retail food sampling components of FoodNet Canada and the Canadian Integrated Program for Antimicrobial Resistance Surveillance (CIPARS), 169 food samples were linked to 37 foodborne outbreak clusters.
- Assessed foodborne illness trends to inform public health action, and enable Canadians to make informed decisions to protect themselves from foodborne illness. This included providing data from NESP, FoodNet, and CIPARS. This data informed working groups, Canadians, and stakeholders, and was used to prioritize risks, assess the effectiveness of activities, and advance policy, among other priorities.
Innovation and Experimentation
PHAC continued conversations to explore the feasibility and use of drones to expand access to innovative STBBI diagnostic testing options for Northern/Remote/Isolated communities across Canada; however, COVID-19 response efforts have led to the deferral of previously planned activities for this initiative.
Through the Innovative Solutions Canada program, PHAC worked with Canadian businesses to develop and test software that uses artificial intelligence to create an interactive portal for the Canadian Immunization Guide. This interactive portal made it easier for Canadians to search and find custom and trustworthy answers to their vaccine questions (based on the expert and evidence-based guidance of the National Advisory Committee on Immunization) and addressed gaps in vaccination knowledge and beliefs. Three successful companies completed their Phase 1 proof of concept reports, which include a summary of their strategy and test results. There are strong early signals from the proof of concept that this technology can produce accurate and meaningful answers to vaccine questions based on government content.
To improve the accessibility of its surveillance data for multiple purposes, audiences, and end users, PHAC experimented with new ways of providing data on foodborne illnesses and antimicrobial resistance to stakeholders. The CIPARS reformatted its annual report for foodborne illness and antimicrobial resistance to make it more concise and visual, while maintaining the delivery of specific data needed by many partners and stakeholders. This change improved the timeliness of surveillance data delivery and contributed to progress in experimenting with data delivery methods. Providing surveillance data in an interactive manner streamlined the transition of data to stakeholders and provided flexibility in custom analysis based on their specific needs.
Sex and Gender-based Analysis Plus
As an integral component of program development, monitoring and evaluation, SGBA+ was more systemically integrated into surveillance activities, science, policy and programs at PHAC throughout the 2019-20 fiscal year. This integration was expressed through activities including the survey data collected on vaccination estimates, as well as the annual surveillance reports on rates of STBBI, which identified factors such as sex and sexual orientation as key socio-demographic determinants of immunization status and infection rates respectively. The annual STI surveillance reports also contain data for syphilis, chlamydia and gonorrhea disaggregated by sex and age group for all provinces and territories.
HIV surveillance, in particular, has a longstanding history of reporting on characteristics such as age, sex, sexual orientation (for men who have sex with men) and injection drug use. This year, the HIV surveillance program continued its efforts to collect more complete information on race/ethnicity (including Indigenous status and residence on or off reserve for First Nations individuals), and individuals who acquired HIV through transactional sex.
In 2019-20, two surveillance reports were published in the Canadian Communicable Disease Report that provided information on key populations most affected by STBBI. These reports described participants’ gender identity, sexual identity, as well as other social determinants of health, including financial and housing stability, and experiences of stigma and discrimination.
Through the incorporation of a SGBA+ in initiatives such as these and more, it becomes apparent that infectious diseases and other illnesses are not experienced in the same way or to the same extent across Canada, but rather are shaped by social determinants of health. As such, efforts are ongoing to enhance SGBA+ implementation through continued analysis of sex, gender, age, and other identifying factors to inform program responses. This work includes targeted awareness campaigns and communications to address population specific health risk and enhanced surveillance tracking.
Sex and gender are key socio-demographic variables collected in all of PHAC’s immunization surveys. For example, the 2017 childhood National Immunization Coverage Survey, and both 2017-18 and 2018-19 seasonal influenza surveys, included sex and gender as a key socio-demographic determinant of immunization status. In alignment with the Policy Direction to Modernize the Government of Canada’s Sex and Gender Information Practices, non-binary gender data was collected. For example, in all three surveys, a statistical analysis comparing immunization rates between males and females was conducted.
The SGBA+ did not affect the collection of data in immunization surveys, but it did affect the analysis and presence of sex disaggregated tables and results in our published reports. Differences in vaccination coverage by sex and gender will be analyzed and presented in all future immunization coverage surveys. Published results may help to provide information on the most appropriate target groups for vaccine promotion efforts. SGBA+ also forms part of the target audience selection process for vaccination campaigns. For example, as women are often the primary health-care decision-makers within the family and are heavy social media users who seek out and share health advice from others, digital advertising is geared towards women and mothers.
While projects conducted under the Immunization Partnership Fund (IPF) focus generally on under- and unvaccinated populations, some projects target groups within these populations that may lack knowledge or awareness of vaccination schedules, or experience challenges or barriers in accessing vaccines, such as Indigenous People, newcomers to Canada, single parents, and young mothers. However, IPF project reporting does not specifically address health inequities or profile the target audience for their interventions.
| Departmental Results | Departmental Result Indicators | Target | Date to achieve target | Actual results | ||
|---|---|---|---|---|---|---|
| 2019-20 | 2018-19 | 2017-18 | ||||
| Infectious diseases are prevented and controlled | % of 2 year old children who have received all recommended vaccinationsFootnote a | 95% | Dec. 31, 2025 | 68% | Data not collectedFootnote b | 68% |
| Proportion of national vaccination coverage goals met for children by 2 years of ageFootnote c | 7/7Footnote d | Dec. 31, 2025 | 1/12 (2017) |
Data not collectedFootnote e | 0/12 (2015) |
|
| Rate per 100,000 of new diagnosed cases of Human Immunodeficiency Virus (HIV) | 0.6 Cases per 100,000 |
Mar. 31, 2030 | Data available in December 2020 | 6.5 (2017) |
||
| Rate of a key antimicrobial resistant infectionFootnote f identified among people in hospitals | 2 cases per 1,000 patient admissions | Mar. 31, 2020 | Data available in late 2020 | 0.61 per 1,000Footnote g (2017) | ||
| Infectious disease outbreaks and threats are prepared for and responded to | % of foodborne illness outbreaks responded to within 24 hours of notification | 90%Footnote h | Mar. 31, 2020 | 98% | 91% | 95% |
| % of new pathogens of international concern that Canada has the capacity to accurately test for | 90% | Mar. 31, 2020 | 100% (2019) |
100% (2018) |
100% (2017) |
|
|
||||||
| 2019–20 Main Estimates |
2019–20 Planned spending |
2019–20 Total authorities available for use |
2019–20 Actual spending (authorities used) |
2019–20 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 207,886,062 | 207,886,062 | 261,470,040 | 257,498,145 | 49,612,083 |
Authorities available for use increased during the fiscal year mainly due to funding approved in response to the COVID-19 pandemic. Actual spending varied from planned spending primarily due to the new funding received.
| 2019–20 Planned full-time equivalents |
2019–20 Actual full-time equivalents |
2019–20 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 1,008 | 1,054 | 46 |
3. Health Security
Description
Prepare for and respond to public health events and emergencies (e.g., floods, forest fires, and outbreaks such as Zika and Ebola); address health and safety risks associated with the use of pathogens and toxins; and address travel-related public health risks.
Results
Under this Core Responsibility PHAC is focused on advancing the following Departmental Results:
- Public health events and emergencies are prepared for and responded to effectively.
- Public health risks associated with the use of pathogens and toxins are reduced.
- Public health risks associated with travel are reduced.
Up until December 2019, PHAC focussed on advancing planned work to strengthen Canada’s ability to prepare for and effectively respond to public health events and emergencies, including the development of an action plan to address recommendations from the World Health Organization (WHO)/Pan American Health Organization (PAHO) Joint External Evaluation (JEE) conducted in 2018. It also met its risk-based compliance and enforcement responsibilities in the areas of biosecurity and biosafety and maintained its conveyance inspection regulatory regime to reduce public health risks associated with travel.
In January 2020, in response to COVID-19, PHAC redirected human and financial resources to support pandemic response efforts. PHAC played a central leadership role, working with federal, provincial and territorial partners to contain the spread of COVID-19, including through enhanced quarantine and border measures and supporting repatriation operations by deploying assets from its National Emergency Strategic Stockpile (NESS) as well as deploying skilled staff and establishing protocols and contracts to support operations and ensure health security.
Result 3.1: Public health events and emergencies are prepared for and responded to effectively.
In 2019-20, PHAC developed a draft National Action Plan for Health Security (NAPHS) in consultation with federal, provincial and territorial partners. The NAPHS addresses recommendations from the WHO/PAHO JEE conducted in 2018. While the JEE determined that Canada has in place the capacities needed to fully implement the International Health Regulations (IHR), the NAPHS focusses on a subset of recommendations to further strengthen Canada’s health security capacity and demonstrate improvement for the next JEE (e.g., Antimicrobial Resistance Detection and Stewardship Activities; Vaccine Coverage; and Risk Communication [Dynamic Listening and Rumour Management]). Efforts to advance work set out in the action plan were delayed due to COVID-19.
In addition, PHAC planned a series of exercises to test the Federal/Provincial/Territorial Public Health Response Plan for Biological Events using a pandemic influenza scenario (the Flu NOVA Exercise). The Agency sponsored an initial planning conference in October 2019, resulting in plans for an Awareness Seminar, a Notification Drill, a Table Top Exercise(s), and a Command Post Exercise. Ninety-six individuals participated, including eighteen provincial/territorial representatives covering pandemic influenza, emergency management and public health. While the Flu NOVA exercise was paused in 2020 due to COVID-19, the work to date has informed the current and ongoing pandemic response.
Further, from lessons learned and provincial/territorial dialogue, PHAC developed and designed a Northern Ready Mini-Clinic conceptual model to support the health emergency surge capacity needs of Canada’s northern and remote communities. A federal/provincial/territorial workshop was held to advance the conceptual model and inform the development of prototypes for testing and validation.
DID YOU KNOW?
In 2019-20, PHAC mobilized staff in response to 14 domestic requests for assistance to investigate and manage disease outbreaks for legionnaire’s disease, measles, rabies, salmonella, syphilis, cancer, and substance related harm. PHAC also deployed 16 staff members (epidemiologists, emergency management officers, and specialists in infection, prevention & control and border health) to Brazzaville (Congo), Geneva (Switzerland) and Goma (Democratic Republic of Congo) to support Ebola response efforts, coordinated by the World Health Organization.
With the onset of COVID-19 in January 2020, PHAC mobilized staff to support the federal health response, and officially activated the Health Portfolio Operations Centre in January 2020. As part of response efforts, PHAC has:
- Activated the Federal/Provincial/Territorial Response Plan for Biological Events and associated governance to enable collaboration and collective action (i.e., the Special Advisory Committee, Technical Advisory Committee, and Logistics Advisory Committee) across jurisdictions to facilitate an efficient, timely and consistent approach to COVID-19 response activities.
- Led Government of Canada efforts to bolster the Canadian supply of personal protective equipment (PPE). This amounted to an investment of approximately $186 million as of March 31, 2020 to purchase PPE, such as:
- over 5.5 million N-95 respirators and equivalents;
- over 8 million surgical masks;
- 6 million face shields; and
- 2 million gowns.
- Deployed PPE and medical devices, such as ventilators from the NESS in response to 20 urgent requests for assistance from provinces and territories. Amount of PPE included:
- Over 35,000 N95 respirators;
- Over 59,000 surgical masks;
- 140,000 face shields; and
- 40,000 gowns.
- Continued the growth and redevelopment of the NESS program. The NESS was initially built on the basis that provincial, territorial and local governments would be prepared for the most common emergencies. Accordingly, it was designed to provide health emergency assets when provincial, territorial and local resources were exhausted. With the unprecedented nature of the current pandemic, the NESS quickly stepped into a more active role in the procurement of PPE and other medical supplies.
- Activated Regional Emergency Coordinating Centres in each PHAC region to coordinate mobilization/response activities and manage local issues and stakeholder engagement. This structure mirrors that of HPOC.
- Deployed public health officers and field epidemiologists in response to requests for assistance at the federal and provincial level, supporting a wide range of surveillance activities and outbreak investigations related to COVID-19 response. Additionally, some public health officers were refocused from original projects to provide support to COVID-19 response at their provincial and territorial placements.
Result 3.2: Public health risks associated with the use of pathogens and toxins are reduced.
In 2019-20, PHAC continued to assess compliance of Canadian laboratories with the Human Pathogens and Toxins Act and supporting Human Pathogens and Toxins Regulations through on-site inspections and document reviews. Of all compliance issues identified, 98% were successfully responded to by regulated parties within established timelines. PHAC met or surpassed its annual inspection targets for all licence types.Footnote 5
As part of ongoing efforts to strengthen regulatory oversight and promote compliance, in 2019-20 PHAC:
- Developed a standardized, annual process to assess and validate the criteria used to plan and prioritize the inspection of Risk Group 2 and Risk Group 3Footnote 6 licensed laboratories so that resources can be allocated to areas of greatest risk.
- Piloted a new portable electronic solution for on-site inspections to streamline inspection and reporting processes. The project was placed on hold to focus on COVID-19 pandemic response efforts.
- Worked closely with regulated parties to promote compliance through training and targeted information sessions to enhance understanding of regulatory requirements. This included piloting virtual workshops to widen training reach and better meet the expressed needs of regulated parties.
- Conducted outreach and engagement activities to sensitize regulated parties to the increased transparency of regulatory operations. This included leveraging Health Canada’s Drug and Health Products Inspection Database, which will facilitate the publishing of laboratory biosafety and inspection information on the Open Government portal starting in fiscal year 2020-21.
PHAC also continued with initiatives to advance global health priorities in the areas of biosecurity and biosafety. With funding from Global Affairs Canada’s Weapons Threat Reduction Program, PHAC, as a WHO Collaborating Centre for Biosafety and Biosecurity, launched the Analytical Approach to Biosafety and Biosecurity as an online e-course available in French and English. This modular, scalable policy toolkit provides practical guidance to help other countries establish or strengthen their national or regional policies and oversight frameworks for pathogen biosafety and biosecurity.
In order to prioritize resources to COVID-19, four biosafety guidelines and one biosafety directive planned for publication in late 2019-20 were postponed. PHAC also postponed the public consultation on the final draft of the third edition of the Canadian Biosafety Standard planned for March 2020. PHAC completed a COVID-19 Biosafety Advisory to support local risk assessments and assist clinical, diagnostic, and research laboratories in implementing proper biosafety procedures to handle samples that may contain the virus that causes COVID-19.
Result 3.3: Public health risks associated with travel are reduced.
In support of its mandate to manage travel-related public health risks on passenger conveyances and at the border, PHAC delivered on the following commitments in 2019-20:
- Communicating existing and emerging travel health risks through increased social media, media, and travel industry outreach. This included targeted material related to Middle East Respiratory Syndrome Coronavirus (MERS CoV) for travellers participating in the Hajj or Umrah pilgrimages; and, three articles and one radio spot on the prevention of travel health risks.
- Conducting 332 risk-based inspections of conveyances (aircraft, passenger ferries and trains, cruise ships), during which 220 critical violations were identified and subsequently actioned and resolved by service providers.
- Implementing and staffing the Central Notification System quarantine contact line that provides remote access to communicable disease health experts to respond to and manage travel-related public health enquiries at Canadian points of entry, 24 hours a day, seven days a week.
- Strengthening Canada’s public health capacity to respond to a potential case of a traveller with Ebola virus disease arriving in Canada, including through a table-top exercise with the Canada Border Services Agency.
In addition to delivering on its 2019-20 DP commitment, PHAC led the federal response when COVID-19 was declared a public health emergency of international concern on January 30, 2020. As the COVID-19 outbreak evolved, PHAC took a strong and comprehensive approach to minimizing the risk of importation and spread by implementing new measures at the border, advising Canadians to avoid all non-essential travel, prohibiting all travel to Canada with some limited exceptions, and asking all travellers who enter Canada to self-isolate. This required the implementation of nine Emergency Orders under the Quarantine Act; extensive and close consultation and collaboration with federal, provincial and territorial counterparts and industry; and the reprioritization and deployment of significant financial and human resources.
PHAC posted the first travel health notice for Wuhan, China on January 7, 2020, with additional notices following for mainland China and other countries experiencing outbreaks of COVID-19, and ultimately leading to a global COVID-19 Travel Health Notice advising travellers to avoid all cruise-ship travel and all other non-essential travel outside of Canada.
PHAC supported the implementation of enhanced border measures starting January 22, 2020, which included:
- Working with the airline industry to inform aircraft passengers of obligations under the Quarantine Act and to provide guidance on aircraft disinfection and sanitation.
- COVID-19 communications materials displayed in airports and handouts to all travellers about quarantine or isolation obligations.
- Development and integration of guidelines and traveller questionnaires into the screening protocols at Canadian airports and at land border kiosks.
- A new increased front-line presence and service at points of entry to Canada, including the training and deployment of additional quarantine officers, screening officers, and information officers to Canadian points of entry.
In February-March 2020, PHAC worked with other government departments and provincial/local counterparts on a number of extraordinary federal efforts to repatriate approximately 750 Canadians from Wuhan, China, the Diamond Princess Cruise Ship in Tokyo, Japan, and the Grand Princess Cruise Ship in San Diego, USA. Additionally, PHAC, in collaboration with other government departments such as the Canadian Armed Forces, led the rapid establishment of three large-scale federal quarantine operations to house and care for repatriated Canadians during their 14-day quarantine period.
On March 18, 2020, PHAC initiated a series of Emergency Orders in Council under the Quarantine Act to close Canada’s borders; first to all foreign nationals, with the exception of U.S. citizens, then to all foreign nationals entering Canada from the US for non-essential travel, and finally, to all travellers exhibiting COVID-19 symptoms. On March 25, 2020, PHAC implemented an Emergency Order under the Quarantine Act requiring all travellers entering Canada to self-isolate/quarantine for 14 days. PHAC also established designated quarantine sites in key locations across Canada to accommodate returning Canadians who were unable to make suitable arrangements to meet isolation requirements. PHAC’s Regional Operations met this unprecedented need, within a rapidly changing environment and with unique challenges faced by the industry, service providers and non-government partners that were mobilized to support operations. In parallel, PHAC stood-up a new unit to promote and enforce compliance with the Order.
The combination of travel health notices, advisories and Emergency Orders reduced the volume of travellers arriving at Canada’s airports, ports and land borders by approximately 95%. This led to reduction in the daily number of imported COVID-19 cases.
Innovation and Experimentation
PHAC’s Global Public Health Information Network (GPHIN) continued using artificial intelligence to support early detection and warning for global public health threats, through active search and monitoring approaches aimed to discover patterns, trends, anomalies, and novel connections. The Situational Awareness Daily Report produced by GPHIN was revamped based on a user satisfaction survey in Spring 2019. The scope of the report is more relevant to public health professionals and contains additional analysis – facilitating early detection, identification and monitoring of emerging global health events. For example, GPHIN first reported on what would later be called COVID-19 in the Situational Awareness Daily Report of December 31, 2019. An independent review of the GPHIN system will be undertaken to assess the effectiveness of the system and recommend improvements to enhance its utility as an early warning system for public health events of concern.
PHAC was responsible for establishing quarantine sites across the country in an expedited manner as the COVID-19 response evolved at a rapid pace. This occurred in a context of great uncertainty related to the virus as well as the availability of service providers. This was an unprecedented effort for PHAC.
Sex and Gender-based Analysis Plus
During the 2019-20 fiscal year, a greater emphasis was put on a SGBA+ at PHAC through its incorporation into national-scale initiatives including the NESS and the Border and Travel Health Program. Although varying in nature, the programs were unified in their considerations of sex and gender as contributory factors to program execution. Within the scope of the NESS, consideration was taken into the user of a product (i.e. a pregnant woman, a child, a young adult). In a similar manner, gender was taken into account when developing communications products such as travel health notices for the Border and Health Travel Program. Where possible, pronouns used remain gender neutral and gender-specific health risks are noted accordingly. Taken together, the integration of social determinants such as sex and gender into PHAC initiatives has enabled the facilitation of more inclusive health programs.
Modifications have also been made to ensure gender inclusivity in forms used for the Biosecurity Program, which works to protect the health and safety of the public against the risks posed by human and terrestrial animal pathogens and biological toxins. The program requires a Human Pathogens and Toxins Act (HPTA) security clearance for individuals working with certain high risk toxins. In 2019, the form used to collect personal information for the HPTA clearances was modified to include a non-binary gender specification (X, or unspecified) in the gender information data collection section. This change is consistent with government-wide efforts to modernize sex and gender information practices, and supports PHAC’s commitment to ensure its policies, programs and initiatives are inclusive of all individuals.
During the scientific competencies module in November 2019, participants received training with respect to Indigenous People in addition to public health training on qualitative analysis and storytelling with public health data. While SGBA+ is not directly addressed, principles of SGBA+ are raised in the form of case studies and small group discussions. For example, participants are asked to think about characteristics of the population that could be involved in a potential outbreak, and as such discussion around different cultural practices (including cultural foods) and unique populations may come up in the facilitated group discussions and hands on exercises.
The content of the scientific competencies module varies and has previously included dedicated training on SGBA+. The next scheduled offering is set to take place in 2021. While the training is geared towards the Canadian Field Epidemiology Program, Public Health Officers with the Canadian Public Health Service have been invited to participate.
| Departmental Results | Departmental Result Indicators | Target | Date to achieve target | Actual results | ||
|---|---|---|---|---|---|---|
| 2019-20 | 2018-19 | 2017-18 | ||||
| Public health events and emergencies are prepared for and responded to effectively | Canada’s readiness to respond to public health events and emergencies as assessed independently by the World Health Organization | 4 (Rating out of 5) |
Mar. 31, 2020 | 4.5Footnote * | 4.5 | Not availableFootnote a |
| % of provincial and territorial requests for assistance responded to within negotiated timelines | 100% | Mar. 31, 2020 | 100% | 100% | 100% | |
| Public health risks associated with the use of pathogens and toxins are reduced | % compliance issues in Canadian laboratories successfully responded to within established timelines | 85% | Mar. 31, 2020 | 98% | 88% | 82% |
| Public health risks associated with travel are reduced | Canada’s capacity for effective public health response at designated points of entry into Canada | 4 (Rating out of 5) |
Mar. 31, 2020 | 5Footnote * | 5 | Not availableFootnote a |
| % of inspected passenger transportation operators that meet public health requirements | 95%Footnote b | Mar. 31, 2020 | 96% | 94%Footnote c | 97% | |
|
||||||
| 2019–20 Main Estimates |
2019–20 Planned spending |
2019–20 Total authorities available for use |
2019–20 Actual spending (authorities used) |
2019–20 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 52,331,185 | 52,331,185 | 249,021,203 | 248,500,491 | 196,169,306 |
Authorities available for use increased during the fiscal year mainly due to funding approved in response to the COVID-19 pandemic. Actual spending varied from planned spending primarily due to the new funding received.
| 2019–20 Planned full-time equivalents |
2019–20 Actual full-time equivalents |
2019–20 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 381 | 385 | 4 |
Financial, human resources and performance information for PHAC’s Program Inventory is available in the GC InfoBase.
Internal Services
Description
Internal Services are those groups of related activities and resources that the federal government considers to be services in support of Programs and/or required to meet corporate obligations of an organization. Internal Services refers to the activities and resources of the 10 distinct services that support Program delivery in the organization, regardless of the Internal Services delivery model in a department. These services are: Management and Oversight Services; Communications Services; Legal Services; Human Resources Management Services; Financial Management Services; Information Management Services; Information Technology Services; Real Property Management Services; Materiel Management Service; and Acquisition Management Services.
Results
Under Internal Services PHAC is focused on advancing the following results:
- Building a healthy, diverse and inclusive workforce.
- Modernizing the workplace to enable a safe and productive workforce with access to modern tools and facilities.
- Enhancing the use of data and improving information sharing.
- Pay system stabilization.
- Informing Canadians about public health issues.
- Building a results-based management culture.
To make progress towards achieving these results, PHAC focused its 2019-20 efforts on key initiatives and activities that promoted diversity and employment equity, facilitated remote working, enhanced accessibility and ensured that no employee faces financial hardship because of a Phoenix pay issue.
Building a healthy, diverse and inclusive workforce
PHAC undertook a number of initiatives this past year to help foster a more agile and inclusive workforce in the spirit of Blueprint 2020, Beyond 2020 and Public Service Renewal.
To support a culture of innovation and experimentation, PHAC employees were encouraged and supported to innovate, experiment, and take smart-risks by offering hands-on learning and development opportunities, removing barriers to collaboration, and sharing best and promising practices. For example, PHAC’s 8-week hands-on learning Fundamentals of Innovation Program helps employees develop the mindset, toolset, skillset and network to innovate when delivering on PHAC’s business. As of December 2019, three cohorts had completed the program.
In 2019-20, the first learning symposium on innovation and experimentation was also held and attracted more than 500 public servants from across the Health Portfolio and several departments. Employees participated in interactive exhibits, plenary sessions and workshops where they heard from experts in and out of government on how to cultivate the mindset, skills and behaviours needed to foster more innovation and experimentation in their work.
A talk-show style Health Talks event to celebrate the 100th anniversary of the creation of Canada’s first federal department of health took place in November 2019. The Health Talks looked at pivotal health moments in the past, the innovations they sparked, and what the future holds for health innovation in Canada. More than 300 employees attended the event in person or by video.
An ambitious communications initiative was launched to help PHAC employees identify and access the corporate wellness resources that best meet their needs. This initiative included both print and web-based tools, and involved considerable engagement with employees directly and through various governance tables. Results from the 2019 Public Service Employee Survey indicated a 5% decrease in employees who felt that their stress level was high/very high and a 5% decrease for those who felt emotionally drained at the end of the workday. While the project was paused due to COVID-19, the Agency created a new wellness page on Canada.ca, providing employees with resources and services.
In 2019-20, PHAC sustained efforts to meet the requirements under the departmental Multi-Year Diversity and Employment Equity Plan in order to close employment equity gaps. For example, an Inclusive Recruitment Guide was developed for managers and Human Resources Advisors to support diversity goals. An Accessibility Readiness Team was also created to support the requirements of the Accessible Canada Act and the Federal Accessibility Strategy. In addition, PHAC:
- Designed new streamlined tools and resources that support managers, management teams, employees and students in managing learning, onboarding experience and employee performance.
- Streamlined access to services related to accommodating persons with disabilities, illnesses and injuries, disability management, the reporting of occupational health and safety incidents and accidents.
- Utilized employment equity staffing inventories such as Employment Opportunity for Students with Disabilities Program, Indigenous Student Employment Opportunity, Federal Internship for Newcomers Program and the LiveWorkPlay initiative to recruit and hire a diverse workforce.
- Continued to support employment opportunities for students and fostered an inclusive work environment that attracts, retains and utilizes their talent. Diversity of hiring was facilitated through student bridging and post-secondary recruitment. Thirty indeterminate appointments were made via these mechanisms, supporting employment opportunities from a variety of diverse universities and areas of expertise.
- Collaborated with employee networks to provide learning sessions for their members, including the Visible Minorities Network on career management (79 participants).
- Implemented the Indigenous Learning Strategy, which entails the promotion of Canada School of Public Service Indigenous-related courses.
- Promoted bilingualism through the organization of various events and a post-secondary recruitment strategy that includes publicizing departmental career opportunities at French speaking institutions.
Efforts were also made in 2019-20 to facilitate more inclusive engagement of external stakeholders. Sessions to distill, record and disseminate learnings enabled the development and sharing of best practices to better engage groups in policy and program consultations, such as Indigenous Peoples, and people with living and lived experience. For example, the annual Orange Shirt Day event was organized in consultation with the PHAC Indigenous Working Group and the PHAC Indigenous Employee Network.
Modernizing the workplace to enable a safe and productive workforce with access to modern tools and facilities
In 2019-20, PHAC continued to modernize the workplace in order to enable a safe and productive workforce, providing employees with access to modern tools and facilities. Highlights include:
- A Digital Modernization Framework was developed and approved for use in making strategic investments in shifting to a digital government.
- Information management and information technology security awareness to mitigate cybersecurity threats was enhanced via numerous training events and activities (seven events were held with a total of 868+ participants, plus a total of 23 CIO messages and Broadcast News articles were sent to employees).
- The third year of the multi-year IT Security Strategic Plan was completed, resulting in an updated suite of IT security standards that were widely communicated to users in PHAC.
- The Guelph Consolidation Project was completed, providing growth space for PHAC and Health Canada.
- Modernization of the harassment and workplace violence prevention and resolution mechanisms and tools was completed in light of upcoming changes to the Occupational Health and Safety Regulations. A review of the suite of occupational health and safety programs was also initiated to include psychological safety considerations in light of recent changes to the Canada Labour Code (Bill C-65).
PHAC worked closely with other government departments to coordinate efforts to ensure essential employees and critical services were available to protect the health, safety and well-being of Canadians. Efforts were made to ensure that employees have a safe workplace as well as the tools they need for working remotely. These preparedness activities helped better position PHAC for the delivery of critical services and commitments during the COVID-19 pandemic. Accommodation requirements and facilities management needs were addressed in a timely manner. Initial planning for office and warehousing needs/pressures was carried out. Enhanced cleaning services/measures were also provided, as needed, to ensure employees’ safety, and office equipment was delivered to employees’ homes who were performing critical functions with a Duty to Accommodate.
Throughout the COVID-19 outbreak, employees have been kept fully apprised of guidance and announcements from public health authorities, the Treasury Board Secretariat and the Public Service Occupational Health Program. Information has been disseminated using a variety of tools and platforms including email messages from the Deputy Heads, Chief Information Officer and Director General of Human Resources and through a new infoCOVID email bulletin. A series of new web-based digital channels were also introduced to help ensure that employees had multiple touchpoints from which to access critical information. These new channels include an employee page on Canada.ca, a closed employee Facebook group and an employee Twitter account.
Enhancing the use of data and improving information sharing
Data and information sharing is integral to informing evidence-based programing and policy. In 2019-20, PHAC finalized its Data Strategy, which centers on PHAC’s ability to collect, generate, secure, manage, access, and analyze data in order to create a clear and consistent approach to data management that supports public health decision-making and action. This strategy enables PHAC to protect and promote the health of Canadians by leveraging data innovation, modern technical capacity, and timely and quality public health data. It also aims to champion and highlight in-house expertise, and provide staff with tools and opportunities to enhance their data skills as needed through communities of practice and training. A five-year implementation plan that is grounded in strengthening internal capacity and leveraging data to transform public health guides the forward work of the strategy.
In 2019-20, PHAC also played a key role in coordinating and sharing information to support public health measures. PHAC provided evidence to support national public health responses by developing Technical Annexes to the Multi-Lateral Information Sharing Agreement, which will provide guidance on information that is shared between PHAC and the province and territories. The portion which highlights the data to be shared for commonly addressed purposes in surveillance was completed and sent for review by partners. A face-to-face meeting between federal, provincial and territorial partners was also held to gather information on priorities and challenges that would inform the Technical Annexes.
Pay system stabilization
In 2019–20, PHAC’s backlog of cases decreased from 6,019 on April 1, 2019, to 3,426 on March 31, 2020. This is largely attributable to the PHAC and Health Canada internal pay team, which was supported by a one-time funding of over $1 million. PHAC led the Public Service in improving its “on-time” performance for staffing actions affecting pay from around 30% in 2018-19 to 90% in 2019-20. This has led to the creation of far fewer new pay issues.
Informing Canadians about public health issues
PHAC continued to provide Canadians with access to the information they needed to take action on their health and safety. The Agency developed numerous initiatives to engage and inform Canadians through various digital and traditional communications methods:
- Lyme disease public awareness campaign.
- Childhood vaccination advertising campaign.
- CPHO Spotlight on Antimicrobial Resistance.
- Public awareness campaign on opioids, problematic substance use and stigma.
Since the start of the COVID-19 outbreak, PHAC has provided Canadians and health care providers with the timely, trusted and evidence-based information they need to protect themselves, their families, their communities and their businesses. PHAC has used various channels to provide information and updates to Canadians, including:
- Dedicated Canada.ca/coronavirus website, also linking to PHAC and Health Canada pages on the COVID-19 response – had more than 61 million visits between its launch on January 16, 2020, and March 31, 2020.
- Regular briefings to the media – PHAC held 34 briefings and press conferences from January 20, 2020, to March 31, 2020.
- Daily Covid-19 technical briefing with Parliamentarians – PHAC hosted 16 briefings in March 2020, in partnership with over 15 other federal departments and agencies. The Agency provided answers on topics such as the Quarantine Act, PPE, medical supplies, social distancing, contact tracing and testing.
- Meetings with Canadian stakeholders – PHAC led 28 bilateral and multilateral meetings with various health, allied health, economic, childcare, agricultural, and critical infrastructure stakeholders, providing situational updates and technical expertise, from January 30, 2020 to March 31, 2020.
- A toll-free information line [1-833-784-4397] with interpretation service available in 200+ languages open from 7:00 a.m. to midnight, 7 days a week.
- Social media.
- TV, radio, print and digital advertising.
- Nation-wide mail-outs – 15.5 million distributed, reaching every household in Canada, starting in March 2020.
Building a results-based management culture
In the latest annual Management Accountability Framework assessment, PHAC received a very positive assessment for Results Management, which includes the use of performance information. This positive assessment is due, in part, to the numerous Agency-wide initiatives undertaken to further advance and sustain a Results-Based Management (RBM) culture within PHAC. For instance, the use of a robust governance that oversaw RBM implementation and review of performance information; upgrades to the PHAC RBM GCPedia website which is recognized as a best practice in government; a new RBM Community of Practice, which has since expanded to include participants from other departments; a pilot project to PHAC’s Data Strategy initiating the Data Management System for Performance Measurement Project; and delivery of in person and virtual RBM Awareness Sessions to managers and employees.
Innovation and Experimentation
In 2019-20, PHAC implemented an Accessible and Inclusive Meeting Space (AIMS) pilot project in Ottawa. The purpose of this project was to design and implement a fully accessible and inclusive meeting room in order to bring awareness to all employees, in terms of the restrictions persons with disabilities face on a daily basis. The ultimate goal is to reduce discrimination and harassment, allowing for a new culture in the workplace. In order to facilitate this, several state of the art elements were used including, technology, lighting, signage, furniture, finishes, and a barrier-free design. This pilot project will be the basis for future AIMS meeting rooms across the country.
| 2019–20 Main Estimates |
2019–20 Planned spending |
2019–20 Total authorities available for use |
2019–20 Actual spending (authorities used)* |
2019–20 Difference (Actual spending minus Planned spending) |
|---|---|---|---|---|
| 99,299,635 | 99,299,635 | 114,197,336 | 113,201,286 | 13,901,651 |
Authorities available for use increased during the fiscal year mainly due to funding approved in response to the COVID-19 pandemic. Actual spending varied from planned spending primarily due to the new funding received.
| 2019–20 Planned full-time equivalents |
2019–20 Actual full-time equivalents |
2019–20 Difference (Actual full-time equivalents minus Planned full-time equivalents) |
|---|---|---|
| 626 | 333 | (293) |
Actual full-time equivalents varied from planned full-time equivalents primarily due to the annual transfer of resources from PHAC to Health Canada under the Health Portfolio Shared Services Partnership Agreement.
Analysis of trends in spending and human resources
Actual expenditures
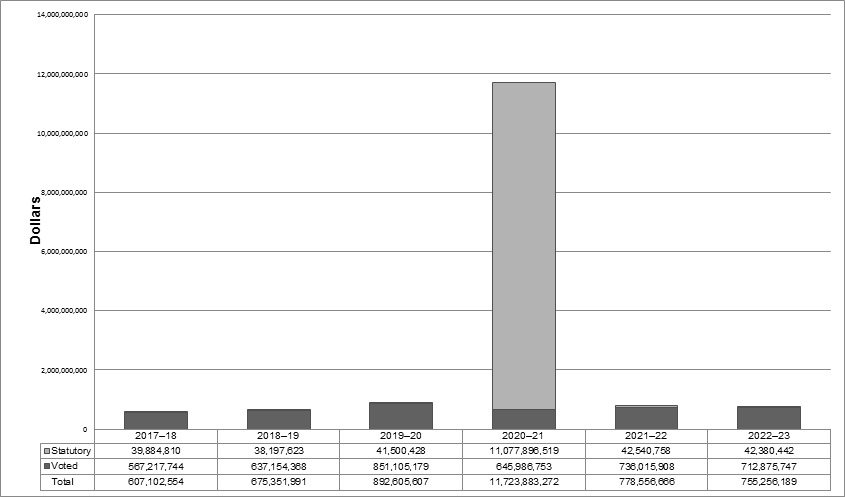
Figure - Text description
| Fiscal year | Total | Voted | Statutory |
|---|---|---|---|
| 2017–18 | 607,102,554 | 567,217,744 | 39,884,810 |
| 2018–19 | 675,351,991 | 637,154,368 | 38,197,623 |
| 2019–20 | 892,605,607 | 851,105,179 | 41,500,428 |
| 2020–21 | 11,723,883,272 | 645,986,753 | 11,077,896,519 |
| 2021–22 | 778,556,666 | 736,015,908 | 42,540,758 |
| 2022–23 | 755,256,189 | 712,875,747 | 42,380,442 |
The changes in spending from 2018–19 to 2019–20 are primarily due to new funding received to respond the COVID-19 pandemic.
| Core Responsibilities and Internal Services | 2019–20 Main Estimates |
2019–20 Planned spending |
2020–21 Planned spending |
2021–22 Planned spending |
2019–20 Total authorities available for use |
2019–20 Actual spending (authorities used) |
2018–19 Actual spending (authorities used) |
2017–18 Actual spending (authorities used) |
|---|---|---|---|---|---|---|---|---|
| 1. Health Promotion and Disease Prevention | 257,822,279 | 257,822,279 | 289,862,972 | 274,725,176 | 278,546,895 | 273,405,685 | 318,391,163 | 239,450,960 |
| 2. Infectious Disease Prevention and Control | 207,886,062 | 207,886,062 | 6,194,078,142 | 273,924,740 | 261,470,040 | 257,498,145 | 199,658,422 | 189,906,141 |
| 3. Health Security | 52,331,185 | 52,331,185 | 5,069,909,224 | 111,037,052 | 249,021,203 | 248,500,491 | 55,577,234 | 78,982,234 |
| Budget Implementation vote – unallocated authorities | Not applicable | Not applicable | Not applicable | Not applicable | 361,734 | Not applicable | Not applicable | Not applicable |
| Subtotal | 518,039,526 | 518,039,526 | 11,553,850,338 | 659,686,968 | 789,399,872 | 779,404,321 | 573,626,819 | 508,339,335 |
| Internal Services | 99,299,635 | 99,299,635 | 170,032,934 | 118,869,698 | 114,197,336 | 113,201,286 | 101,725,172 | 98,763,219 |
| Total | 617,339,161 | 617,339,161 | 11,723,883,272 | 778,556,666 | 903,597,208 | 892,605,607 | 675,351,991 | 607,102,554 |
|
||||||||
The increase in actual spending from 2018–19 to 2019–20 is primarily due to new funding received to respond to the COVID-19 pandemic. The $361,734 represents the frozen allotment that has not yet been distributed to a specific authority. Since the frozen allotment has not been distributed to a specific authority, it has also not been distributed to a specific Core Responsibility.
| Core responsibilities and Internal Services | 2019–20 Actual gross spending* |
2019–20 Actual gross spending for specified purpose accounts |
2019–20 Actual revenues netted against expenditures |
2019–20 Actual net spending (authorities used) |
|---|---|---|---|---|
| 1. Health Promotion and Chronic Disease Prevention | 273,405,686 | 0 | 0 | 273,405,686 |
| 2. Infectious Disease Prevention and Control | 257,498,145 | 0 | 0 | 257,498,145 |
| 3. Health Security | 249,156,384 | 0 | (655,894) | 248,500,490 |
| Subtotal | 780,060,215 | 0 | (655,894) | 779,404,321 |
| Internal Services | 113,201,286 | 0 | 0 | 113,201,286 |
| Total | 893,261,501 | 0 | (655,894) | 892,605,607 |
Actual human resources
| Core responsibilities and Internal Services | 2017–18 Actual full-time equivalents | 2018–19 Actual full-time equivalents | 2019–20 Planned full-time equivalents |
2019–20 Actual full-time equivalents | 2020–21 Planned full-time equivalents | 2021–22 Planned full-time equivalents |
|---|---|---|---|---|---|---|
| 1. Health Promotion and Chronic Disease Prevention | 439 | 476 | 484 | 524 | 563 | 539 |
| 2. Infectious Disease Prevention and Control | 958 | 982 | 1,008 | 1,054 | 1,242 | 1,056 |
| 3. Health Security | 372 | 354 | 381 | 385 | 657 | 365 |
| Subtotal | 1,768 | 1,812 | 1,873 | 1,963 | 2,462 | 1,960 |
| Internal Services | 307 | 322 | 626 | 333 | 671 | 654 |
| Total | 2,075 | 2,134 | 2,499 | 2,296 | 3,133 | 2,614 |
|
||||||
Actual full-time equivalents varied from planned full-time equivalents primarily due to the annual transfer of resources from PHAC to Health Canada under the Health Portfolio Shared Services Partnership Agreement.
Expenditures by vote
For information on PHAC’s organizational voted and statutory expenditures, consult the Public Accounts of Canada 2019-2020.
Government of Canada spending and activities
Information on the alignment of PHAC’s spending with the Government of Canada’s spending and activities is available in the GC InfoBase.
Financial statements and financial statements highlights
Financial statements
PHAC’s financial statements (unaudited) for the year ended March 31, 2020, are available on PHAC’s website.
Financial statements highlights
Condensed Statement of Financial Position (unaudited) as of March 31, 2020 (dollars)
| Financial information | 2019–20 Planned results | 2019–20 Actual results | 2018–19 Actual results | Difference (2019–20 Actual results minus 2019–20 Planned results) |
Difference (2019–20 Actual results minus 2018–19 Actual results) |
|---|---|---|---|---|---|
| Total expenses | 653,521,577 | 713,951,587 | 701,984,958 | 60,430,010 | 11,966,629 |
| Total revenues | 13,984,973 | 13,101,200 | 13,263,174 | (883,773) | (161,974) |
| Net cost of operations before government funding and transfers | 639,536,604 | 700,850,387 | 688,721,784 | 61,313,783 | 12,128,603 |
| Financial Information | 2019–20 | 2018–19 | Difference (2019–20 minus 2018–19) |
|---|---|---|---|
| Total net liabilities | 191,167,217 | 104,519,903 | 86,647,314 |
| Total net financial assets | 165,968,350 | 81,949,325 | 84,019,025 |
| Departmental net debt | 25,198,868 | 22,570,579 | 2,628,289 |
| Total non-financial assets | 297,788,321 | 95,431,613 | 202,356,708 |
| Departmental net financial position | 272,589,453 | 72,861,034 | 199,728,419 |
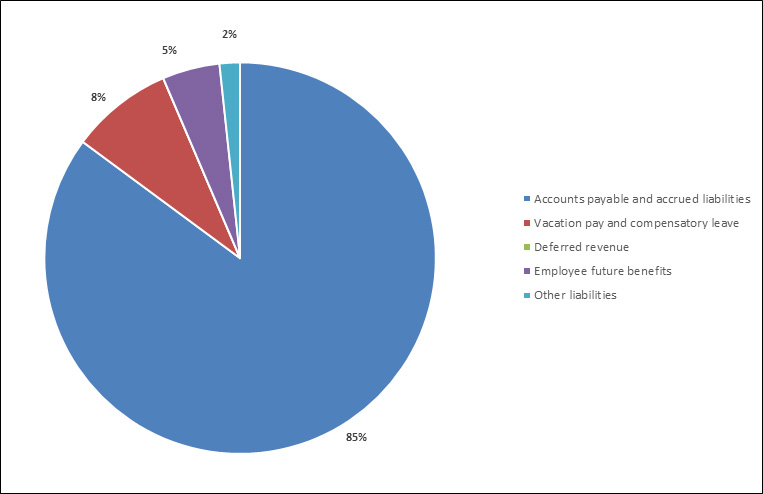
Total liabilities were $191,167,217, an increase of $86,647,314 (83%) over the previous year’s total. The increase is primarily due to an increase in accounts payable and accrued liabilities, which accounted for $83,921,874 (97%) of the variance year-over-year.
Of the total liabilities:
- Accounts payable and accrued liabilities represented $162,737,041 (85%).
- Vacation pay and compensatory leave represented $16,144,920 (8%).
- Employee future benefits represented $9,056,575 (5%).
- Other liabilities represented $3,228,641 (2%).

Total assets were $463,756,670, an increase of $286,375,732 (161%) over the previous year’s total of $177,380,938. This variance is primarily due to an increase in prepaid expenses of $210,091,048 and amounts due from the Consolidated Revenue Fund $69,578,195, representing 73% and 24% of the year-over-year variance, respectively.
Of the total assets:
- Prepaid expenses represented $210,091,048 (45%).
- Due from Consolidated Revenue Fund represented $146,033,600 (31%).
- Tangible capital assets represented $87,697,272 (19%).
- Accounts receivable and advances represented $19,934,750 (4%).
Additional Information
Organizational profile
Appropriate minister: The Honourable Patty Hajdu, P.C., M.P
Institutional head: Kristina Namiesniowski, President
Ministerial portfolio: Health
Enabling instruments: Public Health Agency of Canada Act, Department of Health Act, Emergency Management Act, Quarantine Act, Human Pathogens and Toxins Act, Health of Animals Act, Federal Framework on Lyme Disease Act, and the Federal Framework for Suicide Prevention Act.
Year of incorporation / commencement: 2004
Other: In 2012, the Deputy Heads of Health Canada and PHAC signed a Shared Services Partnership Framework Agreement. Under this agreement, the two organizations consolidated several common functions: emergency management, international affairs, internal audit services, evaluation services, human resources, internal financial services, real property, communications, information management/information technology, and security.
Raison d’être, mandate and role: who we are and what we do
“Raison d’être, mandate and role: who we are and what we do” is available on PHAC’s website.
For more information on PHAC’s organizational mandate letter commitments, see the “Minister’s mandate letter.”
Reporting framework
PHAC's Departmental Results Framework and Program Inventory of record for 2019–20 are shown below.
Departmental Results Framework
- Core Responsibility 1: Health Promotion and Chronic Disease Prevention
- Result 1.1 Canadians have improved physical and mental health.
- Indicator: % of low-income children in very good or excellent health
- Indicator: % of population who have high psychological well-being
- Result 1.2 Canadians have improved health behaviours.
- Indicator: % increase in average minutes/day of physical activity among adults
- Indicator: % increase in average minutes/day of physical activity among children/youth
- Result 1.3 Chronic diseases are prevented.
- Indicator: % increase in years lived in good health by seniors
- Indicator: Rate of new diabetes cases among Canadians
- Indicator: % of adults who are obese
- Indicator: % of children and youth who are obese
- Program Inventory
- Program: Health Promotion
- Program: Chronic Disease Prevention
- Program: Evidence for Health Promotion, and Chronic Disease and Injury Prevention
- Result 1.1 Canadians have improved physical and mental health.
- Core Responsibility 2: Infectious Disease Prevention and Control
- Result 2.1 Infectious diseases are prevented and controlled.
- Indicator: % of 2 year old children who have received all recommended vaccinations
- Indicator: Proportion of national vaccination coverage goals met for children by 2 years of age
- Indicator: Rate per 100,000 of new diagnosed cases of Human Immunodeficiency Virus (HIV)
- Indicator: Rate of a key antimicrobial resistant infection identified among people in hospitals
- Result 2.2 Infectious disease outbreaks and threats are prepared for and responded to.
- Indicator: % of foodborne illness outbreaks responded to within 24 hours of notification
- Indicator: % of new pathogens of international concern that Canada has the capacity to accurately test for
- Program Inventory
- Program: Laboratory Science Leadership and Services
- Program: Communicable Diseases and Infection Control
- Program: Vaccination
- Program: Foodborne and Zoonotic Diseases
- Result 2.1 Infectious diseases are prevented and controlled.
- Core Responsibility 3: Health Security
- Result 3.1 Public health events and emergencies are prepared for and responded to effectively.
- Indicator: Canada’s readiness to respond to public health events and emergencies as assessed independently by the World Health Organization
- Indicator: % of provincial and territorial requests for assistance responded to within negotiated timelines
- Result 3.2 Public health risks associated with the use of pathogens and toxins are reduced.
- Indicator: % of compliance issues in Canadian laboratories successfully responded to within established timelines
- Result 3.3 Public health risks associated with travel are reduced.
- Indicator: Canada’s capacity for effective public health response at designated points of entry into Canada
- Indicator: % of inspected passenger transportation operators that meet public health requirements
- Program Inventory
- Program: Emergency Preparedness and Response
- Program: Biosecurity
- Program: Border and Travel Health
- Result 3.1 Public health events and emergencies are prepared for and responded to effectively.
- Internal Services
Supporting information on the Program Inventory
Financial, human resources and performance information for PHAC’s Program Inventory is available in the GC InfoBase.
Supplementary information tables
The following supplementary information tables are available on PHAC’s website:
- Departmental Sustainable Development Strategy.
- Details on transfer payment programs of $5 million or more.
- Gender-based analysis plus.
- Horizontal initiatives.
- Response to parliamentary committees and external audits.
Federal tax expenditures
The tax system can be used to achieve public policy objectives through the application of special measures such as low tax rates, exemptions, deductions, deferrals and credits. The Department of Finance Canada publishes cost estimates and projections for these measures each year in the Report on Federal Tax Expenditures. This report also provides detailed background information on tax expenditures, including descriptions, objectives, historical information and references to related federal spending programs. The tax measures presented in this report are the responsibility of the Minister of Finance.
Organizational contact information
Anna Romano
Vice-President, Strategic Policy and Planning Branch
Public Health Agency of Canada
130 Colonnade Road
Ottawa, Ontario K1A 0K9
Canada
Email: anna.romano@canada.ca
Appendix: definitions
- appropriation
- Any authority of Parliament to pay money out of the Consolidated Revenue Fund.
- budgetary expenditures
- Operating and capital expenditures; transfer payments to other levels of government, organizations or individuals; and payments to Crown corporations.
- core responsibility
- An enduring function or role performed by a department. The intentions of the department with respect to a core responsibility are reflected in one or more related departmental results that the department seeks to contribute to or influence.
- Departmental Plan
- A report on the plans and expected performance of an appropriated department over a 3-year period. Departmental Plans are usually tabled in Parliament each spring.
- departmental priority
- A plan or project that a department has chosen to focus and report on during the planning period. Priorities represent the things that are most important or what must be done first to support the achievement of the desired departmental results.
- departmental result
- A consequence or outcome that a department seeks to achieve. A departmental result is often outside departments’ immediate control, but it should be influenced by program-level outcomes.
- departmental result indicator
- A quantitative measure of progress on a departmental result.
- departmental results framework
- A framework that connects the department’s core responsibilities to its departmental results and departmental result indicators.
- Departmental Results Report
- A report on a department’s actual accomplishments against the plans, priorities and expected results set out in the corresponding Departmental Plan.
- experimentation
- The conducting of activities that seek to first explore, then test and compare the effects and impacts of policies and interventions in order to inform evidence-based decision-making, and improve outcomes for Canadians, by learning what works, for whom and in what circumstances. Experimentation is related to, but distinct from innovation (the trying of new things), because it involves a rigorous comparison of results. For example, using a new website to communicate with Canadians can be an innovation; systematically testing the new website against existing outreach tools or an old website to see which one leads to more engagement, is experimentation.
- full-time equivalent
- A measure of the extent to which an employee represents a full person-year charge against a departmental budget. For a particular position, the full-time equivalent figure is the ratio of number of hours the person actually works divided by the standard number of hours set out in the person’s collective agreement.
- gender-based analysis plus (GBA+
- An analytical process used to assess how diverse groups of women, men and gender-diverse people experience policies, programs and services based on multiple factors including race ethnicity, religion, age, and mental or physical disability.
- government-wide priorities
- For the purpose of the 2019–20 Departmental Results Report, those high-level themes outlining the government’s agenda in the 2019 Speech from the Throne, namely: Fighting climate change; Strengthening the Middle Class; Walking the road of reconciliation; Keeping Canadians safe and healthy; and Positioning Canada for success in an uncertain world.
- horizontal initiative
- An initiative where two or more federal organizations are given funding to pursue a shared outcome, often linked to a government priority.
- non-budgetary expenditures
- Net outlays and receipts related to loans, investments and advances, which change the composition of the financial assets of the Government of Canada.
- performance
- What an organization did with its resources to achieve its results, how well those results compare to what the organization intended to achieve, and how well lessons learned have been identified.
- performance indicator
- A qualitative or quantitative means of measuring an output or outcome, with the intention of gauging the performance of an organization, program, policy or initiative respecting expected results.
- performance reporting
- The process of communicating evidence-based performance information. Performance reporting supports decision making, accountability and transparency.
- plan
- The articulation of strategic choices, which provides information on how an organization intends to achieve its priorities and associated results. Generally, a plan will explain the logic behind the strategies chosen and tend to focus on actions that lead to the expected result.
- planned spending
- For Departmental Plans and Departmental Results Reports, planned spending refers to those amounts presented in Main Estimates. A department is expected to be aware of the authorities that it has sought and received. The determination of planned spending is a departmental responsibility, and departments must be able to defend the expenditure and accrual numbers presented in their Departmental Plans and Departmental Results Reports.
- program
- Individual or groups of services, activities or combinations thereof that are managed together within the department and focus on a specific set of outputs, outcomes or service levels.
- program inventory
- Identifies all the department’s programs and describes how resources are organized to contribute to the department’s core responsibilities and results.
- result
- A consequence attributed, in part, to an organization, policy, program or initiative. Results are not within the control of a single organization, policy, program or initiative; instead they are within the area of the organization’s influence.
- statutory expenditures
- Expenditures that Parliament has approved through legislation other than appropriation acts. The legislation sets out the purpose of the expenditures and the terms and conditions under which they may be made.
- target
- A measurable performance or success level that an organization, program or initiative plans to achieve within a specified time period. Targets can be either quantitative or qualitative.
- voted expenditures
- Expenditures that Parliament approves annually through an appropriation act. The vote wording becomes the governing conditions under which these expenditures may be made.
Footnotes
- Footnote 1
-
In the Health Portfolio, we refer to sex and gender-based analysis plus (SGBA+) because of the important roles that both sex and gender play in health.
- Footnote 2
-
Individuals who can maintain undetectable viral loads have effectively no risk of transmitting HIV to their sexual partner.
- Footnote 3
-
This exhibit showcases the fascinating world of ticks in a fun and educational manner. It provides practical information and resources for parents and other accompanying adults to talk with children about ticks, tick bite prevention and tick-borne diseases.
- Footnote 4
-
Zoonoses are defined as diseases that can be transmitted from animals and insects to humans.
- Footnote 5
-
Human pathogens classified as Risk Group 2-4, or toxins listed in Schedule 1 of the HPTA, require a licence, issued by PHAC.
- Footnote 6
-
Risk Group 2 pathogens pose a moderate risk to the health of an individual and a low risk to public health – they are able to cause serious disease in a human but unlikely to do so. Risk Group 3 pathogens pose a high risk to the health of an individual and a low risk to public health – they are able to cause serious disease in a human.
Page details
- Date modified: